Epoprostenol
 | |
 | |
| Names | |
|---|---|
| Pronunciation | e" poe pros' ten nol |
| Trade names | Flolan, Veletri, others |
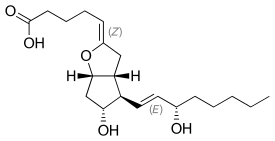
| Other names | Prostacyclin, prostaglandin I2 (PGI2) |
IUPAC name
| |
| Clinical data | |
| Drug class | Prostaglandin[1] |
| Main uses | Pulmonary arterial hypertension, ARDS[2] |
| Side effects | Headache, dizziness, nausea, muscle pain, flushing, fast heart rate, low blood pressure[2] |
| Pregnancy category |
|
| External links | |
| AHFS/Drugs.com | Monograph |
| Legal | |
| License data | |
| Legal status |
|
| Pharmacokinetics | |
| Elimination half-life | 42 seconds |
| Chemical and physical data | |
| Formula | C20H32O5 |
| Molar mass | 352.471 g·mol−1 |
| 3D model (JSmol) | |
SMILES
| |
InChI
| |
Epoprostenol, also known as prostacyclin, is a medication and naturally occurring substance in the human body.[3] As a medication it used to treat pulmonary arterial hypertension and acute respiratory distress syndrome (ARDS).[2] It may also be used during dialysis when heparin cannot be used to prevent platelet aggregation.[1] It may be given by continuous injection into a vein or inhaled.[2][1]
Common side effects include headache, dizziness, nausea, muscle pain, flushing, fast heart rate, and low blood pressure.[2] Other side effects may include bleeding.[2] There is no evidence of harm in pregnancy, but such use has not been well studied.[4] It is a prostaglandin and works by blocking platelet aggregation and dilating blood vessels.[1]
Epoprostenol was approved for medical use in the United States in 1995.[2] It is available as a generic medication.[1] In the United Kingdom 1.5 mg costs the NHS about £45 as of 2021.[1] In the United States this amount costs about 50 USD.[5]
Medical uses
It is used to treat pulmonary arterial hypertension (PAH).[6][7] Specifically, epoprostenol is given to people with class II or class IV PAH.
Side effects
.png.webp)
The side effects of this medication , prostacyclin, are the following (this is not an exhaustive list):[8]
- Prolonged bleeding
- Rapid weight gain
- Redness of face, neck, arms, upper chest
- Blurred vision
- Chest congestion
- Chest pain
- Chills
Mechanism of action
| Prostacyclin effect | Mechanism | Cellular response | |
|---|---|---|---|
| Classical functions |
Vessel tone | ↑cAMP, ↓ET-1 ↓Ca2+, ↑K+ |
↓SMC proliferation ↑Vasodilation |
| Antiproliferative | ↑cAMP ↑PPARgamma |
↓Fibroblast growth ↑Apoptosis | |
| Antithrombotic | ↓Thromboxane-A2 ↓PDGF |
↓Platelet aggregation ↓Platelet adherence to vessel wall | |
| Novel functions |
Antiinflammatory | ↓IL-1, IL-6 ↑IL-10 |
↓Proinflammatory cytokines ↑Antiinflammatory cytokines |
| Antimitogenic | ↓VEGF ↓TGF-β |
↓Angiogenesis ↑ECM remodeling | |
Prostacyclin (PGI2) is released by healthy endothelial cells and performs its function through a paracrine signaling cascade that involves G protein-coupled receptors on nearby platelets and endothelial cells. The platelet Gs protein-coupled receptor (prostacyclin receptor) is activated when it binds to PGI2. This activation, in turn, signals adenylyl cyclase to produce cAMP. cAMP goes on to inhibit any undue platelet activation (in order to promote circulation) and also counteracts any increase in cytosolic calcium levels that would result from thromboxane A2 (TXA2) binding (leading to platelet activation and subsequent coagulation). PGI2 also binds to endothelial prostacyclin receptors, and in the same manner, raises cAMP levels in the cytosol. This cAMP then goes on to activate protein kinase A (PKA). PKA then continues the cascade by promoting the phosphorylation of the myosin light chain kinase, which inhibits it and leads to smooth muscle relaxation and vasodilation. It can be noted that PGI2 and TXA2 work as physiological antagonists.
Function
Prostacyclin (PGI2) chiefly prevents formation of the platelet plug involved in primary hemostasis (a part of blood clot formation). It does this by inhibiting platelet activation.[9] It is also an effective vasodilator. Prostacyclin's interactions contrast with those of thromboxane (TXA2), another eicosanoid. These strongly suggest a mechanism of cardiovascular homeostasis between these two hormones in relation to vascular damage.
Degradation
Prostacyclin, which has a half-life of 42 seconds,[10] is broken down into 6-keto-PGF1, which is a much weaker vasodilator.
Pharmacology
Synthetic prostacyclin analogues (iloprost, cisaprost) are used intravenously, subcutaneously or by inhalation:
- as a vasodilator in severe Raynaud's phenomenon or ischemia of a limb;
- in pulmonary hypertension.
- in primary pulmonary hypertension (PPH)
The production of prostacyclin is inhibited by the action of NSAIDs on cyclooxygenase enzymes COX1 and COX2. These convert arachidonic acid to prostaglandin H2 (PGH2), the immediate precursor of prostacyclin. Since thromboxane (an eicosanoid stimulator of platelet aggregation) is also downstream of COX enzymes, one might think that the effect of NSAIDs would act to balance. However, prostacyclin concentrations recover much faster than thromboxane levels, so aspirin administration initially has little to no effect but eventually prevents platelet aggregation (the effect of prostaglandins predominates as they are regenerated). This is explained by understanding the cells that produce each molecule, TXA2 and PGI2. Since PGI2 is primarily produced in a nucleated endothelial cell, the COX inhibition by NSAID can be overcome with time by increased COX gene activation and subsequent production of more COX enzymes to catalyze the formation of PGI2. In contrast, TXA2 is released primarily by anucleated platelets, which are unable to respond to NSAID COX inhibition with additional transcription of the COX gene because they lack DNA material necessary to perform such a task. This allows NSAIDs to result in PGI2 dominance that promotes circulation and retards thrombosis.
In patients with pulmonary hypertension, inhaled epoprostenol reduces pulmonary pressure, and improves right ventricular stroke volume in patients undergoing cardiac surgery. A dose of 60 μg is hemodynamically safe, and its effect is completely reversed after 25 minutes. No evidence of platelet dysfunction or an increase in surgical bleeding after administration of inhaled epoprostenol has been found.[11] The drug has been known to cause flushing, headaches and hypotension.[12]
Synthesis
Biosynthesis

Prostacyclin is produced in endothelial cells, which line the walls of arteries and veins,[13] from prostaglandin H2 (PGH2) by the action of the enzyme prostacyclin synthase. Although prostacyclin is considered an independent mediator, it is called PGI2 (prostaglandin I2) in eicosanoid nomenclature, and is a member of the prostanoids (together with the prostaglandins and thromboxane). PGI2, derived primarily from COX-2 in humans, is the major arachidonate metabolite released from the vascular endothelium. This is a controversial point, some assign COX 1 as the major prostacyclin producing cyclooxygenase in the endothelial cells of the blood vessels. [14]
The series-3 prostaglandin PGH3 also follows the prostacyclin synthase pathway, yielding another prostacyclin, PGI3.[15] The unqualified term 'prostacyclin' usually refers to PGI2. PGI2 is derived from the ω-6 arachidonic acid. PGI3 is derived from the ω-3 EPA.
Artificial synthesis
Prostacyclin can be synthesized from the methyl ester of prostaglandin F2α.[16] After its synthesis, the drug is reconstituted in saline and glycerin.[17]
History
During the 1960s, a UK research team, headed by Professor John Vane, began to explore the role of prostaglandins in anaphylaxis and respiratory diseases. Working with a team from the Royal College of Surgeons, Vane discovered that aspirin and other oral anti-inflammatory drugs work by inhibiting the synthesis of prostaglandins. This critical finding opened the door to a broader understanding of the role of prostaglandins in the body.
A team at The Wellcome Foundation led by Salvador Moncada had identified a lipid mediator they called "PG-X," which inhibits platelet aggregation. PG-X, later known as prostacyclin, is 30 times more potent than any other then-known anti-aggregatory agent.
In 1976, Vane and fellow researchers Salvador Moncada, Ryszard Gryglewski, and Stuart Bunting published the first paper on prostacyclin in Nature.[18] The collaboration produced a synthesized molecule, which was named epoprostenol. But, as with native prostacyclin, the epoprostenol molecule is unstable in solution and prone to rapid degradation. This presented a challenge for both in vitro experiments and clinical applications.
To overcome this challenge, the research team that discovered prostacyclin continued the research. The research team synthesized nearly 1,000 analogues.
Society and culture
Brands
| Brands[19] | |||
|---|---|---|---|
| Flolan (epoprostenol) for Injection |
Continuously infused | 2 ng/kg/min to start, increased by 2 ng/kg/min every 15 minutes or longer until suitable efficacy/tolerability balance is achieved | Class III Class IV |
| Veletri (epoprostenol) for Injection |
Continuously infused | 2 ng/kg/min to start, increased by 2 ng/kg/min every 15 minutes or longer until suitable efficacy/tolerability balance is achieved | Class III Class IV |
| Remodulin SC§ (treprostinil sodium) Injection |
Continuously infused | 1.25 ng/kg/min to start, increased by up to 1.25 ng/kg/min per week for 4 weeks, then up to 2.5 ng/kg/min per week until
suitable efficacy/tolerability balance is achieved |
Class II Class III Class IV |
| Ventavis (iloprost) Inhalation Solution |
Inhaled 6–9 times daily | 2.5 μg 6–9 times daily to start, increased to 5.0 μg 6–9 times daily if well tolerated | Class III Class IV |
References
- 1 2 3 4 5 6 BNF 81: March-September 2021. BMJ Group and the Pharmaceutical Press. 2021. p. 124. ISBN 978-0857114105.
- 1 2 3 4 5 6 7 "Epoprostenol Monograph for Professionals". Drugs.com. Archived from the original on 4 January 2022. Retrieved 15 December 2021.
- ↑ "Prostacyclin Analogs". LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. National Institute of Diabetes and Digestive and Kidney Diseases. 2012. Archived from the original on 8 May 2021. Retrieved 15 December 2021.
- ↑ "Epoprostenol Use During Pregnancy". Drugs.com. Archived from the original on 4 January 2022. Retrieved 15 December 2021.
- ↑ "Epoprostenol Prices, Coupons & Patient Assistance Programs". Drugs.com. Archived from the original on 4 January 2022. Retrieved 15 December 2021.
- ↑ "Epoprostenol Sodium Monograph for Professionals". Drugs.com. AHFS. 6 April 2020. Archived from the original on 26 October 2020. Retrieved 22 October 2020.
- ↑ "Flolan- epoprostenol sodium injection, powder, lyophilized, for solution Diluent- water solution". DailyMed. 15 November 2019. Archived from the original on 26 October 2020. Retrieved 22 October 2020.
- ↑ "Epoprostenol Side Effects: Common, Severe, Long Term". Drugs.com. Archived from the original on 30 October 2020. Retrieved 4 November 2021.
- ↑ Pathologic Basis of Disease, Robbins and Cotran, 8th ed. Saunders Philadelphia 2010
- ↑ Cawello, W; Schweer, H; Müller, R; Bonn, R; Seyberth, HW (1994). "Metabolism and pharmacokinetics of prostaglandin E1 administered by intravenous infusion in human subjects". European Journal of Clinical Pharmacology. 46 (3): 275–7. doi:10.1007/BF00192562. PMID 8070511. S2CID 25410558.
- ↑ Haché, M; Denault, A; Bélisle, S; Robitaille, D; Couture, P; Sheridan, P; Pellerin, M; Babin, D; Noël, N; Guertin, MC; Martineau, R; Dupuis, J (Mar 2003). "Inhaled epoprostenol (prostacyclin) and pulmonary hypertension before cardiac surgery". The Journal of Thoracic and Cardiovascular Surgery. 125 (3): 642–9. doi:10.1067/mtc.2003.107. PMID 12658208.
- ↑ Nickson, C. (2015, October 28). Prostacyclin or Epoprostenol. Retrieved November 16, 2015, from http://lifeinthefastlane.com/ccc/prostacyclin-or-epoprostenol/ Archived 2019-02-15 at the Wayback Machine
- ↑ prostacyclin. (n.d.) Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. (2003). Retrieved November 17, 2015 from http://medical-dictionary.thefreedictionary.com/prostacyclin Archived 2019-05-17 at the Wayback Machine
- ↑ Kirkby, Nicholas S.; Lundberg, Martina H.; Harrington, Louise S.; Leadbeater, Philip D. M.; Milne, Ginger L.; Potter, Claire M. F.; Al-Yamani, Malak; Adeyemi, Oladipupo; Warner, Timothy D.; Mitchell, Jane A. (2012-10-23). "Cyclooxygenase-1, not cyclooxygenase-2, is responsible for physiological production of prostacyclin in the cardiovascular system". Proceedings of the National Academy of Sciences of the United States of America. 109 (43): 17597–17602. Bibcode:2012PNAS..10917597K. doi:10.1073/pnas.1209192109. ISSN 0027-8424. PMC 3491520. PMID 23045674.
- ↑ Fischer S, Weber PC (1985). "Thromboxane (TX)A3 and prostaglandin (PG)I3 are formed in man after dietary eicosapentaenoic acid: identification and quantification by capillary gas chromatography-electron impact mass spectrometry". Biomed. Mass Spectrom. 12 (9): 470–6. doi:10.1002/bms.1200120905. PMID 2996649.
- ↑ Johnson, Roy A.; Lincoln, Frank H.; Nidy, Eldon G.; Schneider, William P.; Thompson, John L.; Axen, Udo (1978). "Synthesis and characterization of prostacyclin, 6-ketoprostaglandin F1.alpha., prostaglandin I1, and prostaglandin I3". Journal of the American Chemical Society. 100 (24): 7690. doi:10.1021/ja00492a043.
- ↑ Nickson, C. (2015, October 28). Prostacyclin or Epoprostenol. Retrieved November 16, 2015, from http://lifeinthefastlane.com/ccc/prostacyclin-or-epoprostenol/ Archived 2019-02-15 at the Wayback Machine
- ↑ Moncada, S.; Gryglewski, R.; Bunting, S.; Vane, J. R. (21 October 1976). "An enzyme isolated from arteries transforms prostaglandin endoperoxides to an unstable substance that inhibits platelet aggregation". Nature. 263 (5579): 663–665. Bibcode:1976Natur.263..663M. doi:10.1038/263663a0. PMID 802670. S2CID 4279030.
- ↑ ^ REM_RefGuideWC_AUG07v.1
External links
| Identifiers: |
|---|
- "Epoprostenol". Drug Information Portal. U.S. National Library of Medicine. Archived from the original on 2021-04-27. Retrieved 2021-10-24.
- "Epoprostenol sodium". Drug Information Portal. U.S. National Library of Medicine. Archived from the original on 2021-06-25. Retrieved 2021-10-24.