Cardiac resynchronization therapy
| Cardiac resynchronization therapy | |
|---|---|
 | |
| ICD-9-CM | 00.51, 00.54 |
| MeSH | D058409 |
| eMedicine | 1839506-devices |
Cardiac resynchronisation therapy (CRT or CRT-P) is the insertion of electrodes in the left and right ventricles of the heart, as well as on occasion the right atrium, to treat heart failure by coordinating the function of the left and right ventricles via a pacemaker, a small device inserted into the interior chest wall.[1]
CRT is indicated in patients suffering from a low ejection fraction (typically <35%) indicating heart failure, where electrical activity has been compromised, with prolonged QRS duration to >120 ms.[2]
The insertion of electrodes into the ventricles is done under local anesthetic, with access to the ventricles most commonly via the subclavian vein, although access may be conferred from the axillary or cephalic veins. Right ventricular access is direct, while left ventricular access is conferred via the coronary sinus (CS).
CRT defibrillators (CRT-D) also incorporate the additional function of an implantable cardioverter-defibrillator (ICD), to quickly terminate an abnormally fast, life-threatening heart rhythm. CRT and CRT-D have become increasingly important therapeutic options for patients with moderate and severe heart failure.[3] CRT with pacemaker only is often termed "CRT-P" to help distinguish it from CRT with defibrillator (CRT-D).
Indications
The key indication for CRT is left bundle branch block (LBBB) of the heart, a cardiac abnormality leading to delayed left ventricular contraction. LBBB causes a QRS prolongation of >120 ms on the electrocardiogram, contributing to poor left ventricular coordination and reduced systolic function, thereby reduced ejection fraction (<35%). This reduction in ejection fraction is what we consider heart failure.[2]
Heart failure patients are generally considered if in class II or III heart failure, with current guidelines indicating CRT is inappropriate for class IV heart failure.[4]
Method
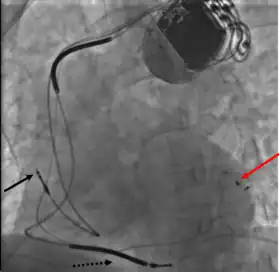
- Atrial lead at the right appendage
- Right ventricular lead at the apex
- Left ventricular lead through the coronary sinus.[5]
CRT requires the placement of an electrical device for biventricular pacing, along with placement of (at least) two pacing leads, to facilitate stable left ventricular and right ventricular pacing. For all elements, the first stage of the process is local anaesthetic followed by incision to allow for approach from the appropriate vein. From here, the leads and device can be inserted.[1]
Right ventricular lead placement
A venipuncture is made, and a guide wire inserted into the vein, where it is guided, with use of real time X-ray imaging, through to the right ventricle. The guide wire is then used to assist in the placement of the electrode lead, which travels through the venous system into the right ventricle where the electrode is embedded.[1]
Left ventricular lead placement
This is generally performed subsequent to RV lead placement, with the RV lead providing a backup in case of accidental damage to the electric fibers of the heart, causing an asystolic event. As with the RV lead, a guide wire is first inserted, allowing for the insertion of a multi-delivery catheter. The catheter is subsequently maneuvered to the opening of the coronary sinus in the right atrium. From here a contrast media is injected, allowing the surgical team to obtain a coronary sinus phleobogram to direct the placement of the lead into the most suitable coronary vein.[1]
Once the phlebogram has been obtained, the multi-delivery catheter is used to guide in the lead, from the chosen vein of entry, into the right atrium, through the coronary sinus and into the relevant cardiac vein.[1]
Left ventricular lead placement is the most complicated and potentially hazardous element of the operation, due to the significant variability of coronary venous structure. Alterations in heart structure, fatty deposits, valves and natural variations all cause additional complications in the process of cannulation.[1]
Device placement
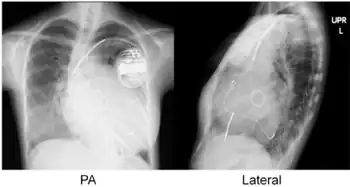
The device is inserted in a subcutaneous pocket created by the surgeon, the choice of left or right side of the chest wall is determined mainly by the patient's preference or location of preexisting device. The device, similar to that of a traditional pacemaker, is generally no larger than a pocket watch and has inserts for the electrode leads.[1]
Complications
Key complications include:[2]
- Dissection or perforation of coronary sinus which can in turn cause pericardial effusion
- Inability to cannulate coronary sinus (approximately 5% of patients)
- Myocardial perforation, pneumothorax and infection, all of which have an incidence of less than 1%
Technology
Several research papers[6][7] have proposed software platforms for planning and guiding the implantation of CRT devices. This research proposes using pre-operative images to characterize tissue and left ventricle activation to identify potential target regions for deploying the CRT leads.
References
- 1 2 3 4 5 6 7 "Cardiac Resynchronization Therapy Technique: Approach Considerations, Placement of Pacing Leads, Programming of Device". emedicine.medscape.com. Retrieved 2018-07-17.
- 1 2 3 Goldman, Lee (2012). Goldman-Cecil Medicine. USA: Elsevier Saunders. p. 379. ISBN 978-9996096563.
- ↑ Choi, Anthony J.; Thomas, Sunu S.; Singh, Jagmeet P. (2016). "Cardiac Resynchronization Therapy and Implantable Cardioverter Defibrillator Therapy in Advanced Heart Failure". Heart Failure Clinics. 12 (3): 423–436. doi:10.1016/j.hfc.2016.03.010. ISSN 1551-7136. PMID 27371518.
- ↑ Implantable cardioverter defibrillators and cardiac resynchronisation therapy for arrhythmias and heart failure - National Institute for Health and Care Excellence (NICE) Guidelines. June 2014
- ↑ Mima, Takahiro; Baba, Shiro; Yokoo, Noritaka; Kaichi, Shinji; Doi, Takahiro; Doi, Hiraku; Heike, Toshio (2010). "Effective cardiac resynchronization therapy for an adolescent patient with dilated cardiomyopathy seven years after mitral valve replacement and septal anterior ventricular exclusion". Journal of Cardiothoracic Surgery. 5 (1): 47. doi:10.1186/1749-8090-5-47. ISSN 1749-8090. PMC 2898667. PMID 20525228.
- ↑ Mountney, P.; Behar, J. M.; Toth, D.; Panayiotou, M.; Reiml, S.; Jolly, M. P.; Karim, R.; Zhang, L.; Brost, A. (November 2017). "A Planning and Guidance Platform for Cardiac Resynchronization Therapy". IEEE Transactions on Medical Imaging. 36 (11): 2366–2375. doi:10.1109/TMI.2017.2720158. ISSN 0278-0062. PMID 28678701. S2CID 3871779.
- ↑ Zhou, Weihua; Hou, Xiaofeng; Piccinelli, Marina; Tang, Xiangyang; Tang, Lijun; Cao, Kejiang; Garcia, Ernest V.; Zou, Jiangang; Chen, Ji (December 2014). "3D fusion of LV venous anatomy on fluoroscopy venograms with epicardial surface on SPECT myocardial perfusion images for guiding CRT LV lead placement". JACC: Cardiovascular Imaging. 7 (12): 1239–1248. doi:10.1016/j.jcmg.2014.09.002. ISSN 1876-7591. PMID 25440593.