Coombs test
| Coombs test | |
|---|---|
| MeSH | D003298 |
| MedlinePlus | 003344 |
A Coombs test, also known as antiglobulin test (AGT) is either of two blood tests used in immunohematology. They are the direct and indirect Coombs tests. The direct Coombs test detects antibodies that are stuck to the surface of the red blood cells.[1] Since these antibodies sometimes destroy red blood cells, a person can be anemic and this test can help clarify the condition. The indirect Coombs detects antibodies that are floating freely in the blood.[1] These antibodies could act against certain red blood cells and the test can be done to diagnose reactions to a blood transfusion.[1]
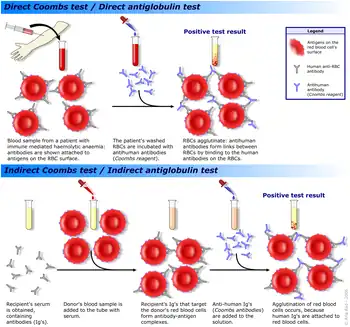
The direct Coombs test is used to test for autoimmune hemolytic anemia—that is, a condition where the immune system breaks down red blood cells, leading to anemia. The direct Coombs test is used to detect antibodies or complement proteins attached to the surface of red blood cells. To perform the test, a blood sample is taken and the red blood cells are washed (removing the patient's own plasma and unbound antibodies from the red blood cells) and then incubated with anti-human globulin ("Coombs reagent"). If the red cells then agglutinate, the direct Coombs test is positive, a visual indication that antibodies or complement proteins are bound to the surface of red blood cells and may be causing destruction of those cells.
The indirect Coombs test is used in prenatal testing of pregnant women and in testing prior to a blood transfusion. The test detects antibodies against foreign red blood cells. In this case, serum is extracted from a blood sample taken from the patient. The serum is incubated with foreign red blood cells of known antigenicity. Finally, anti-human globulin is added. If agglutination occurs, the indirect Coombs test is positive.[2]
Mechanism
The two Coombs tests are based on anti-human antibodies binding to human antibodies, commonly IgG or IgM. These anti-human antibodies are produced by plasma cells of non-human animals after immunizing them with human plasma. Additionally, these anti-human antibodies will also bind to human antibodies that may be fixed onto antigens on the surface of red blood cells (RBCs). In the appropriate test tube conditions, this can lead to agglutination of RBCs and allowing for visualisation of the resulting clumps of RBCs. If clumping is seen, the Coombs test is positive; if not, the Coombs test is negative.[3]
Common clinical uses of the Coombs test include the preparation of blood for transfusion in cross-matching, atypical antibodies in the blood plasma of pregnant women as part of antenatal care, and detection of antibodies for the diagnosis of immune-mediated haemolytic anemias.[4]
Coombs tests are performed using RBCs or serum (direct or indirect, respectively) from venous whole blood samples which are taken from patients by venipuncture. The venous blood is taken to a laboratory (or blood bank), where trained scientific technical staff do the Coombs tests. The clinical significance of the result is assessed by the physician who requested the Coombs test, perhaps with assistance from a laboratory-based hematologist.
Direct Coombs test
The direct Coombs test, also referred to as the direct antiglobulin test (DAT), is used to detect if antibodies or complement system factors have bound to RBCs surface antigens.[5] The DAT is not currently required for pre-transfusion testing[6] but may be included by some laboratories. Pre-transfusion, patients often have an indirect Coombs test.
Uses
.png.webp)
The direct Coombs test is used clinically when immune-mediated hemolytic anemia (antibody-mediated destruction of RBCs) is suspected. A positive Coombs test indicates that an immune mechanism is attacking the patient's RBCs. This mechanism could be autoimmunity, alloimmunity or a drug-induced immune-mediated mechanism.[3]
Examples of alloimmune hemolysis
- Hemolytic disease of the newborn (also known as HDN or erythroblastosis fetalis)
- Rh D hemolytic disease of the newborn (also known as Rh disease)
- ABO hemolytic disease of the newborn (the direct Coombs test may only be weakly positive)
- Anti-Kell hemolytic disease of the newborn
- Rh c hemolytic disease of the newborn
- Rh E hemolytic disease of the newborn
- Other blood group incompatibility (RhC, Rhe, Kidd, Duffy, Lewis, MN, P and others)
- Alloimmune hemolytic transfusion reactions
Examples of autoimmune hemolysis/immunohemolytic hemolysis
- Warm antibody autoimmune hemolytic anemia
- Idiopathic
- Systemic lupus erythematosus
- Evans' syndrome (antiplatelet antibodies and hemolytic antibodies)
- Cold antibody immunohemolytic anemia
Drug-induced immune-mediated hemolysis
- Methyldopa (IgG mediated type II hypersensitivity)
- Penicillin (high dose)
- Quinidine (IgM mediated activation of classical complement pathway and Membrane attack complex, MAC)
(A memory device to remember that the DAT tests the RBCs and is used to test infants for haemolytic disease of the newborn is: Rh Disease; R = RBCs, D = DAT.)
Laboratory
The patient's RBCs are washed (removing the patient's own serum) and then centrifuged with antihuman globulin (also known as Coombs reagent). If immunoglobulin or complement factors have been fixed on to the RBC surface in-vitro, the antihuman globulin will agglutinate the RBCs and the direct Coombs test will be positive. (A visual representation of a positive direct Coombs test is shown in the upper half of the schematic).
Indirect Coombs test
The indirect Coombs test, also referred to as the indirect antiglobulin test (IAT), is used to detect in-vitro antibody-antigen reactions. It is used to detect very low concentrations of antibodies present in a patient's plasma/serum prior to a blood transfusion. In antenatal care, the IAT is used to screen pregnant women for antibodies that may cause hemolytic disease of the newborn. The IAT can also be used for compatibility testing, antibody identification, RBC phenotyping, and titration studies.
Uses
Blood transfusion preparation
The indirect Coombs test is used to screen for antibodies in the preparation of blood for blood transfusion. The donor's and recipient's blood must be ABO and Rh D compatible. Donor blood for transfusion is also screened for infections in separate processes.
- Antibody screening
A blood sample from the recipient and a blood sample from every unit of donor blood are screened for antibodies with the indirect Coombs test. Each sample is incubated against a wide range of RBCs that together exhibit a full range of surface antigens (i.e. blood types).
- Cross matching
The indirect Coombs test is used to test a sample of the recipient's serum for antibodies against a sample of the blood donor's RBCs. This is sometimes called cross-matching blood.
Antenatal antibody screening
The indirect Coombs test is used to screen pregnant women for IgG antibodies that are likely to pass through the placenta into the fetal blood and cause haemolytic disease of the newborn.
Laboratory method
The IAT is a two-stage test. (A cross match is shown visually in the lower half of the schematic as an example of an indirect Coombs test).
First stage
Nonpatient, washed red blood cells (RBCs) with known antigens are incubated with patient serum containing unknown antibody content. If the serum contains antibodies to antigens on the RBC surface, the antibodies will bind to the surface of the RBCs.
Second stage
The RBCs are washed three or four times with isotonic saline solution and then incubated with antihuman globulin. If antibodies have bound to RBC surface antigens in the first stage, RBCs will agglutinate when incubated with the antihuman globulin (also known Coombs reagent) in this stage, and the indirect Coombs test will be positive.
Titrations
By diluting a serum containing antibodies the quantity of the antibody in the serum can be gauged. This is done by using doubling dilutions of the serum and finding the maximum dilution of test serum that is able to produce agglutination of relevant RBCs.
Coombs reagent
Coombs reagent (also known as Coombs antiglobulin or antihuman globulin) is used in both the direct Coombs test and the indirect Coombs test. Coombs reagent is antihuman globulin. It is made by injecting human globulin into animals, which produce polyclonal antibodies specific for human immunoglobulins and human complement system factors. More specific Coombs reagents or monoclonal antibodies can be used.
Enhancement media
Both IgM and IgG antibodies bind strongly with their complementary antigens. IgG antibodies are most reactive at 37 °C. IgM antibodies are easily detected in saline at room temperature as IgM antibodies are able to bridge between RBC's owing to their large size, efficiently creating what is seen as agglutination. IgG antibodies are smaller and require assistance to bridge well enough to form a visual agglutination reaction. Reagents used to enhance IgG detection are referred to as potentiators. RBCs have a net negative charge called zeta potential which causes them to have a natural repulsion for one another. Potentiators reduce the zeta potential of RBC membranes. Common potentiators include low ionic strength solution (LISS), albumin, polyethylene glycol (PEG), and proteolytic enzymes.
History
The Coombs test was first described in 1945 by Cambridge immunologists Robin Coombs (after whom it is named), Arthur Mourant and Rob Race.[8] Historically, it was done in test tubes. Today, it is commonly done using microarray and gel technology.
Popular culture
In Arthur Hailey's 1959 book The Final Diagnosis, the wife of a hospital staff member is pregnant; she is Rh negative and he is Rh positive. He mentions this, and recommends an indirect Coombs test to the new assistant pathologist, who presumes this to be obvious, and even signs the requisition form to order Coombs serum. Due to extreme penny-pinching by the chief pathologist, he overrides the other doctor's decision to order Coombs serum, and refuses to perform an indirect Coombs test, instead deciding that protein and saline tests alone are sufficient. This decision ends up causing tragic consequences. The 1961 film adaption of the novel The Young Doctors tells this story but with a happy ending.
References
- 1 2 3 "Coombs test: MedlinePlus Medical Encyclopedia". medlineplus.gov. Retrieved 2019-05-06.
- ↑ F. Rosen and R. Geha, Case Studies in Immunology, 4th ed., Garland Science, p.173.
- 1 2 Zantek, Nicole D.; Koepsell, Scott A. (2012-04-12). "The direct antiglobulin test: A critical step in the evaluation of hemolysis". American Journal of Hematology. 87 (7): 707–709. doi:10.1002/ajh.23218. Retrieved 2021-07-26.
- ↑ Theiss, Samuel R. Coombs Test. StatPearls Publishing LLC.
- ↑ Reid ME, Lomas-Francis C (23 December 2015). "Chapter 136: Erythrocytes Antigens and Antibodies". Williams hematology (9th ed.). New York: McGraw-Hill. ISBN 9780071833004. OCLC 913870019.
- ↑ "13.3: Pre-transfusion testing". www.transfusionguidelines.org. Joint United Kingdom (UK) Blood Transfusion and Tissue Transplantation Services Professional Advisory Committee. Retrieved 2021-07-26.
- ↑ Joe Chaffin (2017-02-27). "028: Who DAT? with Sue Johnson". Citing: C Feldman & J O'Connor. |author=Mikael Häggström
- ↑ Coombs, R. R.; Mourant, A. E.; Race, R. R. (1945). "A new test for the detection of weak and incomplete Rh agglutinins". British Journal of Experimental Pathology. 26: 255–66. PMC 2065689. PMID 21006651.
External links
- Coombs’ test - direct - Medlineplus.org.
- Coombs’ test - indirect - Medlineplus.org.
- Acute Anemia - emedicine.com
- Drugs that cause haemolytic anemia - Merck Manual.
- Coombs'+Test at the US National Library of Medicine Medical Subject Headings (MeSH)
| Authority control: National libraries |
|---|