Migraine-associated vertigo
| Migraine-associated vertigo | |
|---|---|
| Other names: Migraine-associated vertigo (MAV), Migrainous vertigo, Migraine-related vestibulopathy. | |
| Specialty | Neurology |
Migraine-associated vertigo or Vestibular migraine (VM) is vertigo with migraine, either as a symptom of migraine or as a related neurological disorder. A 2010 report from the University of British Columbia published in the journal Headache said that "'Migraine associated vertigo' is emerging as a popular diagnosis for patients with recurrent vertigo" but, "in contrast to basilar artery migraine, is neither clinically nor biologically plausible as a migraine variant."[1] Epidemiological studies indicate a strong link between vertigo and migraine.[2]
Signs and symptoms
Vertigo is a medically recognized term for the symptom of a vestibular system disturbance. It may include a feeling of rotation or illusory sensations of motion or both. The general term dizziness is used by nonmedical people for those symptoms but often refers to a feeling of light-headedness, giddiness, drowsiness, or faintness, all of which must be differentiated from true vertigo,[3] since the latter symptoms might have other causes.
Motion sickness occurs more frequently in migraine patients (30–50% more than in controls).[4] Benign paroxysmal vertigo of childhood is an example of migraine-associated vertigo in which headache does not often occur.[5] Basilar artery migraine (BAM) consists of two or more symptoms (vertigo, tinnitus, decreased hearing, ataxia, dysarthria, visual symptoms in both hemifields or both eyes, diplopia, bilateral paresthesias, paresis, decreased consciousness and/or loss of consciousness) followed by throbbing headache. Auditory symptoms are rare. However, a study showed a fluctuating low-tone sensorineural hearing loss in more than 50% of patients with BAM with a noticeable change in hearing just before the onset of a migraine headache. The attacks of vertigo are usually concurrent with a headache and the family history is usually positive. The diagnostician must rule out: TIAs, and paroxysmal vestibular disorder[6] accompanied by headache.
There is also a familial vestibulopathy, familial benign recurrent vertigo (fBRV), where episodes of vertigo occur with or without a migraine headache. Testing may show profound vestibular loss. The syndrome responds to acetazolamide. Familial hemiplegic migraine (FHM) has been linked to mutations in the calcium channel gene. (Ophoff et al. 1966 cf. Lempert et al.)[5]
Pathophysiology
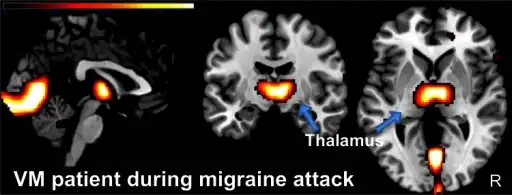
The pathophysiology of MAV is not completely understood; both central and peripheral defects have been observed.[7]
Diagnosis
By the Consensus document of the Barány Society and the International Headache Society on the diagnostic criteria of vestibular migraine, the diagnostic criteria of vestibular migraine are:[8]
- At least 5 episodes with vestibular symptoms of moderate or severe intensity, lasting 5 minutes to 72 hours
- Current or previous history of migraine with or without aura according to the International Classification of Headache Disorders (ICHD)
- One or more migraine features with at least 50% of the vestibular episodes:
- headache with at least two of the following characteristics: one sided location, pulsaing quality, moderate or severe pain intensity, aggravation by routine physical activity
- photophobia and phonophobia
- visual aura
- Not better accounted for by another vestibular or ICHD diagnosis
The diagnostic criteria of probable vestibular migraine are:
- At least 5 episodes with vestibular symptoms of moderate or severe intensity, lasting 5 minutes to 72 hours
- Only one of the criteria B and C for vestibular migraine is fulfilled (migraine history or migraine features during the episode)
- Not better accounted for by another vestibular or ICHD diagnosis
Classification
- Benign paroxysmal positional vertigo
- Migraine is commonly associated with BPPV, the most common vestibular disorder in patients presenting with dizziness. The two may be linked by genetic factors or by vascular damage to the labyrinth.[5]
- Ménière's disease
- There is an increased prevalence of migraine in patients with Ménière's disease and migraine leads to a greater susceptibility of developing Ménière’s disease. But they can be distinguished. Ménière's disease may go on for days or even years, while migraines typically do not last longer than 24 hours.[5]
- Motion sickness
- More prevalent in patients with migraine.[5]
- Psychiatric syndromes
- Dizziness and spinning vertigo are the second most common symptom of panic attacks, and they can also present as a symptom of major depression. Migraine is a risk factor for developing major depression and panic disorder and vice versa.[5]
Treatment
Treatment of migraine-associated vertigo is the same as the treatment for migraine in general.[9] There is not enough evidence to indicate which medications are most effective for preventing vestibular migraine.[10]
Epidemiology
The prevalence of migraine and vertigo is 1.6 times higher in 200 dizziness clinic patients than in 200 age- and sex-matched controls from an orthopaedic clinic. Among the patients with unclassified or idiopathic vertigo, the prevalence of migraine was shown to be elevated. In another study, migraine patients reported 2.5 times more vertigo and also 2.5 more dizzy spells during headache-free periods than the controls.[5]
MAV may occur at any age with a female:male ratio of between 1.5 and 5:1. Familial occurrence is not uncommon. In most patients, migraine headaches begin earlier in life than MAV with years of headache-free periods before MAV manifests.[5]
In a diary study, the 1-month prevalence of MAV was 16%, frequency of MAV was higher and duration longer on days with headache, and MAV was a risk factor for co-morbid anxiety.[11]
References
- ↑ Phillips J, Longridge N, Mallinson A, Robinson G (August 2010). "Migraine and Vertigo: A Marriage of Convenience?". Headache. 50 (8): 1362–1365. doi:10.1111/j.1526-4610.2010.01745.x. PMID 20738416. S2CID 12044693.
- ↑ von Brevern, M; Baloh RW; Bisdorff A; Brandt T; Bronstein AM; Furman JM; Goadsby PJ; Neuhauser H; Radtke A; Versino M (2011). "Response to: Migraine and Vertigo: A Marriage of Convenience?". Headache. 51 (2): 308–309. doi:10.1111/j.1526-4610.2010.01834.x. PMID 21284614. S2CID 33074758.
- ↑ Lempert T, Neuhauser H (August 2005). "Migrainous vertigo". Neurol Clin. 23 (3): 715–730, vi. doi:10.1016/j.ncl.2005.01.003. PMID 16026673.
- ↑ Neuhauser H, Lempert T (February 2004). "Vertigo and dizziness related to migraine: a diagnostic challenge". Cephalalgia. 24 (2): 83–91. doi:10.1111/j.1468-2982.2004.00662.x. PMID 14728703. S2CID 240201.
- 1 2 3 4 5 6 7 8 Lempert T, Neuhauser H (March 2009). "Epidemiology of vertigo, migraine and vestibular migraine". J. Neurol. 256 (3): 333–8. doi:10.1007/s00415-009-0149-2. PMID 19225823. S2CID 27402289. Archived from the original on 2021-08-28. Retrieved 2022-06-10.
- ↑ "Vestibular Paroxysmia Treatment, Symptoms, Diagnosis, Treatment, Causes". Vertigo Clinic & Treatment in Rajasthan India. Archived from the original on 2021-09-16. Retrieved 2020-12-14.
- ↑ Cal R, Bahmad Jr F (2008). "Migraine associated with auditory-vestibular dysfunction" (PDF). Braz J Otorhinolaryngol. 74 (4): 606–12. doi:10.1016/S1808-8694(15)30611-X. PMID 18852990. Archived (PDF) from the original on 2012-10-11. Retrieved 2022-06-10.
- ↑ Lempert T, et al. (2012). "Vestibular migraine: Diagnostic criteria. Consensus document of the Barány Society and the International Headache Society". Journal of Vestibular Research. 22 (4): 167–172. doi:10.3233/VES-2012-0453. PMID 23142830.
- ↑ Fotuhi M, Glaun B, Quan SY, Sofare T (May 2009). "Vestibular migraine: a critical review of treatment trials". J. Neurol. 256 (5): 711–6. doi:10.1007/s00415-009-5050-5. PMID 19252785. S2CID 23572094.
- ↑ Maldonado Fernández, Miguel; Birdi, Jasminder S.; Irving, Greg J.; Murdin, Louisa; Kivekäs, Ilkka; Strupp, Michael (2015-06-21). "Pharmacological agents for the prevention of vestibular migraine". The Cochrane Database of Systematic Reviews (6): CD010600. doi:10.1002/14651858.CD010600.pub2. ISSN 1469-493X. PMC 6494480. PMID 26093662.
- ↑ Salhofer, S; Lieba-Samal D; Freydl E; Bartl S; Wiest G; Wöber C (2010). "Migraine and vertigo--a prospective diary study". Cephalalgia. 30 (7): 821–828. doi:10.1177/0333102409360676. PMID 20647173. S2CID 31453147.
External links
| External resources |
|---|
- eMedicine article Archived 2022-08-30 at the Wayback Machine