Phlegmasia cerulea dolens
| Phlegmasia cerulea dolens | |
|---|---|
 | |
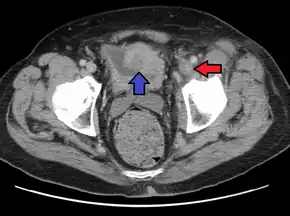
| A person with a two hour history of phlegmasia cerulea dolens (left leg, right side of image) | |
| Specialty | Vascular surgery |
| Symptoms | Swelling, pain, bluish discoloration[1] |
| Complications | Pulmonary embolism, compartment syndrome, gangrene, limb loss[1] |
| Risk factors | Cancer, hypercoagulability, venous stasis, surgery, major trauma, pregnancy, hormone therapy, immobilization[1] |
| Diagnostic method | Ultrasound[1] |
| Differential diagnosis | Arterial embolism, deep vein thrombosis, cellulitis, lymphedema[1] |
| Treatment | Leg elevation, anticoagulation, thrombolysis, thrombectomy[1] |
| Frequency | Uncommon[1] |
Phlegmasia cerulea dolens (PCD) is a severe form of deep venous thrombosis (DVT) that blocks outflow of blood from a limb.[1] Symptoms include swelling, pain, and bluish discoloration.[1] Most commonly the leg is affected, with less than 10% of cases affected the arm.[2] Complications may include pulmonary embolism, compartment syndrome, gangrene, and limb loss.[1]
Risk factors include cancer (30%), hypercoagulability, venous stasis, surgery, major trauma, pregnancy, hormone therapy, and immobilization; though in some cases none are present.[1] The underlying mechanism involves extensive blockage of an extremity vein by a clot such that blood is unable to leave.[1] Diagnosis is usually by ultrasound.[1] A similar, but less severe, condition that results in a white limb is known as phlegmasia alba dolens.[1]
It is a medical emergency.[1] Management involves raising the leg above the level of the heart, anticoagulants with heparin, and intravenous fluids.[1] The clot may be removed either by thrombolysis or thrombectomy.[1] The risk of death among those severely affected is as high as 40%.[1] Among those who survive post thrombotic syndrome is common.[1]
Phlegmasia cerulea dolens is uncommon.[1] Those most commonly affected are in their 50s or 60.[1] Males are more commonly affected than females.[1] The condition was first described and named in 1938 by Gregoire.[1] The term means "painful blue inflammation".[1]
Signs and symptoms
It is characterized by progressive lower extremity swelling distal to the thigh, tight shiny skin, bluish skin (inadequate blood oxygenation), petechiae or purpura, and sudden severe pain of the affected limb in proportion to the level of venous blockage. People often have difficulty walking. Bilsters, bullae, numbness, an motor weakness may develop in severe cases, along with gangrene in ~50% of cases.[1][3] Distal pulses may be felt early on but may diminish over time, and doppler signal can be usually heard throughout disease progression.[3] The left limb is more commonly affected due to its vascular anatomy (the right internal iliac artery directly overlies the left iliac vein).[4][1]
Associated diseases
PCD is associated with an underlying cancer in 20-40% of cases.[1] There is a high risk of massive pulmonary embolism, even under anticoagulation.[5]
Cause
Risk factors are present in around 50% of cases. These include cancer, hyper-coagulable states, cardiac disease, venous stasis, venous insufficiency, May-Thurner syndrome (right iliac artery compressing the left iliac vein that runs beneath it), surgery, trauma, pregnancy, inferior vena cava (IVC) filter, hormone therapy, hormonal birth control, prolonged immobilization, inflammatory bowel disease, heart failure, and central venous cathetes. The cause is unknown in ~10% of cases.[2][4][1]
Pathophysiology
When a thrombus occludes an extremity vein, pressure backs up in the venous system leading plasma fluid to leak out into the interstitium of the affected limb. This increases the pressure of that limb compartment, which can collapse the arteries and lead to acute ischemia, gangrene, hypovolemia, and hemodynamic instability.[1][6]
Diagnosis
PCD is best diagnosed with contrast venography, but venous duplex ultrasonography is used more commonly. Magnetic resonance and computed tomography venography can also be used.[4]
Differential diagnosis
Other conditions that can present similarly include:[1]
- Cellulitis
- Venous insufficiency
- Superficial thrombophlebitis
- DVT
- Arterial embolism
- Lymphedema
Treatment
Treatment includes immediate anticoagulation, fluid resuscitation, bed rest, limb elevation above 60º, limb wrap to reduce pain and swelling, and either catheter-based thrombolysis, percutaneous transluminal angioplasty, or surgical venous thrombectomy or fasciotomy to remove the blood clot.[4][3][1][6] Some people also suggest an IVC filter before thrombolysis.[4]
Prognosis
PCD is fully reversible if the causal venous thrombus is promptly removed.[3] In the 40-60% of people who go on to develop venous gangrene, there is a 20-50% risk of amputation and 20-40% mortality rate.[1][4] Following PCD resolution people are more likely to develop venous insufficiency and post-thrombotic syndrome.[1]
There is a grading system that has been established:[4][6]
- Grade I = non-complicated (no blistering, strong sensory-motor function and strong distal pulses)
- Grade II = impending venous gangrene (blistering, weak sensory-motor function and weak distal pulses)
- Grade III = venous gangrene
Epidemiology
PCD is most likely to occur in people in their 50s and 60s, but can occur as early as 6 months old. There is slight male predominance of around 1.5:1.[4][1]
History
This phenomenon was first discovered by Fabricus Hildanius in the 16th century, and was officially termed "phlegmasia cerulea dolens" by Gregoire in 1938.[1][4] Phlegmasia originates from the Greek root phlegma (inflammation), cerulea originates from Latin root caeruleus (dark blue), and dolens originates from Latin word dolens (suffering).[3]
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 Gardella, L; Faulk, JB (January 2021). "Phlegmasia Alba And Cerulea Dolens". PMID 33085284. Archived from the original on 2021-08-28. Retrieved 2021-05-09.
{{cite journal}}: Cite journal requires|journal=(help) - 1 2 Greenberg, Jacques; Troutman, Douglas A.; Shubinets, Valeriy; Dougherty, Matthew J.; Calligaro, Keith D. (February 2016). "Phlegmasia Cerulea Dolens in the Upper Extremity: A Case Report and Systematic Review and Outcomes Analysis". Vascular and Endovascular Surgery. 50 (2): 98–101. doi:10.1177/1538574416631645. ISSN 1538-5744. Archived from the original on 2021-08-28. Retrieved 2021-02-16.
- 1 2 3 4 5 Rutherford's vascular surgery and endovascular therapy. Anton N. Sidawy, Bruce A. Perler (9th ed.). Philadelphia, PA. 2019. ISBN 978-0-323-58130-1. OCLC 1037557259. Archived from the original on 2021-08-28. Retrieved 2021-02-11.
{{cite book}}: CS1 maint: others (link) - 1 2 3 4 5 6 7 8 9 Chinsakchai, Khamin; ten Duis, Kaj; Moll, Frans L.; de Borst, Gert J. (January 2011). "Trends in Management of Phlegmasia Cerulea Dolens". Vascular and Endovascular Surgery. 45 (1): 5–14. doi:10.1177/1538574410388309. ISSN 1538-5744. Archived from the original on 2021-08-29. Retrieved 2021-02-16.
- ↑ John T. Owings (December 2005). "Management of Venous Thromboembolism". ACS Surgery. American College of Surgeons. Archived from the original on January 27, 2012. Retrieved January 16, 2012.
- 1 2 3 Chang, Grace; Yeh, James J. (July 2014). "Fulminant phlegmasia cerulea dolens with concurrent cholangiocarcinoma and a lupus anticoagulant: a case report and review of the literature". Blood Coagulation & Fibrinolysis. 25 (5): 507–511. doi:10.1097/MBC.0000000000000057. ISSN 1473-5733. PMID 24553060. Archived from the original on 2021-08-28. Retrieved 2021-02-16.
External links
| Classification | |
|---|---|
| External resources |