Kidney dysplasia
| Kidney dysplasia | |
|---|---|
| Other names: Multicystic dysplastic kidney,[1] renal dysplasia,[1] multicystic renal dysplasia[2] | |
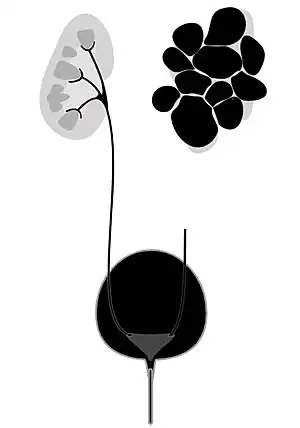 | |
| Diagram of multicystic dysplastic kidney | |
| Specialty | Nephrology, urology |
| Complications | Hydronephrosis, high blood pressure, urinary tract infection, kidney failure[1] |
| Risk factors | Family history, use of certain medications or drugs during pregnancy[1] |
| Diagnostic method | Ultrasound[1] |
| Treatment | Follow-up, dialysis, kidney transplant[1] |
| Frequency | 1 in 4,000 newborns[1] |
Kidney dysplasia, also known as multicystic dysplastic kidney (MCDK), is when the internal structures of one or both kidneys do not form properly during early development.[1] If one kidney is affected, often there are no symptoms, though in some cases the kidney enlarges and causes pain.[1] Complications can include hydronephrosis, high blood pressure, urinary tract infections (UTI), or kidney failure.[1] If both kidneys are severely affected the child may die around the time of birth.[1]
The cause includes a numbers of genetic mutations and exposure to certain drugs or medications during pregnancy.[1] The underlying mechanism involves urine being unable to flow through the tubules within the kidneys resulting in cyst formation.[1] Diagnosis is generally by ultrasound, either before or after birth.[1]
If only a single kidney is affected and no symptoms are present follow-up to look for potential complications may be all that is required.[1] If both kidneys are affected dialysis or a kidney transplant may be required.[1] In some cases the affected kidney may shrink in size.[1] Kidney dysplasia affects about 1 in 4,000 newborns.[1] It was first described in 1836.[3]
Signs and symptoms
When a diagnosis of multicystic kidney is made in utero by ultrasound, the disease is found to be bilateral in many cases. Those with bilateral disease often have other severe deformities or polysystemic malformation syndromes.[4] In bilateral cases, the newborn has the classic characteristic of Potter's syndrome.[5][6]
The bilateral condition is incompatible with survival, as the contralateral system frequently is abnormal as well. Contralateral ureteropelvic junction obstruction is found in 3% to 12% of infants with multicystic kidney and contralateral vesicoureteral reflux is seen even more often, in 18% to 43% of infants. Because the high incidence of reflux, voiding cystourethrography usually has been considered advisable in all newborns with a multicystic kidney.
Cause
The cause of multicystic dysplastic kidney can be attributed to genetics. Renal dysplasia can be a consequence of a genetic syndrome, which in turn may affect the digestive tract, nervous system, or other areas of the urinary tract. If the mother had been taking certain prescription drugs such as those for hypertension, this may be a precipitating factor as well.[7]
Pathophysiology
The mechanism of multicystic dysplastic kidney is a result of an abnormal induction of metanephric mesenchyme. This could be a result of a formation difficulty of the mesonephric duct. Some mutations in genes associated with renal dysplasia (in syndromes) have been determined. The mutations in question occur at EYA1 or SIX1 genes (branchio-oto-renal syndrome). The PAX2 gene is also thought to play a role in MCDK.[8]
The contralateral kidney often undergoes hypertrophy. This is believed to be a compensatory mechanism to the non-functional MCDK. About 90% of patients with an MCDK will have contralateral hypertrophy into adulthood. The impact of contralateral hypertrophy on long-term renal outcomes is unknown.[9]
Diagnosis
MCDK is usually diagnosed by ultrasound examination before birth. Mean age at the time of antenatal diagnosis is about 28 weeks[10] A microscopic analysis of urine in individuals with probable multicystic dysplastic kidney should be done.[8]One meta-analysis demonstrated that unilateral MCDK occurs more frequently in males and the greater percentage of MCKD occur on the left side of the body.[11]
 Right dysplastic kidney with the largest cyst size measuring 33.16mm
Right dysplastic kidney with the largest cyst size measuring 33.16mm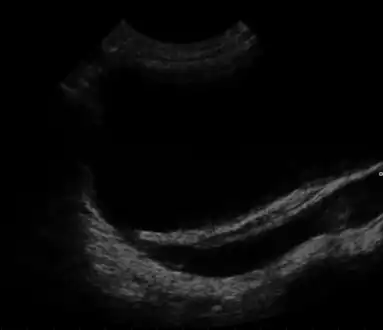 Ultrasound showing vesicoureteral reflux
Ultrasound showing vesicoureteral reflux
Treatment
MCDK is not treatable. However, the patient is observed periodically for the first few years during which ultrasounds are generally taken to ensure the healthy kidney is functioning properly and that the unhealthy kidney is not causing adverse effects. In severe cases MCDK can lead to neonatal fatality (in bilateral cases), however in unilateral cases the prognosis might be better (it would be dependent on associated anomalies).[12][13]
Epidemiology
In regard to the epidemiology of multicystic dysplasia kidney, the incidence of MCDK is estimated to be 1 in every 4,000 live births, making it rare in terms of the general population.[7]
Other animals
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 "Kidney Dysplasia | NIDDK". National Institute of Diabetes and Digestive and Kidney Diseases. Archived from the original on 7 June 2021. Retrieved 24 January 2021.
- ↑ RESERVED, INSERM US14-- ALL RIGHTS. "Orphanet: Multicystic dysplastic kidney". www.orpha.net. Archived from the original on 24 October 2019. Retrieved 31 July 2019.
- ↑ Lager, Donna J.; Abrahams, Neil (2012). Practical Renal Pathology, A Diagnostic Approach E-Book: A Volume in the Pattern Recognition Series. Elsevier Health Sciences. p. 27. ISBN 978-1-4557-3786-4. Archived from the original on 2021-07-11. Retrieved 2021-01-24.
- ↑ Seseke, F. (2003). "Clinical Aspects of Paediatric Urology". Imaging in Paediatric Urology. pp. 1–67. doi:10.1007/978-3-642-55785-9_1. ISBN 978-3-642-62803-0.
- ↑ Potter Syndrome~treatment at eMedicine
- ↑ Lager, Donna J.; Abrahams, Neil (2012-11-07). Practical Renal Pathology, A Diagnostic Approach: A Volume in the Pattern Recognition Series. Elsevier Health Sciences. p. 27. ISBN 978-1455737864. Archived from the original on 2016-05-10. Retrieved 2015-11-25.
- 1 2 "Kidney Dysplasia". www.niddk.nih.gov. Archived from the original on 2015-11-25. Retrieved 2015-11-24.
- 1 2 Multicystic Renal Dysplasia at eMedicine
- ↑ Gaither, Thomas W.; Patel, Ankur; Patel, Chandni; Chuang, Kai-wen; Cohen, Ronald A.; Baskin, Laurence S. (2018). "Natural History of Contralateral Hypertrophy in Patients with Multicystic Dysplastic Kidneys". Journal of Urology. 199 (1): 280–286. doi:10.1016/j.juro.2017.06.075. PMID 28645868. Archived from the original on 2020-07-15. Retrieved 2019-01-08.
- ↑ Chang, Ling-Wei; Chang, Fong-Ming; Chang, Chiung-Hsin; Yu, Chen-Hsiang; Cheng, Yueh-Chin; Chen, Hsi-Yao (2002). "Prenatal diagnosis of fetal multicystic dysplastic kidney with two-dimensional and three-dimensional ultrasound". Ultrasound in Medicine & Biology. 28 (7): 853–858. doi:10.1016/s0301-5629(02)00535-5. PMID 12208325.
- ↑ Schreuder, M. F.; Westland, R.; Van Wijk, J. A. E. (2009). "Unilateral multicystic dysplastic kidney: A meta-analysis of observational studies on the incidence, associated urinary tract malformations and the contralateral kidney". Nephrology Dialysis Transplantation. 24 (6): 1810–1818. doi:10.1093/ndt/gfn777. PMID 19171687.
- ↑ Stevenson, Roger E.; Hall, Judith G.; Everman, David B.; Solomon, Benjamin D. (2015-10-16). Human Malformations and Related Anomalies. Oxford University Press. p. 800. ISBN 9780199386048. Archived from the original on 2016-05-05. Retrieved 2015-11-24.
- ↑ Schwartz, M. William (2012-01-01). The 5 Minute Pediatric Consult. Lippincott Williams & Wilkins. p. 439. ISBN 9781451116564. Archived from the original on 2016-05-12. Retrieved 2015-11-24.
Further reading
- Al-Khaldi, N.; Watson, A. R.; Zuccollo, J.; Twining, P.; Rose, D. H. (1994). "Outcome of antenatally detected cystic dysplastic kidney disease". Archives of Disease in Childhood. 70 (6): 520–522. doi:10.1136/adc.70.6.520. PMC 1029874. PMID 8048824.
- Van Eijk, L.; Cohen-Overbeek, T. E.; Den Hollander, N. S.; Nijman, J. M.; Wladimiroff, J. W. (2002). "Unilateral multicystic dysplastic kidney: A combined pre- and postnatal assessment". Ultrasound in Obstetrics and Gynecology. 19 (2): 180–183. doi:10.1046/j.0960-7692.2001.00497.x. PMID 11876812.
External links
| Classification | |
|---|---|
| External resources |