Bone metastasis
Bone metastasis, or osseous metastatic disease, is a category of cancer metastases that results from primary tumor invasion to bone. Bone-originating primary tumors such as osteosarcoma, chondrosarcoma, and Ewing's sarcoma are rare; the most common bone tumor is a metastasis[1] Bone metastases can be classified as osteolytic, osteoblastic, or both. Unlike hematologic malignancies which originate in the blood and form non-solid tumors, bone metastases generally arise from epithelial tumors and form a solid mass inside the bone. Bone metastases, especially in a state of advanced disease, can cause severe pain, characterized by a dull, constant ache with periodic spikes of incident pain.[2]
| Bone metastasis | |
|---|---|
 | |
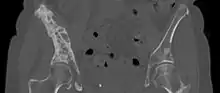
| 3D rendered CT scan of bone metastases of the hip bone, in a 60 year old woman with parotid gland cancer. Large lesions are seen on the ilium on the more distant side. Involvement of the vertebral column has caused a compression fracture. | |
| Specialty | Oncology |
Types of lesions
Under normal conditions, bone undergoes continuous remodeling through osteoclast-mediated bone resorption and osteoblast-mediated bone deposition.[3] These processes are normally tightly regulated within bone to maintain bone structure and calcium homeostasis in the body. Dysregulation of these processes by tumor cells leads to either osteoblastic or osteolytic lesions, reflective of the underlying mechanism of development.[3] Typically, osteolytic metastases are more aggressive than osteoblastic metastases, which have a slower course. Regardless of the phenotype, bone metastases commonly show osteoclast proliferation and hypertrophy.[4]
Primary tumors
- Osteoblastic lesions[5]
- Prostate cancer
- Carcinoid
- Small cell lung cancer
- Hodgkin lymphoma
- Medulloblastoma
- Osteolytic lesions[5]
- Mixed lesions[5]
Signs and symptoms
Bone metastases can cause severe pain, bone fractures, spinal cord compression, hypercalcemia, anemia, spinal instability, decreased mobility, and rapid degradation in the quality of life for patients.[6][7] Patients have described the pain as a dull ache that grows worse over time, with intermittent periods of sharp, jagged pain.[2] Even under controlled pain management, periods of breakthrough pain can occur rapidly, without warning, several times a day.[8] Pain may be worse at night and partially relieved by activity.[9] Metastases to weightbearing bones may become symptomatic early in the course of disease, as compared to metastases to the flat bones of the rib or sternum.[9]
- Effects of bone metastasis
Major complications secondary to bone metastases are termed Skeletal-Related Events (SREs).[10]
- Occurrence of pathological long bone and vertebral fractures
- Development of spinal cord compression
- Need for radiation for pain relief or to treat or prevent pathological fractures or spinal cord compression
- Requirement for surgery to bone
- Episodes of hypercalcemia of malignancy
Other symptoms include:
- Spinal Instability
- Compression of the Cauda Equina
- Cranial Nerve Palsies
- Suppression of bone marrow function (i.e. anemia)
- Decreased mobility

Sources of bone metastases
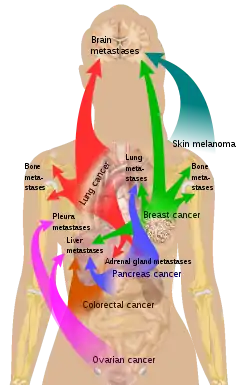
Bone is the third most common location for metastasis, after the lung and liver.[12] While any type of cancer is capable of forming metastatic tumors within bone, the microenvironment of the marrow tends to favor particular types of cancer, including prostate, breast, and lung cancers.[3] In prostate cancer, bone metastases tend to be the only site of metastasis.[2] The most common sites of bone metastases are the spine, pelvis, ribs, skull, and proximal femur.[9]
Common primary tumors
Mechanism
Initial Seeding
Many cancers spread to bone, but not all bones are implicated in cancerous metastasis. The microenvironment of differing bone types is thought to play a role in its predisposition to tumor seeding.[13] For example, trabecular bone rich in red marrow and bone subject to frequent turnover are more likely to be seeded[13] at premetastatic niches formed by interactions between cancerous cells and bone substrate[14] Tumor cells are then attracted to the metastatic niche in the bone. However, the characteristics of these niches have yet to be fully elucidated.[14] Initial seeding can occur prior to the discovery of the primary tumor.[14]
Vascular Seeding
The pathogenesis of bone metastasis via the vasculature is hypothesized to be related to the Batson vertebral vein plexus, a longitudinal valveless system connected to the breast, lung, kidney, thyroid, and prostate gland that extends from the sacrum to the skull.[15] The most common locations of metastases are the pelvis, vertebral bodies, ribs and ends of long bones.[15]
Dormancy
Once established, the tumor cells can remain dormant on the bone microenvironment, radiologically undetectable, for many years.[14] The triggers which eventually awaken metastatic tumor cells are an active field of study as they could elucidate mechanisms of controlling dormancy.[14]
Tumor Cell-Bone Interactions
Tumor cells may have paraneoplastic effects, such as via the secretion of Prostaglandin E, TGF-alpha, TGF-beta, TNF, and interleukins to increase bone resorption. The destruction of bone affected by bone metastases are caused by osteoclast-mediated osteolysis.[15] The uncoupled regulation of osteoclasts and osteoblasts leads to malformation of the bone.[2] Lytic bone lesions may also lead to the pathogenesis of hypercalcemia in cancers that have spread to bone[16]
Diagnosis
Skeletal Radiography
A plain film x-ray of the entire body can identify bone metastasis. However, the sclerotic or osteolytic lesions must be at least 1 cm in diameter.[14] A combination of X-ray, CT and MRI scans may be most sensitive in the diagnosis of cancerous bone metastasis.[14]
Radionuclide Bone Scan
A radionuclide bone scan or scintigraphy can identify bone metastasis. Technetium-99m–labeled bisphosphonate attaches to calcium at sites of active bone formation.[14] Bone scans are more sensitive and can identify lesions earlier than plain radiographs.[14] However, these methods are less effective at identifying purely osteolytic lesions and will also highlight other areas of bone formation, such as those caused by trauma or inflammation unrelated to cancer.[14] Additionally, bladder activity may mask the detection of certain pelvic lesions.[14]
CT Scan
A CT scan can detect bone metastases before they present with symptoms in patients diagnosed with tumors that are high-risk for spread to the bone. Even sclerotic bone metastases are generally less radiodense than enostoses, and it has been suggested that bone metastasis should be the favored diagnosis between the two for bone lesions lower than a cutoff of 1060 Hounsfield units (HU).[10] If a biopsy is indicated, a CT scan is often used to localize the lesion before biopsy.[14]
MRI
MRIs can be used to detect bone metastasis with a sensitivity of 82-100% and a specificity of 73-100%.
PET Scan
Positron emission tomography (PET) with fluorine 18–labeled fluorodeoxyglucose ( 18 F-FDG) is a powerful diagnostic tool to visualize the activity of bone metastasis.[14] Bone metastases on PET scan are usually multiple, irregularly distributed foci of increased tracer uptake without relationship to a single anatomic structure.[14] A PET scan can directly identify tumor cells with significant metabolic rate. However, it is a costly procedure and device availability may be limited.[14]
Bone Markers
Due to the high rate of bone turnover, metabolites are theorized to be capable of detecting bone metastasis.[14] Use of bone markers for detection and screening is an active field of research, though radiographic evidence remains the gold standard.[14] However, once the presence of a bone metastasis has been established, tumor metabolic markers can provide useful diagnostic and prognostic information.[14]
Treatment
The goals of treatment for bone metastases include pain control, prevention and treatment of fractures, maintenance of patient quality of life, and local tumor control.[9] Optimal treatment requires a multidisciplinary team of physicians, including medical and radiation oncologists, orthopedic surgeons, radiologists, nuclear medicine physician, palliative medicine specialists, and more.[14] Assessment of treatment is determined by multiple factors, including performance status, pain score, impact on quality of life, and overall status of clinical disease.[14] Important therapies include external-beam radiotherapy, targeted radioisotope therapy, image guided tumor ablation chemotherapy, and bone-targeting chemotherapeutic agents such as Bisphosphonates and Denosumab. Orthopedic interventions such as internal fixation or spinal decompression may be necessary in the case of loss of structural stability due to bone destruction.[14]
Pain management
The World Health Organization's pain ladder was designed for the management of cancer-associated pain. The original ladder details the management of pain using a sequence of analgesic medications, starting with non-steroidal anti-inflammatory medications and progressing to weak and strong opioids[17]
Other treatments include corticosteroids, radiotherapy, and radionucleotides.[2] Percutaneous osteoplasty involves the use of bone cement to reduce pain and improve mobility.[18] In palliative therapy, the main options are external radiation and radiopharmaceuticals.[19]
Thermal ablation techniques are increasingly being used in the palliative treatment of painful metastatic bone disease. Although the majority of patients experience complete or partial relief of pain following external radiation therapy, the effect is not immediate and has been shown in some studies to be transient in more than half of patients.[20] For patients who are not eligible or do not respond to traditional therapies ( i.e. radiation therapy, chemotherapy, palliative surgery, bisphosphonates or analgesic medications), thermal ablation techniques have been explored as alternatives for pain reduction. Several multi-center clinical trials studying the efficacy of radiofrequency ablation in the treatment of moderate to severe pain in patients with metastatic bone disease have shown significant decreases in patient reported pain after treatment.[21][22] These studies are limited, however, to patients with one or two metastatic sites; pain from multiple tumors can be difficult to localize for directed therapy. More recently, cryoablation has also been explored as a potentially effective alternative as the area of destruction created by this technique can be monitored more effectively by CT than radiofrequency ablation, a potential advantage when treating tumors adjacent to critical structures.[23]
A Cochrane review of calcitonin for the treatment of metastatic bone pain suggests calcitonin yields no significant benefit in the reduction of bone pain or improvements in quality of life.[24]
Bone-Targeted Agents
Bone-Targeted Agents (BTAs) including Bisphosphonates and Denosumab, can interrupt osteoclast-mediated osteolysis.[14] Osteoclast inhibitors, most frequently used in the treatment of osteoporosis, can allow for bone healing and delay complications.[14] BTAs have been shown to decrease the incidence of Skeletal Related Events (SREs) like pathological fractures, thereby decreasing the need for surgical intervention or pain medication.[14]
Prognosis
Many cancers are predisposed to metastasize to bone.[12] The list below details the likelihood of a cancer, if in a stage of advanced metastasis, to have spread to bone at time of death:[25]
- Breast: 65-75%
- Prostate: 65-75%
- Thyroid: 60%
- Kidney: 20-25%
- Lung: 30-40%
Given the high incidence of breast, lung and prostate cancer, these patients account for > 80% of patients with bone metastases.[14]
For patients with advanced metastatic disease involving the bone, median survival from the time of diagnosis of a bone metastasis varies by primary tumor type. A list is included below:[25]
- Breast: 19–25 months
- Prostate: 12–53 months
- Thyroid: 48 months
- Kidney: 12 months
- Lung: 6–7 months
See also
References
- MedlinePlus Overview bonecancer
- Jimenez-Andrade JM, Mantyh WG, Bloom AP, Ferng AS, Geffre CP, Mantyh PW (June 2010). "Bone cancer pain". Annals of the New York Academy of Sciences. 1198 (1): 173–81. Bibcode:2010NYASA1198..173J. doi:10.1111/j.1749-6632.2009.05429.x. PMC 5642911. PMID 20536932.
- Guise T (October 2010). "Examining the metastatic niche: targeting the microenvironment". Semin. Oncol. 37 (Suppl 2): S2–14. doi:10.1053/j.seminoncol.2010.10.007. PMID 21111245.
- Halvorson KG, Sevcik MA, Ghilardi JR, Rosol TJ, Mantyh PW (September 2006). "Similarities and differences in tumor growth, skeletal remodeling and pain in an osteolytic and osteoblastic model of bone cancer". Clin J Pain. 22 (7): 587–600. doi:10.1097/01.ajp.0000210902.67849.e6. PMID 16926574. S2CID 40275522.
- Macedo, F; Ladeira, K; Pinho, F; Saraiva, N; Bonito, N; Pinto, L; Goncalves, F (3 March 2017). "Bone Metastases: An Overview". Oncology Reviews. 11 (1): 321. doi:10.4081/oncol.2017.321. PMC 5444408. PMID 28584570.
- Coleman RE (October 2006). "Clinical features of metastatic bone disease and risk of skeletal morbidity". Clin. Cancer Res. 12 (20 Pt 2): 6243s–9s. doi:10.1158/1078-0432.CCR-06-0931. PMID 17062708.
- Mercadante S (January 1997). "Malignant bone pain: pathophysiology and treatment". Pain. 69 (1–2): 1–18. doi:10.1016/S0304-3959(96)03267-8. PMID 9060007. S2CID 44576422.
- Zeppetella G (March 2009). "Impact and management of breakthrough pain in cancer". Current Opinion in Supportive and Palliative Care. 3 (1): 1–6. doi:10.1097/SPC.0b013e3283260658. PMID 19365156. S2CID 20516011.
- Jacofsky, David (2004). "Metastatic Disease to Bone". Hospital Physician.
- Ulano, Adam; Bredella, Miriam A.; Burke, Patrick; Chebib, Ivan; Simeone, F. Joseph; Huang, Ambrose J.; Torriani, Martin; Chang, Connie Y. (2016). "Distinguishing Untreated Osteoblastic Metastases From Enostoses Using CT Attenuation Measurements". American Journal of Roentgenology. 207 (2): 362–368. doi:10.2214/AJR.15.15559. ISSN 0361-803X. PMID 27101076.
- List of included entries and references is found on main image page in Commons: Commons:File:Metastasis sites for common cancers.svg#Summary
- Vigorita, Vincent (2007). Orthopaedic Pathology. Lippincott Williams & Wilkins. p. 527. ISBN 978-0781796705.
- Fornetti, J., Welm, A.L. and Stewart, S.A. (2018), Understanding the Bone in Cancer Metastasis. J Bone Miner Res, 33: 2099-2113. https://doi-org.ucsf.idm.oclc.org/10.1002/jbmr.3618
- Abeloff's Clinical Oncology. 2020. doi:10.1016/c2015-0-05400-4. ISBN 9780323476744. S2CID 70437912.
- Miller, Mark D.; Thompson, Stephen R. (2019-10-05). Miller's Review of Orthopaedics E-Book. Elsevier Health Sciences. ISBN 978-0-323-60980-7.
- Hiraga, Toru (June 2019). "Bone metastasis: Interaction between cancer cells and bone microenvironment". Journal of Oral Biosciences. 61 (2): 95–98. doi:10.1016/j.job.2019.02.002. S2CID 92580605.
- Anekar, Aabha A.; Cascella, Marco (2022), "WHO Analgesic Ladder", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 32119322, retrieved 2022-09-14
- Anselmetti, Giovanni Carlo (June 2010). "Osteoplasty: Percutaneous Bone Cement Injection beyond the Spine". Seminars in Interventional Radiology. 27 (2): 199–208. doi:10.1055/s-0030-1253518. PMC 3036518. PMID 21629409.
- Criteria for Palliation of Bone Metastases – Clinical Applications from International Atomic Energy Agency. Retrieved November 2011
- Tong, Daphne; Gillick, Laurence; Hendrickson, Frank R. (1982-09-01). "The palliation of symptomatic osseous metastases final results of the study by the radiation therapy oncology group". Cancer. 50 (5): 893–899. doi:10.1002/1097-0142(19820901)50:5<893::aid-cncr2820500515>3.0.co;2-y. PMID 6178497.
- Dupuy, Damian E.; Liu, Dawei; Hartfeil, Donna; Hanna, Lucy; Blume, Jeffrey D.; Ahrar, Kamran; Lopez, Robert; Safran, Howard; DiPetrillo, Thomas (2010-02-15). "Percutaneous radiofrequency ablation of painful osseous metastases". Cancer. 116 (4): 989–997. doi:10.1002/cncr.24837. ISSN 1097-0142. PMC 2819592. PMID 20041484.
- Goetz, Matthew P.; Callstrom, Matthew R.; Charboneau, J. William; Farrell, Michael A.; Maus, Timothy P.; Welch, Timothy J.; Wong, Gilbert Y.; Sloan, Jeff A.; Novotny, Paul J. (2004-01-15). "Percutaneous Image-Guided Radiofrequency Ablation of Painful Metastases Involving Bone: A Multicenter Study". Journal of Clinical Oncology. 22 (2): 300–306. doi:10.1200/JCO.2004.03.097. ISSN 0732-183X. PMID 14722039.
- Callstrom, Matthew R.; Dupuy, Damian E.; Solomon, Stephen B.; Beres, Robert A.; Littrup, Peter J.; Davis, Kirkland W.; Paz-Fumagalli, Ricardo; Hoffman, Cheryl; Atwell, Thomas D. (2013-03-01). "Percutaneous image-guided cryoablation of painful metastases involving bone". Cancer. 119 (5): 1033–1041. doi:10.1002/cncr.27793. ISSN 1097-0142. PMC 5757505. PMID 23065947.
- Martinez-Zapata, MJ (2012). "Calcitonin used to treat metastatic bone pain". Cochrane Database Syst Rev (3): CD003223. doi:10.1002/14651858.CD003223.pub2. PMID 16856000.
- Selvaggi, Giovanni; Scagliotti, Giorgio V. (2005-12-01). "Management of bone metastases in cancer: A review". Critical Reviews in Oncology/Hematology. 56 (3): 365–378. doi:10.1016/j.critrevonc.2005.03.011. ISSN 1040-8428.
{kind=link}
Further reading
- Bellahcène A, Castronovo V (January 1997). "Expression of bone matrix proteins in human breast cancer: potential roles in microcalcification formation and in the genesis of bone metastases". Bull Cancer. 84 (1): 17–24. PMID 9180854.
- Furger KA, Menon RK, Tuck AB, Bramwell VH, Chambers AF (November 2001). "The functional and clinical roles of osteopontin in cancer and metastasis". Curr. Mol. Med. 1 (5): 621–32. doi:10.2174/1566524013363339. PMID 11899236.
- Ibrahim T, Leong I, Sanchez-Sweatman O, et al. (2000). "Expression of bone sialoprotein and osteopontin in breast cancer bone metastases". Clin. Exp. Metastasis. 18 (3): 253–60. doi:10.1023/A:1006754605901. PMID 11315099. S2CID 27673069.
- Chung, Leland W.K.; Isaacs, William B.; Simons, Jonathan W. (2007). Prostate Cancer: Biology, Genetics, and the New Therapeutics. Humana Press. ISBN 978-1-59745-224-3.