Classic autism
Kanner autism, or classic autism, is an outdated neurodevelopmental diagnosis which is now considered part of autism spectrum disorder.[3][10] The term 'autism' was historically used to refer specifically to classic autism,[10] but it is now more commonly used for the spectrum at large.[11][12]
| Autism | |
|---|---|
 | |
| An autistic boy stacking cans | |
| Specialty | Psychiatry, pediatrics, occupational medicine |
| Symptoms | Trouble with social interaction, verbal and nonverbal communication, and presence of restricted interests and repetitive behavior[1] |
| Complications | Social isolation, employment problems, stress |
| Usual onset | By age two or three[2][3] |
| Duration | Lifelong[2] |
| Causes | Genetic and environmental factors[4] |
| Diagnostic method | Based on behavior and developmental history[2] |
| Differential diagnosis | Reactive attachment disorder, intellectual disability, schizophrenia[5] |
| Treatment | Occupational therapy, speech therapy, psychotropic medication[6][7] |
| Medication | Antipsychotics, antidepressants, stimulants (associated symptoms)[8] |
| Frequency | 24.8 million (2015)[9] |
Parents often noticed signs of autism during the first three years of their child's life.[1][3]
Autism was hypothesized to be caused by a combination of genetic and environmental factors,[4] with genetic factors thought to heavily predominate.[13] Controversies surround other proposed environmental causes; for example, the vaccine hypothesis, which although disproven, continues to hold sway in certain communities.[14][15] Contemporary diagnostic manuals include only one diagnosis - autism spectrum disorder (ASD) - which includes classic autism along with Asperger syndrome and pervasive developmental disorder not otherwise specified (PDD-NOS).[3]
Globally, classic autism was estimated to affect 24.8 million people as of 2015.[9]
Characteristics
Classic autism is a highly variable neurodevelopmental disorder[16] whose symptoms first appear during infancy or childhood, and generally follows a steady course without remission.[17] Autistic people may be severely impaired in some respects but average, or even superior, in others.[18] Overt symptoms gradually begin after the age of six months and become established by age two or three years.[19] Some autistic children experience regression in their communication and social skills after reaching developmental milestones at a normal pace.[20] It was said to be distinguished by a characteristic triad of symptoms: impairments in social interaction, impairments in communication, and repetitive behavior. Other aspects, such as atypical eating, are also common but are not essential for diagnosis.[21] Individual symptoms of autism occur in the general population and appear not to associate highly, without a sharp line separating pathologically severe from common traits.[22]
Social development
Autistic people have social impairments and often lack the intuition about others that many people take for granted. Unusual social development becomes apparent early in childhood. Autistic infants show less attention to social stimuli, smile and look at others less often, and respond less to their own name. Autistic toddlers differ more strikingly from social norms; for example, they have less eye contact and turn-taking, and do not have the ability to use simple movements to express themselves, such as pointing at things.[23] Three- to five-year-old autistic children are less likely to exhibit social understanding, approach others spontaneously, imitate and respond to emotions, communicate nonverbally, and take turns with others. However, they do form attachments to their primary caregivers.[24] Most autistic children displayed moderately less attachment security than neurotypical children, although this difference disappears in children with higher mental development or less pronounced autistic traits.[25] Children with high-functioning autism have more intense and frequent loneliness compared to non-autistic peers, despite the common belief that autistic children prefer to be alone. Making and maintaining friendships often proves to be difficult for autistic people. For them, the quality of friendships, not the number of friends, predicts how lonely they feel. Functional friendships, such as those resulting in invitations to parties, may affect the quality of life more deeply.[26]
Communication
Differences in communication may be present from the first year of life, and may include delayed onset of babbling, unusual gestures, diminished responsiveness, and vocal patterns that are not synchronized with the caregiver. In the second and third years, autistic children have less frequent and less diverse babbling, consonants, words, and word combinations; their gestures are less often integrated with words. Autistic children are less likely to make requests or share experiences, and are more likely to simply repeat others' words (echolalia)[27] or reverse pronouns.[28] Deficits in joint attention may be present - for example, they may look at a pointing hand instead of the object to which the hand is pointing.[23] Autistic children may have difficulty with imaginative play and with developing symbols into language.[27]
Repetitive behavior

Autistic individuals can display many forms of repetitive or restricted behavior, which the Repetitive Behavior Scale-Revised (RBS-R) categorizes as follows.[29]
- Stereotyped behaviors: Repetitive movements, such as hand flapping, head rolling, or body rocking.
- Compulsive behaviors: Time-consuming behaviors intended to reduce the anxiety that an individual feels compelled to perform repeatedly or according to rigid rules, such as placing objects in a specific order, checking things, or handwashing.
- Sameness: Resistance to change; for example, insisting that the furniture not be moved or refusing to be interrupted.
- Ritualistic behavior: Unvarying pattern of daily activities, such as an unchanging menu or a dressing ritual.
- Restricted interests: Interests or fixations that are abnormal in theme or intensity of focus, such as preoccupation with a single television program, toy, or game.
No single repetitive or self-injurious behavior seems to be specific to autism, but autism appears to have an elevated pattern of occurrence and severity of these behaviors.[30]
Other symptoms
Autistic individuals may have symptoms that are independent of the diagnosis.[21] An estimated 0.5% to 10% of individuals with classic autism show unusual abilities, ranging from splinter skills such as the memorization of trivia to the extraordinarily rare talents of prodigious autistic savants.[31] Sensory abnormalities are found in over 90% of autistic people, and are considered core features by some,[21] although there was no good evidence that sensory symptoms differentiate autism from other developmental disorders.[32] An estimated 60–80% of autistic people have motor signs that include poor muscle tone, poor motor planning, and toe walking.[21]
Causes
It was presumed initially that there was a common cause at the genetic, cognitive, and neural levels for classic autism's characteristic triad of symptoms.[33] However, over time, there was increasing evidence that autism was instead a complex and highly heritable disorder whose core aspects have distinct causes which often often co-occur.[33][34][35]
Although theories regarding vaccines lack convincing scientific evidence, are biologically implausible,[36] and originated from a fraudulent study,[37] parental concern about a potential vaccine link with autism (and subsequent concern about ASD) has led to lower rates of childhood immunizations, outbreaks of previously controlled childhood diseases in some countries, and the preventable deaths of several children.[38][39]
Diagnosis
Diagnosis of classic autism was based on behavioral symptoms, not cause or mechanism.[22][40]
Classification
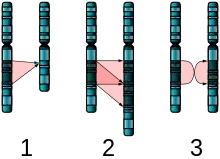
Classic autism was listed as autistic disorder in the fourth edition of the American Psychiatric Association's diagnostic manual, as one of the five pervasive developmental disorders (PDDs).[10] However, the PDDs were collapsed into the single diagnosis of Autism Spectrum Disorder in 2013,[10] and the WHO's diagnostic manual ICD-11 (which had listed it as childhood autism in its previous edition[41]) followed suit a few years later.[42] Classic autism was said to be characterized by widespread abnormalities of social interactions and communication, severely restricted interests, and highly repetitive behavior.[17]
Of the PDDs, Asperger syndrome was closest to classic autism in signs and likely causes; Rett syndrome and childhood disintegrative disorder share several signs with it, but were understood to potentially have unrelated causes; PDD not otherwise specified (PDD-NOS; also called atypical autism) was diagnosed when the criteria were not met for one of the other four PDDs.[43] People would usually attract a diagnosis of Asperger syndrome rather than classic autism if they showed no substantial delay in language development,[44] but early language ability was found to be a poor predictor of outcomes in adulthood.[45]
Prognosis and management

There is no known cure for autism,[6] and very little research addressed long-term prognosis for classic autism.[47] Many autistic children lack social support, future employment opportunities or self-determination.[26]
The main goals when treating autistic children are to lessen associated deficits and family distress, and to increase quality of life and functional independence. In general, higher IQs are correlated with greater responsiveness to treatment and improved treatment outcomes.[48] Services should be carried out by behavior analysts, special education teachers, speech pathologists, and licensed psychologists.
Intensive, sustained special education programs and behavior therapy early in life often improves functioning and decreases symptom severity and maladaptive behaviors;[49] claims that intervention by around age three years is crucial are not substantiated.[50]
No known medication relieves autism's core symptoms of social and communication impairments.
Education
Early, intensive ABA therapy has demonstrated effectiveness in enhancing communication and adaptive functioning in preschool children;[51] it is also well-established for improving the intellectual performance of that age group.[49][51] It is not known whether treatment programs for children lead to significant improvements after the children grow up,[49] and the limited research on the effectiveness of adult residential programs shows mixed results.[52]
Alternative medicine
Although many alternative therapies and interventions were used, few are supported by scientific studies.[53] Treatment approaches have little empirical support in quality-of-life contexts, and many programs focus on success measures that lack predictive validity and real-world relevance.[26] Some alternative treatments placed autistic individuals at risk.[54] For example, in 2005, a five-year-old child with autism was killed by botched chelation therapy (which is not recommended for autism as risks outweigh any potential benefits).[55][56][57]
Epidemiology
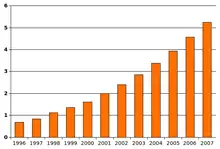
Globally, classic autism was understood to affect an estimated 24.8 million people as of 2015.[9] After it was recognised as a distinct disorder, reports of autism cases substantially increased, which was largely attributable to changes in diagnostic practices, referral patterns, availability of services, age at diagnosis, and public awareness[58][59] (particularly among women).[60]
Several other conditions were commonly seen in children with autism. They include:
- Intellectual disability. The percentage of autistic individuals who also met criteria for intellectual disability has been reported as anywhere from 25% to 70%, a wide variation illustrating the difficulty of assessing intelligence of individuals on the autism spectrum.[61] In comparison, for PDD-NOS the association with intellectual disability was much weaker,[62] and by definition, the diagnosis of Asperger's excluded intellectual disability.[63]
- Minor physical anomalies are significantly increased in the autistic population.[64]
- Preempted diagnoses. Although the DSM-IV ruled out the concurrent diagnosis of many other conditions along with autism, the full criteria for Attention deficit hyperactivity disorder (ADHD), Tourette syndrome, and other of these conditions were often present. As a result, modern ASD allows for these diagnoses.[3]
History

The New Latin word autismus (English translation autism) was coined by the Swiss psychiatrist Eugen Bleuler in 1910 as he was defining symptoms of schizophrenia. He derived it from the Greek word autós (αὐτός, meaning "self"), and used it to mean morbid self-admiration, referring to "autistic withdrawal of the patient to his fantasies, against which any influence from outside becomes an intolerable disturbance".[66] The word autism first took its modern sense in 1938 when Hans Asperger of the Vienna University Hospital adopted Bleuler's terminology autistic psychopaths in a lecture in German about child psychology.[67] Asperger was investigating Asperger syndrome which, for various reasons, was not widely considered a separate diagnosis until 1981,[65] although both are now considered part of ASD. Leo Kanner of the Johns Hopkins Hospital first used autism in English to refer to classic autism when he introduced the label early infantile autism in a 1943 report.[28] Almost all the characteristics described in Kanner's first paper on the subject, notably "autistic aloneness" and "insistence on sameness", are still regarded as typical of the autistic spectrum of disorders.[34] Starting in the late 1960s, classic autism was established as a separate syndrome.[68]
It took until 1980 for the DSM-III to differentiate autism from childhood schizophrenia. In 1987, the DSM-III-R provided a checklist for diagnosing autism. In May 2013, the DSM-5 was released, updating the classification for pervasive developmental disorders. The grouping of disorders, including PDD-NOS, autism, Asperger syndrome, Rett syndrome, and CDD, has been removed and replaced with the general term of Autism Spectrum Disorder.[69]
References
- Landa RJ (March 2008). "Diagnosis of autism spectrum disorders in the first 3 years of life". Nature Clinical Practice. Neurology. 4 (3): 138–147. doi:10.1038/ncpneuro0731. PMID 18253102.
- "NIMH " Autism Spectrum Disorder". nimh.nih.gov. October 2016. Retrieved 20 April 2017.
- American Psychiatric Association (2013). "Autism Spectrum Disorder, 299.00 (F84.0)". Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). American Psychiatric Publishing. pp. 50–59.
- Chaste P, Leboyer M (September 2012). "Autism risk factors: genes, environment, and gene-environment interactions". Dialogues in Clinical Neuroscience. 14 (3): 281–292. doi:10.31887/DCNS.2012.14.3/pchaste. PMC 3513682. PMID 23226953.
- Corcoran J, Walsh J (9 February 2006). Clinical Assessment and Diagnosis in Social Work Practice. Oxford University Press, New York. p. 72. ISBN 978-0-19-516830-3. LCCN 2005027740. OCLC 466433183.
- Myers SM, Johnson CP (November 2007). "Management of children with autism spectrum disorders". Pediatrics. 120 (5): 1162–1182. doi:10.1542/peds.2007-2362. PMID 17967921.
- Sukhodolsky DG, Bloch MH, Panza KE, Reichow B (November 2013). "Cognitive-behavioral therapy for anxiety in children with high-functioning autism: a meta-analysis". Pediatrics. 132 (5): e1341–e1350. doi:10.1542/peds.2013-1193. PMC 3813396. PMID 24167175.
- Ji N, Findling RL (March 2015). "An update on pharmacotherapy for autism spectrum disorder in children and adolescents". Current Opinion in Psychiatry. 28 (2): 91–101. doi:10.1097/YCO.0000000000000132. PMID 25602248. S2CID 206141453.
- Vos, Theo; et al. (GBD 2015 Disease and Injury Incidence and Prevalence Collaborators) (October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
- Rosen NE, Lord C, Volkmar FR (December 2021). "The Diagnosis of Autism: From Kanner to DSM-III to DSM-5 and Beyond". Journal of Autism and Developmental Disorders. 51 (12): 4253–4270. doi:10.1007/s10803-021-04904-1. PMC 8531066. PMID 33624215.
- "Autism". National Institute for Health and Care Excellence. UK. Retrieved 2022-03-17.
- Fletcher-Watson S (2019). Autism: a new introduction to psychological theory and current debates. Francesca Happé ([New edition; Updated edition] ed.). Abingdon, Oxon. ISBN 978-1-315-10169-9. OCLC 1073035060.
- Tick B, Bolton P, Happé F, Rutter M, Rijsdijk F (May 2016). "Heritability of autism spectrum disorders: a meta-analysis of twin studies". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 57 (5): 585–595. doi:10.1111/jcpp.12499. PMC 4996332. PMID 26709141.
- Taylor LE, Swerdfeger AL, Eslick GD (June 2014). "Vaccines are not associated with autism: an evidence-based meta-analysis of case-control and cohort studies". Vaccine. 32 (29): 3623–3629. doi:10.1016/j.vaccine.2014.04.085. PMID 24814559.
- Rutter M (January 2005). "Incidence of autism spectrum disorders: changes over time and their meaning". Acta Paediatrica. 94 (1): 2–15. doi:10.1111/j.1651-2227.2005.tb01779.x. PMID 15858952. S2CID 79259285.
- Geschwind DH (October 2008). "Autism: many genes, common pathways?". Cell. 135 (3): 391–395. doi:10.1016/j.cell.2008.10.016. PMC 2756410. PMID 18984147.
- "F84. Pervasive developmental disorders". ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision. World Health Organization. 2007. Archived from the original on 21 April 2013. Retrieved 10 October 2009.
- Pinel JP (2011). Biopsychology (8th ed.). Boston, Massachusetts: Pearson. p. 235. ISBN 978-0-205-03099-6. OCLC 1085798897.
- Rogers SJ (June 2009). "What are infant siblings teaching us about autism in infancy?". Autism Research. 2 (3): 125–137. doi:10.1002/aur.81. PMC 2791538. PMID 19582867.
- Stefanatos GA (December 2008). "Regression in autistic spectrum disorders". Neuropsychology Review. 18 (4): 305–319. doi:10.1007/s11065-008-9073-y. PMID 18956241. S2CID 34658024.
- Geschwind DH (2009). "Advances in autism". Annual Review of Medicine. 60: 367–380. doi:10.1146/annurev.med.60.053107.121225. PMC 3645857. PMID 19630577.
- London E (October 2007). "The role of the neurobiologist in redefining the diagnosis of autism". Brain Pathology. 17 (4): 408–411. doi:10.1111/j.1750-3639.2007.00103.x. PMC 8095627. PMID 17919126. S2CID 24860348.
- Volkmar FR, Paul R, Pelphrey KA, Rogers SJ, eds. (2014). Handbook of Autism and Pervasive Developmental Disorders: Volume Two: Assessment, Interventions, and Policy. Vol. 2 (4th ed.). Hoboken, New Jersey: John Wiley & Sons. p. 301. ISBN 978-1-118-28220-5. LCCN 2013034363. OCLC 946133861. Retrieved 1 March 2019.
- Sigman M, Dijamco A, Gratier M, Rozga A (2004). "Early detection of core deficits in autism". Mental Retardation and Developmental Disabilities Research Reviews. 10 (4): 221–233. CiteSeerX 10.1.1.492.9930. doi:10.1002/mrdd.20046. PMID 15666338.
- Rutgers AH, Bakermans-Kranenburg MJ, van Ijzendoorn MH, van Berckelaer-Onnes IA (September 2004). "Autism and attachment: a meta-analytic review". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 45 (6): 1123–1134. doi:10.1111/j.1469-7610.2004.t01-1-00305.x. PMID 15257669.
- Burgess AF, Gutstein SE (May 2007). "Quality of Life for People with Autism: Raising the Standard for Evaluating Successful Outcomes" (PDF). Child and Adolescent Mental Health. 12 (2): 80–86. doi:10.1111/j.1475-3588.2006.00432.x. PMID 32811109. Archived from the original (PDF) on 3 December 2013. Retrieved 24 November 2013.
- Landa R (2007). "Early communication development and intervention for children with autism". Mental Retardation and Developmental Disabilities Research Reviews. 13 (1): 16–25. doi:10.1002/mrdd.20134. PMID 17326115.
- Kanner L (1943). "Autistic disturbances of affective contact". Acta Paedopsychiatrica. 35 (4): 100–136. PMID 4880460. Reprinted in Kanner L (1968). "Autistic disturbances of affective contact". Acta Paedopsychiatrica. 35 (4): 100–136. PMID 4880460.
- Lam KS, Aman MG (May 2007). "The Repetitive Behavior Scale-Revised: independent validation in individuals with autism spectrum disorders". Journal of Autism and Developmental Disorders. 37 (5): 855–866. doi:10.1007/s10803-006-0213-z. PMID 17048092. S2CID 41034513.
- Bodfish JW, Symons FJ, Parker DE, Lewis MH (June 2000). "Varieties of repetitive behavior in autism: comparisons to mental retardation". Journal of Autism and Developmental Disorders. 30 (3): 237–243. doi:10.1023/A:1005596502855. PMID 11055459. S2CID 16706630.
- Treffert DA (May 2009). "The savant syndrome: an extraordinary condition. A synopsis: past, present, future". Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 364 (1522): 1351–1357. doi:10.1098/rstb.2008.0326. PMC 2677584. PMID 19528017.
- Rogers SJ, Ozonoff S (December 2005). "Annotation: what do we know about sensory dysfunction in autism? A critical review of the empirical evidence". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 46 (12): 1255–1268. doi:10.1111/j.1469-7610.2005.01431.x. PMID 16313426.
- Happé F, Ronald A (December 2008). "The 'fractionable autism triad': a review of evidence from behavioural, genetic, cognitive and neural research". Neuropsychology Review. 18 (4): 287–304. doi:10.1007/s11065-008-9076-8. PMID 18956240. S2CID 13928876.
- Happé F, Ronald A, Plomin R (October 2006). "Time to give up on a single explanation for autism". Nature Neuroscience. 9 (10): 1218–1220. doi:10.1038/nn1770. PMID 17001340.
- Beaudet AL (May 2007). "Autism: highly heritable but not inherited". Nature Medicine. 13 (5): 534–536. doi:10.1038/nm0507-534. PMID 17479094. S2CID 11673879.
- Gerber JS, Offit PA (February 2009). "Vaccines and autism: a tale of shifting hypotheses". Clinical Infectious Diseases. 48 (4): 456–461. doi:10.1086/596476. PMC 2908388. PMID 19128068.
- Godlee F, Smith J, Marcovitch H (January 2011). "Wakefield's article linking MMR vaccine and autism was fraudulent". BMJ. 342: c7452. doi:10.1136/bmj.c7452. PMID 21209060. S2CID 43640126. Archived from the original on 11 November 2013.
- Vaccines and autism:
- Doja A, Roberts W (November 2006). "Immunizations and autism: a review of the literature". The Canadian Journal of Neurological Sciences. Le Journal Canadien des Sciences Neurologiques. 33 (4): 341–346. doi:10.1017/s031716710000528x. PMID 17168158.
- Gerber JS, Offit PA (February 2009). "Vaccines and autism: a tale of shifting hypotheses". Clinical Infectious Diseases. 48 (4): 456–461. doi:10.1086/596476. PMC 2908388. PMID 19128068.
- Gross L (May 2009). "A broken trust: lessons from the vaccine--autism wars". PLOS Biology. 7 (5): e1000114. doi:10.1371/journal.pbio.1000114. PMC 2682483. PMID 19478850.
- Paul R (June 2009). "Parents ask: Am I risking autism if I vaccinate my children?". Journal of Autism and Developmental Disorders. 39 (6): 962–963. doi:10.1007/s10803-009-0739-y. PMID 19363650. S2CID 34467853.
- Poland GA, Jacobson RM (January 2011). "The age-old struggle against the antivaccinationists". The New England Journal of Medicine. 364 (2): 97–99. doi:10.1056/NEJMp1010594. PMID 21226573.
- McBrien J, Murphy J, Gill D, Cronin M, O'Donovan C, Cafferkey MT (July 2003). "Measles outbreak in Dublin, 2000". The Pediatric Infectious Disease Journal. 22 (7): 580–584. doi:10.1097/00006454-200307000-00002. PMID 12867830.
- Baird G, Cass H, Slonims V (August 2003). "Diagnosis of autism". BMJ. 327 (7413): 488–493. doi:10.1136/bmj.327.7413.488. PMC 188387. PMID 12946972.
- "ICD-10 Version:2016". icd.who.int. Retrieved 2022-04-28.
- "World Health Organisation updates classification of autism in the ICD-11 – Autism Europe". Retrieved 2022-04-28.
- Volkmar FR, State M, Klin A (January 2009). "Autism and autism spectrum disorders: diagnostic issues for the coming decade". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 50 (1–2): 108–115. doi:10.1111/j.1469-7610.2008.02010.x. PMID 19220594.
- "Diagnostic criteria for 299.00 Autistic Disorder". Diagnostic and statistical manual of mental disorders: DSM-IV (4th ed.). Washington, D.C.: American Psychiatric Association. 2000. ISBN 978-0-89042-025-6. LCCN 00024852. OCLC 768475353. Archived from the original on 29 October 2013 – via Centers for Disease Control.
- Howlin P (2003-02-01). "Outcome in High-Functioning Adults with Autism with and Without Early Language Delays: Implications for the Differentiation Between Autism and Asperger Syndrome". Journal of Autism and Developmental Disorders. 33 (1): 3–13. doi:10.1023/A:1022270118899. ISSN 1573-3432. PMID 12708575. S2CID 35817450.
- Powell K (August 2004). "Opening a window to the autistic brain". PLOS Biology. 2 (8): E267. doi:10.1371/journal.pbio.0020267. PMC 509312. PMID 15314667.
- Seltzer MM, Shattuck P, Abbeduto L, Greenberg JS (2004). "Trajectory of development in adolescents and adults with autism". Mental Retardation and Developmental Disabilities Research Reviews. 10 (4): 234–247. doi:10.1002/mrdd.20038. PMID 15666341.
- Eldevik S, Hastings RP, Hughes JC, Jahr E, Eikeseth S, Cross S (May 2009). "Meta-analysis of Early Intensive Behavioral Intervention for children with autism". Journal of Clinical Child and Adolescent Psychology. 38 (3): 439–450. CiteSeerX 10.1.1.607.9620. doi:10.1080/15374410902851739. PMID 19437303. S2CID 205873629.
- Rogers SJ, Vismara LA (January 2008). "Evidence-based comprehensive treatments for early autism". Journal of Clinical Child and Adolescent Psychology. 37 (1): 8–38. doi:10.1080/15374410701817808. PMC 2943764. PMID 18444052.
- Howlin P, Magiati I, Charman T (January 2009). "Systematic review of early intensive behavioral interventions for children with autism". American Journal on Intellectual and Developmental Disabilities. 114 (1): 23–41. doi:10.1352/2009.114:23-41. PMID 19143460.
- Eikeseth S (2009). "Outcome of comprehensive psycho-educational interventions for young children with autism". Research in Developmental Disabilities. 30 (1): 158–178. CiteSeerX 10.1.1.615.3336. doi:10.1016/j.ridd.2008.02.003. PMID 18385012.
- Van Bourgondien ME, Reichle NC, Schopler E (April 2003). "Effects of a model treatment approach on adults with autism". Journal of Autism and Developmental Disorders. 33 (2): 131–140. doi:10.1023/A:1022931224934. PMID 12757352. S2CID 30125359.
- Sigman M, Spence SJ, Wang AT (2006). "Autism from developmental and neuropsychological perspectives". Annual Review of Clinical Psychology. 2: 327–355. doi:10.1146/annurev.clinpsy.2.022305.095210. PMID 17716073.
- Tye C, Runicles AK, Whitehouse AJ, Alvares GA (2019). "Characterizing the Interplay Between Autism Spectrum Disorder and Comorbid Medical Conditions: An Integrative Review". Frontiers in Psychiatry (Review). 9: 751. doi:10.3389/fpsyt.2018.00751. PMC 6354568. PMID 30733689.
- Levy SE, Hyman SL (October 2008). "Complementary and alternative medicine treatments for children with autism spectrum disorders". Child and Adolescent Psychiatric Clinics of North America (Review). 17 (4): 803–20, ix. doi:10.1016/j.chc.2008.06.004. PMC 2597185. PMID 18775371.
- Brown MJ, Willis T, Omalu B, Leiker R (August 2006). "Deaths resulting from hypocalcemia after administration of edetate disodium: 2003-2005". Pediatrics. 118 (2): e534–e536. doi:10.1542/peds.2006-0858. PMID 16882789. S2CID 28656831. Archived from the original on 27 July 2009.
- James S, Stevenson SW, Silove N, Williams K (May 2015). James S (ed.). "Chelation for autism spectrum disorder (ASD)". The Cochrane Database of Systematic Reviews (Review) (5): CD010766. doi:10.1002/14651858.CD010766. PMID 26106752.
- Fombonne E (June 2009). "Epidemiology of pervasive developmental disorders". Pediatric Research. 65 (6): 591–598. doi:10.1203/PDR.0b013e31819e7203. PMID 19218885.
- Gernsbacher MA, Dawson M, Goldsmith HH (April 2005). "Three Reasons Not to Believe in an Autism Epidemic". Current Directions in Psychological Science. 14 (2): 55–58. doi:10.1111/j.0963-7214.2005.00334.x. PMC 4232964. PMID 25404790.
- Russell G, Stapley S, Newlove-Delgado T, Salmon A, White R, Warren F, et al. (August 2021). "Time trends in autism diagnosis over 20 years: a UK population-based cohort study". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 63 (6): 674–682. doi:10.1111/jcpp.13505. PMID 34414570. S2CID 237242123.
The figure starkly illustrates an overall 787% increase in recorded incidence of autism diagnosis over 20 years.
- Dawson M, Mottron L, Gernsbacher MA (2008). "Learning in autism" (PDF). In Byrne JH, Roediger HL (eds.). Learning and Memory: A Comprehensive Reference. Vol. 2. Elsevier. pp. 759–772. doi:10.1016/B978-012370509-9.00152-2. ISBN 978-0-12-370504-4. OCLC 775005136. Archived from the original (PDF) on 3 March 2012. Retrieved 26 July 2008.
- Chakrabarti S, Fombonne E (June 2001). "Pervasive developmental disorders in preschool children". JAMA. 285 (24): 3093–3099. doi:10.1001/jama.285.24.3093. PMID 11427137.
- Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR). Washington, D.C.: American Psychiatric Association. 2000. p. 80.
- Ozgen HM, Hop JW, Hox JJ, Beemer FA, van Engeland H (March 2010). "Minor physical anomalies in autism: a meta-analysis". Molecular Psychiatry. 15 (3): 300–307. doi:10.1038/mp.2008.75. PMID 18626481.
- Wolff S (August 2004). "The history of autism". European Child & Adolescent Psychiatry. 13 (4): 201–208. doi:10.1007/s00787-004-0363-5. PMID 15365889. S2CID 6106042.
- Kuhn R (September 2004). "Eugen Bleuler's concepts of psychopathology". History of Psychiatry. 15 (59 Pt 3): 361–366. doi:10.1177/0957154X04044603. PMID 15386868. S2CID 5317716. The quote is a translation of Bleuler's 1910 original.
- Asperger H (1938). "Das psychisch abnormale Kind" [The psychically abnormal child]. Wien Klin Wochenschr (in German). 51: 1314–1317.
- Fombonne E (September 2003). "Modern views of autism". Canadian Journal of Psychiatry. 48 (8): 503–505. doi:10.1177/070674370304800801. PMID 14574825. S2CID 8868418.
- Baker JP (September 2013). "Autism at 70--redrawing the boundaries" (PDF). The New England Journal of Medicine. 369 (12): 1089–1091. doi:10.1056/NEJMp1306380. PMID 24047057. S2CID 44613078. Archived from the original (PDF) on 3 March 2019.
External links
| Library resources about Classic autism |