High-functioning autism
High-functioning autism (HFA) is an autism classification where a person exhibits no intellectual disability, but may exhibit deficits in communication, emotion recognition and expression, and social interaction.[11][12][13] HFA is not included in either the American Psychological Association's DSM-5 or the World Health Organization's ICD-10, neither of which subdivides autism based on intellectual capabilities.
| High-functioning autism | |
|---|---|
| Other names | Sukhareva Syndrome[1] |
| Specialty | Psychiatry |
| Symptoms | Trouble with social interaction, impaired communication, restricted interests, repetitive behavior |
| Complications | Social isolation, employment problems, family stress, being bullied, self-harm[2] |
| Usual onset | By age two or three[3][4] |
| Duration | Long-term |
| Causes | Genetic and environmental factors |
| Diagnostic method | Based on behavior and developmental history |
| Differential diagnosis | Asperger syndrome, ADHD, Tourette syndrome, anxiety, bipolar disorder, obsessive–compulsive disorder |
| Treatment | Behavioral therapy, speech therapy, psychotropic medication[5][6][7] |
| Medication | Antipsychotics, antidepressants, stimulants (associated symptoms)[8][9][10] |
Characterization
High-functioning autism is characterized by features similar to those of Asperger syndrome. The defining characteristic recognized by psychologists is a significant delay in the development of early speech and language skills, before the age of three years.[12] The diagnostic criteria of Asperger syndrome exclude a general language delay.[14]
Further differences in features of people with high-functioning autism from those with Asperger syndrome include the following:[12][15][16][17]
- Lower verbal reasoning ability
- Better visual/spatial skills (higher performance IQ)
- Less deviating locomotion (e.g. clumsiness)
- Problems functioning independently
- Curiosity and interest for many different things
- Not as good at empathizing with other people
- Male to female ratio (4:1) much smaller
As of 2013, Asperger Syndrome and High-functioning autism are no longer terms used by the American Psychological Association, and have instead both been merged into autism spectrum disorder (ASD).[18][19][20] As of 2021, the World Health Organization also retired the terms and merged them into autism spectrum disorder.[21][22]
Comorbidities
Individuals with autism spectrum disorders, including high-functioning autism, risk developing symptoms of anxiety. While anxiety is one of the most commonly occurring mental health symptoms, children and adolescents with high functioning autism are at an even greater risk of developing symptoms.[23]
There are other comorbidities, the presence of one or more disorders in addition to the primary disorder, associated with high-functioning autism. Some of these include bipolar disorder and obsessive–compulsive disorder (OCD). In particular the link between HFA and OCD, has been studied; both have abnormalities associated with serotonin.[24]
Observable comorbidities associated with HFA include ADHD and Tourette syndrome. HFA does not cause, nor include, intellectual disabilities. This characteristic distinguishes HFA from low-functioning autism; between 40 and 55% of individuals with autism also have an intellectual disability.[25]
Behavior
An association between HFA and criminal behavior is not completely characterized. Several studies have shown that the features associated with HFA may increase the probability of engaging in criminal behavior.[24] While there is still a great deal of research that needs to be done in this area, recent studies on the correlation between HFA and criminal actions suggest that there is a need to understand the attributes of HFA that may lead to violent behavior. There have been several case studies that link the lack of empathy and social naïveté associated with HFA to criminal actions.[26]
There is still a need for more research on the link between HFA and crimes, because many other studies point out that most people with ASD are more likely to be victims and less likely to commit crimes than the general population. But there are also small-subgroups of people with autism that commit crimes because they lack understanding of the laws they have broken.[27] Misunderstandings are especially common regarding autism and sex offenses, since many people with autism do not receive sex education.[28]
Cause
Although little is known about the biological basis of autism, studies have revealed structural abnormalities in specific brain regions. Regions identified in the "social" brain include the amygdala, superior temporal sulcus, fusiform gyrus area and orbitofrontal cortex. Further abnormalities have been observed in the caudate nucleus, believed to be involved in restrictive behaviors, as well as in a significant increase in the amount of cortical grey matter and atypical connectivity between brain regions.[29]
Diagnosis and IQ
HFA is not a recognised diagnosis by the American Psychological Association (DSM-5) or the World Health Organization (ICD-10). HFA is often, however, used in clinical settings to describe a set of symptoms related to an autism spectrum disorder whereby they exhibit standard autism indicators although have an intelligence quotient (IQ) of 70 or greater.[30]
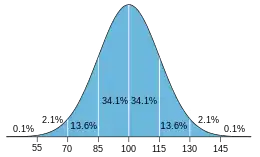
For modern IQ tests, the raw score is transformed to a normal distribution with mean 100 and standard deviation 15.[31] This results in approximately two-thirds of the population scoring between IQ 85 and IQ 115 and about 2.5 percent each above 130 and below 70.[32][33]
IQ scales are ordinally scaled.[34][35][36][37][38] The raw score of the norming sample is usually (rank order) transformed to a normal distribution with mean 100 and standard deviation 15.[31] While one standard deviation is 15 points, and two SDs are 30 points, and so on, this does not imply that mental ability is linearly related to IQ, such that IQ 50 would mean half the cognitive ability of IQ 100. In particular, IQ points are not percentage points.
A diagnosis of intellectual disability is in part based on the results of IQ testing. Borderline intellectual functioning is the categorization of individuals of below-average cognitive ability (an IQ of 71–85), although not as low as those with an intellectual disability (70 or below).
People with high IQs are found at all levels of education and occupational categories. The biggest difference occurs for low IQs with only an occasional college graduate or professional scoring below 90.[39]
Treatment
While there exists no single treatment or medicine for people with autism, there exists several strategies to help lessen the symptoms and effects of the condition.
Augmentative and alternative communication
Augmentative and alternative communication (AAC) is used for autistic people who cannot communicate orally. People who have problems speaking may be taught to use other forms of communication, such as body language, computers, interactive devices, and pictures.[40] The Picture Exchange Communication System (PECS) is a commonly used form of augmentative and alternative communication with children and adults who cannot communicate well orally. People are taught how to link pictures and symbols to their feelings, desires and observation, and may be able to link sentences together with the vocabulary that they form.[41]
Speech-language therapy
Speech–language therapy can help those with autism who need to develop or improve communication skills.[42] According to the organization Autism Speaks, "speech-language therapy is designed to coordinate the mechanics of speech with the meaning and social use of speech".[41] People with autism may have issues with communication, or speaking spoken words. Speech-language pathologists (SLP) may teach someone how to communicate more effectively with others or work on starting to develop speech patterns.[43] The SLP will create a plan that focuses on what the child needs.
Occupational therapy
Occupational therapy helps autistic children and adults learn everyday skills that help them with daily tasks, such as personal hygiene and movement. These skills are then integrated into their home, school, and work environments. Therapists will oftentimes help people learn to adapt their environment to their skill level.[44] This type of therapy could help autistic people become more engaged in their environment.[41] An occupational therapist will create a plan based on a person's needs and desires and work with them to achieve their set goals.
Applied behavioral analysis (ABA)
Applied behavior analysis (ABA) is considered the most effective therapy for autism spectrum disorders by the American Academy of Pediatrics.[45] ABA focuses on teaching adaptive behaviors like social skills, play skills, or communication skills[46][47] and diminishing problematic behaviors such as self-injury[48] by creating a specialized plan that uses behavioral therapy techniques, such as positive or negative reinforcement, to encourage or discourage certain behaviors over-time.[49] However, ABA has been strongly criticised by the autistic community, who view it as abusive and detrimental to autistic children's growth.[50][51][52]
Sensory integration therapy
Sensory integration therapy helps people with autism adapt to different kinds of sensory stimuli. Many with autism can be oversensitive to certain stimuli, such as lights or sounds, causing them to overreact. Others may not react to certain stimuli, such as someone speaking to them.[53] Many types of therapy activities involve a form of play, such as using swings, toys and trampolines to help engage people with sensory stimuli.[41] Therapists will create a plan that focuses on the type of stimulation the person needs integration with.
Neurofeedback
Studies suggest Neurofeedback alleviates certain symptoms of autism, such as emotional outbursts, hyperactivity, resistance to change, and stimming. Although considered a safe, non-invasive procedure, it may potentially involve some side effects. [54]
Criticism of functioning labels
Many medical professionals, autistic people, and supporters of autistic rights disagree with the categorisation of individuals into "high-functioning autism" and "low-functioning autism", stating that the "low-functioning" label causes people to put low expectations on a child and view them as lesser.[57][58] Furthermore, critics of functioning labels state that an individual's functioning can fluctuate from day to day, and categories do not take this into consideration.[58][59] Levels of functioning are unrelated to intellectual disability.[58] Additionally, individuals with "medium-functioning autism" are typically left out of the discussion entirely, and due to the non-linear nature of the autistic spectrum, individuals can be high-functioning in some areas while at the same time being medium or low functioning in other areas.[60]
See also
- Asperger syndrome and neuroscience
- Autism-spectrum quotient, a self-administered test for high-functioning autism
- Historical figures sometimes considered autistic
- Low-functioning autism
- Nonverbal learning disorder
- Lorna Wing
References
- Manouilenko I, Bejerot S (August 2015). "Sukhareva – Prior to Asperger and Kanner". Nordic Journal of Psychiatry (Report) (published 31 March 2015). 69 (6): 479–82. doi:10.3109/08039488.2015.1005022. PMID 25826582. S2CID 207473133.
- "Autism spectrum disorder - Symptoms and causes". Mayo Clinic. Archived from the original on 14 July 2019. Retrieved 13 July 2019.
- "NIMH " Autism Spectrum Disorder". nimh.nih.gov. October 2016. Archived from the original on 21 April 2017. Retrieved 20 April 2017.
- American Psychiatric Association (2013). "Autism Spectrum Disorder. 299.00 (F84.0)". Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Arlington, VA: American Psychiatric Publishing. pp. 50–59. doi:10.1176/appi.books.9780890425596. hdl:2027.42/138395. ISBN 978-0-89042-559-6.
- Myers SM, Johnson CP (November 2007). "Management of children with autism spectrum disorders". Pediatrics. 120 (5): 1162–82. doi:10.1542/peds.2007-2362. PMID 17967921. Archived from the original on 2019-03-23. Retrieved 2019-05-24.
- Sanchack, KE; Thomas, CA (15 December 2016). "Autism Spectrum Disorder: Primary Care Principles". American Family Physician. 94 (12): 972–79. PMID 28075089.
- Sukhodolsky, DG; Bloch, MH; Panza, KE; Reichow, B (November 2013). "Cognitive-behavioral therapy for anxiety in children with high-functioning autism: a meta-analysis". Pediatrics. 132 (5): e1341–50. doi:10.1542/peds.2013-1193. PMC 3813396. PMID 24167175.
- Ji N, Findling RL (March 2015). "An update on pharmacotherapy for autism spectrum disorder in children and adolescents". Current Opinion in Psychiatry. 28 (2): 91–101. doi:10.1097/YCO.0000000000000132. PMID 25602248. S2CID 206141453.
- Oswald DP, Sonenklar NA (June 2007). "Medication use among children with autism spectrum disorders". Journal of Child and Adolescent Psychopharmacology. 17 (3): 348–55. doi:10.1089/cap.2006.17303. PMID 17630868.
- Jaeggi, S. M.; Buschkuehl, M.; Jonides, J.; Perrig, W. J. (2008). "From the Cover: Improving fluid intelligence with training on working memory". Proceedings of the National Academy of Sciences. 105 (19): 6829–33. Bibcode:2008PNAS..105.6829J. doi:10.1073/pnas.0801268105. PMC 2383929. PMID 18443283.
- Sanders, James Ladell (2009). "Qualitative or Quantitative Differences Between Asperger's Disorder and Autism? Historical Considerations". Journal of Autism and Developmental Disorders. 39 (11): 1560–1567. doi:10.1007/s10803-009-0798-0. ISSN 0162-3257. PMID 19548078. S2CID 26351778.
- Carpenter, Laura Arnstein; Soorya, Latha; Halpern, Danielle (2009). "Asperger's Syndrome and High-Functioning Autism". Pediatric Annals. 38 (1): 30–5. doi:10.3928/00904481-20090101-01. PMID 19213291.
- Andari, Elissar; Duhamel, Jean-René; Zalla, Tiziana; Herbrecht, Evelyn; Leboyer, Marion; Sirigu, Angela (2 March 2019). "Promoting social behavior with oxytocin in highfunctioning autism spectrum disorders" (PDF). PNAS. 107 (9): 4389–4394. doi:10.1073/pnas.0910249107. PMC 2840168. PMID 20160081.
- Asperger's Disorder Archived 2013-04-25 at archive.today – Diagnostic and Statistical Manual of Mental Disorders Fourth edition Text Revision (DSM-IV-TR) American Psychiatric Association (2000)
- "News and general information | Finance, High tech, Health, ..." (PDF). March 14, 2022. Archived from the original on August 9, 2007.
- Rinehart, NJ; Bradshaw, JL; Brereton, AV; Tonge, BJ (2002). "Lateralization in individuals with high-functioning autism and Asperger's disorder: A frontostriatal model". Journal of Autism and Developmental Disorders. 32 (4): 321–331. doi:10.1023/A:1016387020095. PMID 12199137. S2CID 23067447.
- Mazefsky, Carla A.; Oswald, Donald P. (2006). "Emotion Perception in Asperger's Syndrome and High-functioning Autism: The Importance of Diagnostic Criteria and Cue Intensity". Journal of Autism and Developmental Disorders. 37 (6): 1086–95. doi:10.1007/s10803-006-0251-6. PMID 17180461. S2CID 12094187.
- "Neurodevelopmental Disorders". Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Washington, DC: American Psychiatric Association. 18 March 2022. ISBN 9780890425770. LCCN 2021051782.
- "6A02 Autism spectrum disorder". International Classification of Diseases 11th Revision (ICD-11). World Health Organisation. February 2022 [adopted in 2019]. 6A02. Retrieved 14 May 2022.
- "Asperger syndrome". Genetic and Rare Diseases Information Center (GARD) – an NCATS Program. Retrieved 26 January 2019.
- "ICD-11". icd.who.int. Retrieved 2022-04-10.
- "World Health Organisation updates classification of autism in the ICD-11". autismeurope. Retrieved 2022-04-10.
- Reaven, Judy (2011). "The treatment of anxiety symptoms in youth with high-functioning autism spectrum disorders: Developmental considerations for parents". Brain Research. 1380: 255–63. doi:10.1016/j.brainres.2010.09.075. PMID 20875799. S2CID 5226904.
- Mazzone, Luigi; Ruta, Liliana; Reale, Laura (2012). "Psychiatric comorbidities in asperger syndrome and high functioning autism: Diagnostic challenges". Annals of General Psychiatry. 11 (1): 16. doi:10.1186/1744-859X-11-16. PMC 3416662. PMID 22731684.
- Newschaffer, Craig J.; Croen, Lisa A.; Daniels, Julie; Giarelli, Ellen; Grether, Judith K.; Levy, Susan E.; Mandell, David S.; Miller, Lisa A.; Pinto-Martin, Jennifer; Reaven, Judy; Reynolds, Ann M.; Rice, Catherine E.; Schendel, Diana; Windham, Gayle C. (2007). "The Epidemiology of Autism Spectrum Disorders*". Annual Review of Public Health. 28 (1): 235–258. doi:10.1146/annurev.publhealth.28.021406.144007. ISSN 0163-7525. PMID 17367287.
- Lerner, Matthew D.; Haque, Omar Sultan; Northrup, Eli C.; Lawer, Lindsay; Bursztajn, Harold J. (2012). "Emerging Perspectives on Adolescents and Young Adults With High-Functioning Autism Spectrum Disorders, Violence, and Criminal Law". Journal of the American Academy of Psychiatry and the Law. 40 (2): 177–90. PMID 22635288.
- "Autism Myths & Misconceptions" (PDF). Retrieved 2021-08-05.
- Moyer, Melinda Wenner (2019-07-09). "When autistic people commit sexual crimes". Spectrum News. Retrieved 2021-08-05.
- Spencer, Michael; Stanfield, Andrew; Johnstone, Eve (2011). "Brain imaging and the neuroanatomical correlates of autism". In Roth, Ilona; Rezaie, Payam (eds.). Researching the Autism Spectrum. pp. 112–55. doi:10.1017/CBO9780511973918.006. ISBN 978-0-511-97391-8.
- de Giambattista, Concetta (2019). "Subtyping the Autism Spectrum Disorder: Comparison of Children with High Functioning Autism and Asperger Syndrome". Journal of Autism and Developmental Disorders. 49 (1): 138–150. doi:10.1007/s10803-018-3689-4. PMC 6331497. PMID 30043350.
- Gottfredson 2009, pp. 31–32
- Neisser, Ulrich (1997). "Rising Scores on Intelligence Tests". American Scientist. 85 (5): 440–447. Bibcode:1997AmSci..85..440N. Archived from the original on 4 November 2016. Retrieved 1 December 2017.
- Hunt 2011, p. 5 "As mental testing expanded to the evaluation of adolescents and adults, however, there was a need for a measure of intelligence that did not depend upon mental age. Accordingly the intelligence quotient (IQ) was developed. ... The narrow definition of IQ is a score on an intelligence test ... where 'average' intelligence, that is the median level of performance on an intelligence test, receives a score of 100, and other scores are assigned so that the scores are distributed normally about 100, with a standard deviation of 15. Some of the implications are that: 1. Approximately two-thirds of all scores lie between 85 and 115. 2. Five percent (1/20) of all scores are above 125, and one percent (1/100) are above 135. Similarly, five percent are below 75 and one percent below 65."
- Mussen, Paul Henry (1973). Psychology: An Introduction. Lexington, MA: Heath. p. 363. ISBN 978-0-669-61382-7.
The I.Q. is essentially a rank; there are no true "units" of intellectual ability.
- Truch, Steve (1993). The WISC-III Companion: A Guide to Interpretation and Educational Intervention. Austin, TX: Pro-Ed. p. 35. ISBN 978-0-89079-585-9.
An IQ score is not an equal-interval score, as is evident in Table A.4 in the WISC-III manual.
- Bartholomew, David J. (2004). Measuring Intelligence: Facts and Fallacies. Cambridge: Cambridge University Press. p. 50. ISBN 978-0-521-54478-8.
When we come to quantities like IQ or g, as we are presently able to measure them, we shall see later that we have an even lower level of measurement—an ordinal level. This means that the numbers we assign to individuals can only be used to rank them—the number tells us where the individual comes in the rank order and nothing else.
- Mackintosh 1998, pp. 30–31 "In the jargon of psychological measurement theory, IQ is an ordinal scale, where we are simply rank-ordering people. ... It is not even appropriate to claim that the 10-point difference between IQ scores of 110 and 100 is the same as the 10-point difference between IQs of 160 and 150"
- Stevens, S. S. (1946). "On the Theory of Scales of Measurement". Science. 103 (2684): 677–680. Bibcode:1946Sci...103..677S. doi:10.1126/science.103.2684.677. PMID 17750512. S2CID 4667599.
- Kaufman 2009
- "Augmentative and Alternative Communication (AAC)". American Speech-Language-Hearing Association. Archived from the original on 2019-08-15. Retrieved 2019-08-20.
- "What Treatments are Available for Speech, Language and Motor Issues?". Autism Speaks. Archived from the original on 2015-12-22. Retrieved 2015-12-16.
- "What is Autism, Asperger Syndrome, and Pervasive Developmental Disorders?". US Autism and Asperger Association. Archived from the original on 28 December 2015. Retrieved 16 December 2015.
- "Speech and Language Therapy". Autism Education Trust. Archived from the original on June 26, 2018.
- "Occupational Therapy's Role with Autism" (PDF). American Occupational Therapy Association. Retrieved April 3, 2022.
- Myers, Scott M.; Johnson, Chris Plauché (1 November 2007). "Management of Children With Autism Spectrum Disorders". Pediatrics. 120 (5): 1162–1182. doi:10.1542/peds.2007-2362. ISSN 0031-4005. PMID 17967921. Archived from the original on 9 October 2019. Retrieved 20 August 2019.
- "Applied Behavioral Analysis (ABA): What is ABA?". Autism partnership. Archived from the original on 2019-01-03. Retrieved 2019-08-20.
- Matson, Johnny; Hattier, Megan; Belva, Brian (January–March 2012). "Treating adaptive living skills of persons with autism using applied behavior analysis: A review". Research in Autism Spectrum Disorders. 6 (1): 271–276. doi:10.1016/j.rasd.2011.05.008.
- Summers, Jane; Sharami, Ali; Cali, Stefanie; D'Mello, Chantelle; Kako, Milena; Palikucin-Reljin, Andjelka; Savage, Melissa; Shaw, Olivia; Lunsky, Yona (November 2017). "Self-Injury in Autism Spectrum Disorder and Intellectual Disability: Exploring the Role of Reactivity to Pain and Sensory Input". Brain Sci. 7 (11): 140. doi:10.3390/brainsci7110140. PMC 5704147. PMID 29072583.
- "Applied Behavioral Strategies - Getting to Know ABA". Archived from the original on 2015-10-07. Retrieved 2015-12-16.
- "Invisible Abuse: ABA and the things only autistic people can see". 28 March 2019.
- "The Controversy Around ABA". Child Mind Institute.
- "The controversy over autism's most common therapy". 10 August 2016.
- Smith, M; Segal, J; Hutman, T. "Autism Spectrum Disorders".
{{cite journal}}: Cite journal requires|journal=(help) - "Neurofeedback And Autism: General Information And Systematic Review". February 6, 2022. Retrieved October 6, 2022.
- National Institute of Mental Health. "Medications for Autism". Psych Central. Archived from the original on 2015-12-13. Retrieved 2015-12-16.
- Pope, J; Volkmar, F (November 14, 2014). "Medicines for Autism".
{{cite journal}}: Cite journal requires|journal=(help) - "More Problems with Functioning Labels". Ollibean. 2013-09-26. Archived from the original on 2019-04-30. Retrieved 2017-12-29.
- Bottema-Beutel, Kristen; Kapp, Steven K.; Lester, Jessica Nina; Sasson, Noah J.; Hand, Brittany N. (1 March 2021). "Avoiding Ableist Language: Suggestions for Autism Researchers". Autism in Adulthood. 3 (1): 18–29. doi:10.1089/aut.2020.0014. ISSN 2573-9581. S2CID 221764244.
- "Identity-First Autistic". Identity-First Autistic. Archived from the original on 2017-12-30. Retrieved 2017-12-29.
- Williams, Kat (2019-04-04). "The Fallacy of Functioning Labels". National Center for Mental Health. Retrieved 2021-08-05.
Further reading
- Robison, John Elder (2007). Look Me in the Eye: My Life with Asperger's. Three Rivers Press. ISBN 9780307395986.