Rectal examination
Digital rectal examination (DRE; Latin: palpatio per anum, PPA) is an internal examination of the rectum, performed by a healthcare provider.
| Rectal examination | |
|---|---|
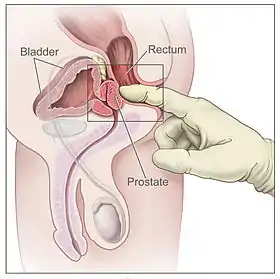 Digital rectal exam: side view of the male reproductive and urinary anatomy, including the prostate, rectum and bladder | |
| ICD-9-CM | 89.34 |
| MeSH | D051517 |
| MedlinePlus | 007069 |
Usage
This examination may be used
- for the diagnosis of prostatic disorders, benign prostatic hyperplasia and the four types of prostatitis. Chronic prostatitis/chronic pelvic pain syndrome, chronic bacterial prostatitis, acute (sudden) bacterial prostatitis, and asymptomatic inflammatory prostatitis. The DRE has a 50% specificity for benign prostatic hyperplasia.[1] Vigorous examination of the prostate in suspected acute prostatitis can lead to seeding of septic emboli and should never be done. Its utility as a screening method for prostate cancer however is not supported by the evidence;[2]
- for the evaluation of certain clinical symptoms: a male with change in urinary ability, impotence, or dysuria (blood in the urine), pain with bowel movements;[3]
- a DRE with a FOBT might have value for the anemic patient in the emergency room who has no other identifiable cause for anemia, is not actively bleeding, and you are concerned that Gastrointestinal malignancy may be the cause for their anemia;[4][5][6][7]
- a true active gastrointestinal bleed: vomiting blood, vomiting coffee-grind like material, defecating blood or black tarry stools that can not be easily attributed to facial trauma or oral surgery, eating beets or anything with red food dye or overuse of NSAIDS/over the counter pain medication. Doing a rectal exam to examine stool color may provide a clue as to the location of the bleed but is not a reliable indicator;[8][9][4][5][6]
- for the diagnosis of appendicitis or other examples of an acute abdomen (i.e. acute abdominal symptoms indicating a serious underlying disease). Although a Journal of Emergency Medicine paper concludes: "We found the DRE to have a limited role in the diagnosis of acute, undifferentiated abdominal pain and acute appendicitis.";[10][4]
- for the estimation of the muscle tone of the anal sphincter, which may be useful in case of fecal incontinence or neurologic diseases, including traumatic spinal cord injuries;
- traditionally, the digital rectal examination (DRE) was considered an essential part of the physical examination for all trauma patients. However, the sensitivity of the DRE for injuries of the spinal cord, pelvis, and bowel is poor, and false positive and negative results are common. Thus, routine performance is unnecessary and generally unhelpful. The examination is warranted in cases where urethral injury or penetrating rectal injury is suspected;[11][12]
- in females, for the limited gynecological palpations of internal organs when you are unable to access the vaginal vault or it is too painful (vaginal atrophy);
- for examination of the hardness and color of the feces (i.e. in cases of constipation, and fecal impaction);
- prior to a colonoscopy or proctoscopy;
- to evaluate hemorrhoids although internal hemorrhoids are often too soft to be felt, a visual inspection may be more useful;[13]
- in newborns to exclude imperforate anus;
- through the insertion of medical devices including thermometers or specialized balloons; to identify digestion problems, parasites, organ damage, anal bruising, and foreign objects in the rectal cavity;
Usage as a screening tool
In colorectal cancer screening of asymptomatic adults aged 50 to 75
- Even though 1 in 4 colorectal cancers (CRC) is located in the rectum, little evidence supports the effectiveness of using the DRE for rectal cancer detection[14][15] and it is not recommended in the colorectal cancer screening guidelines.[16] The DRE is inadequate as a screening tool for colorectal cancer because it examines less than 10% of the colorectal mucosa; sigmoidoscopy is preferred.
- Although the DRE is commonly used as a way to obtain a stool sample for a FOBT (fecal occult blood test) in an office based setting, this is an insufficient way of screening for colorectal cancer and is not recommended.[17][18][19] A single office-based FOBT (fecal occult blood test) performed following a digital rectal examination (DRE) is not an adequate screen due to low sensitivity for advanced tumor and colorectal cancer.[20] Screening for colon cancer this way does not meet HEDIS, Medicare or American Cancer Society standards.[21] The FOBT has never been validated for any purpose other than as a take home colon cancer screening test.[7] A paper published in the Journal of General Internal Medicine states, "While FOBT done appropriately (taken home and used according to the instructions) is an important screening option, in-office FOBT may be worse than no screening at all because it misses 95% of cases of advanced tumor, giving many patients a false sense of reassurance."[22]
In prostate cancer screening of asymptomatic men aged 55 to 69
- In men aged 55–69 who have been counseled on the known harms and potential benefits of prostate cancer screening, the U.S. Preventive Service Task Force (USPSTF) May 2018 statement states, "The use of digital rectal examination as a screening modality is not recommended because there is a lack of evidence on the benefits."[23] The American Academy of Family Physicians (AAFP) states, "Digital Rectal Exam does not improve detection of prostate cancer and should not be performed as a part of screening."[24] The American Urology Association (AUA) 2013 (reviewed and validity confirmed 2018) guideline panel states, "The literature supporting the efficacy of digital rectal exam (DRE) for screening with the goal of reducing prostate cancer mortality provide limited evidence to draw conclusions."[25] "The guideline panel could find no evidence to support the continued use of DRE as a first-line method of screening."[26] Although DRE has long been used to diagnose prostate cancer, no controlled studies have shown a reduction in the morbidity or mortality of prostate cancer when detected by DRE at any age.[26][27]
- A meta-analysis published in the Annals of Family Medicine concluded: "Given the considerable lack of evidence supporting its efficacy, we recommend against routine performance of DRE to screen for prostate cancer in the primary care setting."[2]
Procedure
The digital rectal examination is a relatively simple medical procedure. The patient undresses and is then placed in a position where the anus is accessible (lying on the side, squatting on the examination table, bent over it, or lying down with feet in stirrups). If the patient is lying on his/her side, the physician will usually have her/him bring one or both legs up to his/her chest. If the patient bends over the examination table or the back of a chair, the physician will have her/him place his/her elbows on the table and squat down slightly. If the patient uses the supine position, the physician will ask the patient to slide down to the end of the examination table until his/her buttocks are positioned just beyond the end and then place her/his feet in the stirrups. The physician spreads the buttocks apart and will usually examine the external area (anus and perineum) for any abnormalities such as hemorrhoids, lumps, or rashes. Then, as the patient relaxes and bears down (as if having a bowel movement), the physician slips a lubricated finger into the rectum through the anus and palpates the insides for a short time.[28]
Society and culture
Due to the taboos surrounding the anus and the potential for discomfort and embarrassment, the rectal exam is a common comedic device, including in episodes of Saturday Night Live,[29] Impractical Jokers, Futurama, Family Guy, South Park and the movie Fletch, with M. Emmet Walsh as the general practitioner and Chevy Chase as the patient being examined. Similar activities to the rectal exam are attributed to extraterrestrials in video games such as Saints Row IV, Gaia Online and Destroy All Humans!.[30] The practice of rectal exams without prior consent by medical students has been an area of concern.[31]
Veterinary medicine
In veterinary medicine rectal examination is useful in dogs for analysis of the prostate (as in men), pelvic urethra, sublumbar lymph nodes, and anal glands. In horses it is a vital component of the clinical examination for colic, to determine the presence or absence of bowel torsion, impaction, or displacement. When horses undergo a rectal examination there is a small risk of a rectal tear occurring, which can be a life-threatening event, rapidly leading to peritonitis and septic shock. It is also a common procedure in cattle, and is one method of diagnosing pregnancy in both the horse and the cow.
The procedure in dogs and cats is similar to humans. For the horse, the patient stands in a stock and may be sedated. The examiner puts on a long glove that extends to the shoulder. The examiner inserts the hand and arm into the rectum as far as necessary.
See also
- Body cavity search
- Colonoscopy
- GCC homosexuality test
References
- Goljan, Edward (2011). Rapid Review Pathology Third Edition. Mosby Elsevier. p. 429. ISBN 978-0-323-08438-3.
- Naji, Leen; Randhawa, Harkanwal; Sohani, Zahra; Dennis, Brittany; Lautenbach, Deanna; Kavanagh, Owen; Bawor, Monica; Banfield, Laura; Profetto, Jason (2018). "Digital Rectal Examination for Prostate Cancer Screening in Primary Care: A Systematic Review and Meta-Analysis". The Annals of Family Medicine. 16 (2): 149–154. doi:10.1370/afm.2205. PMC 5847354. PMID 29531107.
- "Pri-Med | Put That Finger Down! The End of the..." Pri-Med.
- "FOBT and DRE's in the ED (June 2018) » Emergency Medicine | Blog Archive | Boston University". www.bumc.bu.edu. Retrieved 2019-02-20.
- Gupta, Arjun; Tang, Zhouwen; Agrawal, Deepak (2018). "Eliminating In-Hospital Fecal Occult Blood Testing: Our Experience with Disinvestment". The American Journal of Medicine. 131 (7): 760–763. doi:10.1016/j.amjmed.2018.03.002. PMID 29601803. S2CID 5046971.
- Sharma, Virender K.; Komanduri, Sri; Nayyar, Sanjay; Headly, Anna; Modlinger, Paul; Metz, David C.; Verghese, Vino J.; Wanahita, Anna; Go, Mae F.; Howden, Colin W. (2001). "An audit of the utility of in-patient fecal occult blood testing". The American Journal of Gastroenterology. 96 (4): 1256–1260. doi:10.1111/j.1572-0241.2001.03709.x. PMID 11316179. S2CID 20602869.
- Monash, Bradley (2017-07-01). "Fecal occult blood testing in hospitalized patients with upper gastrointestinal bleeding". Journal of Hospital Medicine. 12 (7): 567–569. doi:10.12788/jhm.2773. PMID 28699947.
- "UpToDate". www.uptodate.com. Retrieved 2019-11-13.
- Jensen, D. M.; Machicado, G. A. (December 1988). "Diagnosis and treatment of severe hematochezia. The role of urgent colonoscopy after purge". Gastroenterology. 95 (6): 1569–1574. doi:10.1016/s0016-5085(88)80079-9. ISSN 0016-5085. PMID 3263294.
- Kessler, Chad; Bauer, Stephen J. (2012). "Utility of the Digital Rectal Examination in the Emergency Department: A Review". The Journal of Emergency Medicine. 43 (6): 1196–1204. doi:10.1016/j.jemermed.2012.06.015. PMID 22883714.
- "UpToDate". www.uptodate.com. Retrieved 2019-10-22.
- Shlamovitz, Gil Z.; Mower, William R.; Bergman, Jonathan; Crisp, Jonathan; DeVore, Heather K.; Hardy, David; Sargent, Martine; Shroff, Sunil D.; Snyder, Eric; Morgan, Marshall T. (July 2007). "Poor test characteristics for the digital rectal examination in trauma patients". Annals of Emergency Medicine. 50 (1): 25–33, 33.e1. doi:10.1016/j.annemergmed.2007.01.022. ISSN 1097-6760. PMID 17391807.
- "Hemorrhoids - Diagnosis and treatment - Mayo Clinic". Mayo Clinic.
- Ang, C. W.; Dawson, R.; Hall, C.; Farmer, M. (2008). "The diagnostic value of digital rectal examination in primary care for palpable rectal tumour". Colorectal Disease. 10 (8): 789–792. doi:10.1111/j.1463-1318.2007.01381.x. PMID 17868406. S2CID 639158.
- "UpToDate". www.uptodate.com. Retrieved 2019-02-18.
- "Final Recommendation Statement: Colorectal Cancer: Screening - US Preventive Services Task Force". www.uspreventiveservicestaskforce.org. Retrieved 2019-02-07.
- Wender, R. C. (2006). "Colorectal cancer screening: Don't just do it, do it right". American Family Physician. 73 (10): 1707–8. PMID 16734049.
- Ashraf, Imran; Paracha, Shafaq R.; Arif, Murtaza; Choudhary, Abhishek; Matteson, Michelle L.; Clark, Robert E.; Godfrey, Jonathan D.; Hammad, Hazem T.; Bechtold, Matthew L. (2012). "Digital Rectal Examination Versus Spontaneous Passage of Stool for Fecal Occult Blood Testing". Southern Medical Journal. 105 (7): 357–361. doi:10.1097/SMJ.0b013e31825bfdc5. PMID 22766663. S2CID 22573405.
- Nadel, Marion R.; Shapiro, Jean A.; Klabunde, Carrie N.; Seeff, Laura C.; Uhler, Robert; Smith, Robert A.; Ransohoff, David F. (2005). "A National Survey of Primary Care Physicians' Methods for Screening for Fecal Occult Blood". Annals of Internal Medicine. 142 (2): 86–94. doi:10.7326/0003-4819-142-2-200501180-00007. PMID 15657156. S2CID 24639260.
- Collins, Judith F.; Lieberman, David A.; Durbin, Theodore E.; Weiss, David G.; Veterans Affairs Cooperative Study #380 Group (2005). "Accuracy of Screening for Fecal Occult Blood on a Single Stool Sample Obtained by Digital Rectal Examination: A Comparison with Recommended Sampling Practice". Annals of Internal Medicine. 142 (2): 81–5. doi:10.7326/0003-4819-142-2-200501180-00006. PMID 15657155. S2CID 29833684.
- "Colorectal Cancer Screening Tests". www.cancer.org. Retrieved 2019-10-12.
- Nadel, Marion R.; Berkowitz, Zahava; Klabunde, Carrie N.; Smith, Robert A.; Coughlin, Steven S.; White, Mary C. (2010). "Fecal Occult Blood Testing Beliefs and Practices of U.S. Primary Care Physicians: Serious Deviations from Evidence-Based Recommendations". Journal of General Internal Medicine. 25 (8): 833–839. doi:10.1007/s11606-010-1328-7. PMC 2896587. PMID 20383599.
- Grossman, David C.; Curry, Susan J.; Owens, Douglas K.; Bibbins-Domingo, Kirsten; Caughey, Aaron B.; Davidson, Karina W.; Doubeni, Chyke A.; Ebell, Mark; Epling, John W.; Kemper, Alex R.; Krist, Alex H.; Kubik, Martha; Landefeld, C. Seth; Mangione, Carol M.; Silverstein, Michael; Simon, Melissa A.; Siu, Albert L.; Tseng, Chien-Wen; Tseng, C. W. (2018). "Screening for Prostate Cancer". JAMA. 319 (18): 1901–1913. doi:10.1001/jama.2018.3710. PMID 29801017.
- "Prostate Cancer - Clinical Preventive Service Recommendation". www.aafp.org. Retrieved 2019-02-18.
- "American Urological Association -". www.auanet.org. Retrieved 2019-02-20.
- Hoffman, Richard M (Jun 25, 2018). "Screening for prostate cancer". UpToDate.
- Epstein JI (2002). "Pathology of prostatic neoplasia". In Walsh PC (ed.). Campbell's Urology (8th ed.). Philadelphia: Saunders.
- "Digital Rectal Examination". Healthline. 26 June 2017. Retrieved 31 March 2018.
- New York Magazine - Vol. 28, No. 11. "Saturday Night Live at twenty"
- "Alien anal probe saw Saints Row IV refused classification in Australia". IGN Entertainment Inc. June 25, 2013. Retrieved July 19, 2014.
- Rees, Charlotte E.; Monrouxe, Lynn V. (2011). "Medical students learning intimate examinations without valid consent: A multicentre study". Medical Education. 45 (3): 261–272. doi:10.1111/j.1365-2923.2010.03911.x. PMID 21251051. S2CID 3372919.