Nevus
Nevus (plural nevi) is a nonspecific medical term for a visible, circumscribed, chronic lesion of the skin or mucosa.[1] The term originates from nævus, which is Latin for "birthmark"; however, a nevus can be either congenital (present at birth) or acquired. Common terms, including mole, birthmark, and beauty mark, are used to describe nevi, but these terms do not distinguish specific types of nevi from one another.
| Nevus | |
|---|---|
| Other names | nevi |
 | |
| A benign nevus | |
| Specialty | Dermatology |
Classification
The term nevus is applied to a number of conditions caused by neoplasias and hyperplasias of melanocytes,[2] as well as a number of pigmentation disorders, both hypermelanotic (containing increased melanin, the pigment responsible for skin color) and hypomelanotic (containing decreased melanin).[3] Suspicious skin moles which are multi-colored or pink may be a finding in skin cancer.[4]
Usually acquired
- Melanocytic nevus
- Atypical (dysplastic) nevus: This type of nevus must be diagnosed based on histological features. Clinically, atypical nevi are characterized by variable pigmentation and irregular borders.[5]
- Becker's nevus
- Blue nevus (rarely congenital): A classic blue nevus is usually smaller than 1 cm, flat, and blue-black in color.[6]
- Hori's nevus
- Nevus spilus (speckled lentiginous nevus): This lesion includes dark speckles within a tan-brown background.[7]
- Pigmented spindle cell nevus
- Spitz nevus
- Zosteriform lentiginous nevus
Usually congenital
- Congenital melanocytic nevus
- These nevi are often categorized based on size, however, the lesions usually grow in proportion to the body over time, so the category may change over an individual's life.[2] This categorization is important because large congenital melanocytic nevi are associated with an increased risk of melanoma, a serious type of skin cancer.[2]
- Nevus of Ito
- Nevus of Ota
 Conjunctival nevus of a 32-year-old male
Conjunctival nevus of a 32-year-old male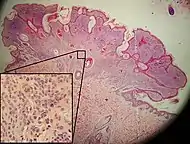 Micrograph of an intradermal melanocytic nevus
Micrograph of an intradermal melanocytic nevus.jpg.webp) Acquired melanocytic nevi
Acquired melanocytic nevi.jpg.webp) Atypical nevus
Atypical nevus Becker's nevus
Becker's nevus Blue nevus
Blue nevus
 Spitz nevus
Spitz nevus Congenital melanocytic nevus
Congenital melanocytic nevus Nevus of Ota
Nevus of Ota Compound nevus, left buttock
Compound nevus, left buttock
Acquired
Congenital
 Nevus anemicus
Nevus anemicus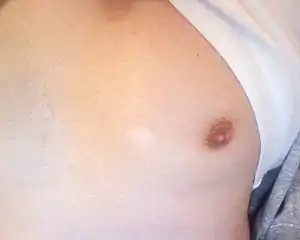 Nevus depigmentosus
Nevus depigmentosus
Additional types of nevi do not involve disorders of pigmentation or melanocytes. These additional nevi represent hamartomatous proliferations of the epithelium,[8] connective tissue,[9] and vascular malformations.[10]
Epidermal nevi
These nevi represent excess growth of specific cells types found in the skin, including those that make up oil and sweat glands.[8]
Connective tissue nevi
Connective tissue nevi represent abnormalities of collagen in the dermis, the deep layer of the skin.[9]
- Collagenoma
- Elastoma
Vascular nevi
These nevi represent excess growth of blood vessels, including capillaries.[11]
- Nevus simplex (nevus flammeus nuchae), also known as a stork bite or salmon patch.
 Nevus sebaceous
Nevus sebaceous.JPG.webp) Nevus flammeus nuchae
Nevus flammeus nuchae
Intramucosal nevi
An intramucosal nevus is a nevus within the mucosa as found in for example the mouth and genital areas. In the mouth, they are found most frequently on the hard palate. They are typically light brown and dome-shaped.[12] Intramucosal nevi account for 64% of all reported case of oral nevi.[13]
Diagnosis
Nevi are typically diagnosed clinically with the naked eye or using dermatoscopy. More advanced imaging tests are available for distinguishing melanocytic nevi from melanoma, including computerized dermoscopy and image analysis.[14] The management of nevi depends on the type of nevus and the degree of diagnostic uncertainty. Some nevi are known to be benign, and may simply be monitored over time. Others may warrant more thorough examination and biopsy for histopathological examination (looking at a sample of skin under a microscope to detect unique cellular features). For example, a clinician may want to determine whether a pigmented nevus is a type of melanocytic nevus, dysplastic nevus, or melanoma as some of these skin lesions pose a risk for malignancy. The ABCDE criteria (asymmetry, border irregularity, color variegation, diameter > 6 mm, and evolution) are often used to distinguish nevi from melanomas in adults, while modified criteria (amelanosis, bleeding or bumps, uniform color, small diameter or de novo, and evolution) can be used when evaluating suspicious lesions in children.[15] In addition to histopathological examination, some lesions may also warrant additional tests to aid in diagnosis, including special stains, immunohistochemistry, and electron microscopy.[16] Typically, the nevi that exist since childhood are harmless.
 A modern polarized dermatoscope
A modern polarized dermatoscope A dermatoscope
A dermatoscope
Differential diagnoses
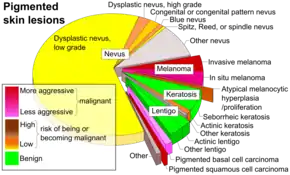
Hypermelanotic nevi must be differentiated from other types of pigmented skin lesions, including:[6][7]
- Lentigo simplex
- Solar lentigo
- Café au lait macule
- Ink-spot lentigo
- Mucosal melanotic macule
- Mongolian spot (dermal melanocytosis)
 Cafe au lait
Cafe au lait Mongolian spot
Mongolian spot
Management

The management of a nevus depends on the specific diagnosis, however, the options for treatment generally include the following modalities:
Destruction
- Chemical peels
- Cryotherapy
- Dermabrasion
- Electrodessication
- Laser ablation
Surgery
The decision to observe or treat a nevus may depend on a number of factors, including cosmetic concerns, irritative symptoms (e.g., pruritus), ulceration, infection, and concern for potential malignancy.[2]
Syndromes
The term nevus is included in the names of multiple dermatologic syndromes:
Etymology
A naevus may also be spelled nevus. The plural is nevi or naevi. The word is from nævus, Latin for "birthmark" and is correctly pronounced Nye-voos.
See also
References
- Happle, Rudolf (1995). "What is a nevus? A proposed definition of a common medical term". Dermatology. 191 (1): 1–5. doi:10.1159/000246468. PMID 8589475.
- "Chapter 122. Benign Neoplasias and Hyperplasias of Melanocytes". Fitzpatrick's Dermatology in General Medicine. The McGraw-Hill Companies, Inc. 2012. ISBN 978-0-07-166904-7.
- "Chapter 75. Hypomelanoses and Hypermelanoses". Fitzpatrick's Dermatology in General Medicine. The McGraw Hill Companies, Inc. 2012. ISBN 978-0-07-166904-7.
- Baran, Robert; Berker, David A. R. de; Holzberg, Mark; Thomas, Luc (2012). Baran and Dawber's Diseases of the Nails and their Management. John Wiley & Sons. p. PT113. ISBN 9781118286708.
- "Dysplastic (Atypical) Nevi". Melanocytic Lesions - Springer. 2014. doi:10.1007/978-1-4939-0891-2. ISBN 978-1-4939-0890-5.
- "Dermal melanocytosis". Melanocytic Lesions - Springer. 2014. doi:10.1007/978-1-4939-0891-2. ISBN 978-1-4939-0890-5.
- "Lentigo, Other Melanosis, and the Acquired Nevus". Melanocytic Lesions - Springer. 2014. doi:10.1007/978-1-4939-0891-2. ISBN 978-1-4939-0890-5.
- "Chapter 118. Benign Epithelial Tumors, Hamartomas, and Hyperplasias.". Fitzpatrick's Dermatology in General Medicine. The McGraw-Hill Companies, Inc. 2012. ISBN 978-0-07-166904-7.
- "Chapter 66. Dermal Hypertrophies and Benign Fibroblastic/Myofibroblastic Tumors.". Fitzpatrick's Dermatology in General Medicine. The McGraw-Hill Companies, Inc. 2012. ISBN 978-0-07-166904-7.
- "Chapter 172. Vascular Malformations.". Fitzpatrick's Dermatology in General Medicine. The McGraw Hill Companies, Inc. 2012. ISBN 978-0-07-166904-7.
- "Chapter 107. Neonatal, Pediatric, and Adolescent Dermatology". Fitzpatrick's Dermatology in General Medicine. The McGraw-Hill Companies, Inc. 2012. ISBN 978-0-07-166904-7.
- "Oral Nevi". MedScape. Retrieved 23 January 2018.
- Buchner, A.; Merrell, P. W.; Carpenter, W. M. (2004). "Relative frequency of solitary melanocytic lesions of the oral mucosa". Journal of Oral Pathology and Medicine. 33 (9): 550–557. doi:10.1111/j.1600-0714.2004.00238.x. ISSN 0904-2512. PMID 15357676.
- Rigel, Darrell S.; Russak, Julie; Friedman, Robert (2016-10-01). "The evolution of melanoma diagnosis: 25 years beyond the ABCDs". CA: A Cancer Journal for Clinicians. 60 (5): 301–316. doi:10.3322/caac.20074. ISSN 1542-4863. PMID 20671054.
- Scope, Alon; Marchetti, Michael A.; Marghoob, Ashfaq A.; Dusza, Stephen W.; Geller, Alan C.; Satagopan, Jaya M.; Weinstock, Martin A.; Berwick, Marianne; Halpern, Allan C. (2016). "The study of nevi in children: Principles learned and implications for melanoma diagnosis". Journal of the American Academy of Dermatology. 75 (4): 813–823. doi:10.1016/j.jaad.2016.03.027. PMC 5030195. PMID 27320410.
- "Ancillary Techniques in Diagnosing Melanocytic Lesions". Melanocytic Lesions - Springer. 2014. doi:10.1007/978-1-4939-0891-2. ISBN 978-1-4939-0890-5.