Lactose intolerance
Lactose intolerance is a common condition caused by a decreased ability to digest lactose, a sugar found in dairy products.[1] Those affected vary in the amount of lactose they can tolerate before symptoms develop.[1] Symptoms may include abdominal pain, bloating, diarrhea, flatulence, and nausea.[1] These symptoms typically start thirty minutes to two hours after eating or drinking milk-based food.[1] Their severity typically depends on the amount a person eats or drinks.[1] Lactose intolerance does not cause damage to the gastrointestinal tract.[2]
| Lactose intolerance | |
|---|---|
| Other names | Lactase deficiency, hypolactasia, alactasia, lactose challenged |
 | |
| Lactose is made up of two simple sugars | |
| Specialty | Gastroenterology |
| Symptoms | Abdominal pain, bloating, diarrhea, flatulence, nausea[1] |
| Complications | Does not cause damage to the GI tract[2] |
| Usual onset | 30–120 min after dairy products[1] |
| Causes | Decreased ability to digest lactose (genetic, small intestine injury)[1] |
| Diagnostic method | Symptoms resolve following eliminating lactose[1] |
| Differential diagnosis | Irritable bowel syndrome, celiac disease, inflammatory bowel disease, milk allergy[1] |
| Treatment | Decreasing lactose in the diet, lactase supplements, treat the underlying cause[1] |
| Frequency | ~65% of people (less common in Northern Europeans)[3] |
Lactose intolerance is due to the lack of the enzyme lactase in the small intestines to break lactose down into glucose and galactose.[3] There are four types: primary, secondary, developmental, and congenital.[1] Primary lactose intolerance occurs as the amount of lactase declines as people age.[1] Secondary lactose intolerance is due to injury to the small intestine. Such injury could be the result of infection, celiac disease, inflammatory bowel disease, or other diseases.[1][4] Developmental lactose intolerance may occur in premature babies and usually improves over a short period of time.[1] Congenital lactose intolerance is an extremely rare genetic disorder in which little or no lactase is made from birth.[1] The onset of primary lactose intolerance, the most common type, is typically in late childhood or early adulthood,[1] but prevalence increases with age.[5]
Diagnosis may be confirmed if symptoms resolve following eliminating lactose from the diet.[1] Other supporting tests include a hydrogen breath test and a stool acidity test.[1] Other conditions that may produce similar symptoms include irritable bowel syndrome, celiac disease, and inflammatory bowel disease.[1] Lactose intolerance is different from a milk allergy.[1] Management is typically by decreasing the amount of lactose in the diet, taking lactase supplements, or treating the underlying disease.[1][6] People are usually able to drink at least one cup of milk per sitting without developing significant symptoms, with greater amounts tolerated if drunk with a meal or throughout the day.[1][7]
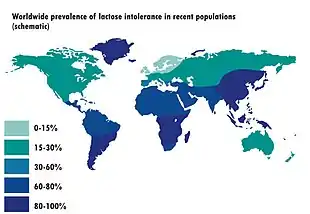
Most adults (around 65–70% of the world's population) are affected by lactose malabsorption.[5][8] Other mammals normally lose the ability to digest lactose after weaning and this was the ancestral state of all humans before the recent evolution of lactase persistence, which extends lactose tolerance into adulthood.[9] Lactase persistence evolved in several populations independently, probably as an adaptation to the domestication of dairy animals around 10,000 years ago.[10][11] Today the prevalence of lactose tolerance varies widely between regions and ethnic groups.[5] The ability to digest lactose is most common in people of European descent, and to a lesser extent in parts of the Middle East and Africa.[5][8] Traditional food cultures reflect local variations in tolerance[5] and historically many societies have adapted to low levels of tolerance by making dairy products that contain less lactose than fresh milk.[12] The medicalization of lactose intolerance as a disorder has been attributed to biases in research history, since most early studies were conducted amongst populations which are normally tolerant,[9] as well as the cultural and economic importance of milk in countries such as the United States.[13]
Terminology
Lactose intolerance primarily refers to a syndrome with one or more symptoms upon the consumption of food substances containing lactose sugar. Individuals may be lactose intolerant to varying degrees, depending on the severity of these symptoms.
Hypolactasia is the term specifically for the small intestine producing little or no lactase enzyme.[14] If a person with hypolactasia consumes lactose sugar, it results in lactose malabsorption.[2] The digestive system is unable to process the lactose sugar, and the unprocessed sugars in the gut produce the symptoms of lactose intolerance.
Lactose intolerance is not an allergy, because it is not an immune response, but rather a sensitivity to dairy caused by a deficiency of lactase enzyme. Milk allergy, occurring in about 2% of the population, is a separate condition, with distinct symptoms that occur when the presence of milk proteins trigger an immune reaction.[15]
Signs and symptoms
The principal manifestation of lactose intolerance is an adverse reaction to products containing lactose (primarily milk), including abdominal bloating and cramps, flatulence, diarrhea, nausea, borborygmi, and vomiting (particularly in adolescents). These appear one-half to two hours after consumption.[1] The severity of these signs and symptoms typically increases with the amount of lactose consumed; most lactose-intolerant people can tolerate a certain level of lactose in their diets without ill effects.[16][17]
Because lactose intolerance is not an allergy, it does not produce allergy symptoms (such as itching, hives, or anaphylaxis).
Causes
Lactose intolerance is a consequence of lactase deficiency, which may be genetic (primary hypolactasia and primary congenital alactasia) or environmentally induced (secondary or acquired hypolactasia). In either case, symptoms are caused by insufficient levels of lactase in the lining of the duodenum. Lactose, a disaccharide molecule found in milk and dairy products, cannot be directly absorbed through the wall of the small intestine into the bloodstream, so, in the absence of lactase, passes intact into the colon. Bacteria in the colon can metabolise lactose, and the resulting fermentation produces copious amounts of gas (a mixture of hydrogen, carbon dioxide, and methane) that causes the various abdominal symptoms. The unabsorbed sugars and fermentation products also raise the osmotic pressure of the colon, causing an increased flow of water into the bowels (diarrhea).[18][9]
Lactose intolerance in infants (congenital lactase deficiency) is caused by mutations in the LCT gene. The LCT gene provides the instructions for making lactase. Mutations are believed to interfere with the function of lactase, causing affected infants to have a severely impaired ability to digest lactose in breast milk or formula.[19] Lactose intolerance in adulthood is a result of gradually decreasing activity (expression) of the LCT gene after infancy, which occurs in most humans. The specific DNA sequence in the MCM6 gene helps control whether the LCT gene is turned on or off.[20] At least several thousand years ago, some humans developed a mutation in the MCM6 gene that keeps the LCT gene turned on even after breast feeding is stopped.[21] Populations that are lactose intolerant lack this mutation. The LCT and MCM6 genes are both located on the long arm (q) of chromosome 2 in region 21. The locus can be expressed as 2q21.[21] The lactase deficiency also could be linked to certain heritages and varies widely. A 2016 study of over 60,000 participants from 89 countries found regional prevalence of lactose malabsorption was "64% (54–74) in Asia (except Middle East), 47% (33–61) in eastern Europe, Russia, and former Soviet Republics, 38% (CI 18–57) in Latin America, 70% (57–83) in the Middle East, 66% (45–88) in northern Africa, 42% (13–71) in northern America, 45% (19–71) in Oceania, 63% (54–72) in sub-Saharan Africa, and 28% (19–37) in northern, southern and western Europe."[5] According to Johns Hopkins Medicine, lactose intolerance is more common in Asian Americans, African Americans, Mexican Americans, and Native Americans.[22] Analysis of the DNA of 94 ancient skeletons in Europe and Russia concluded that the mutation for lactose tolerance appeared about 4,300 years ago and spread throughout the European population.[23]
Some human populations have developed lactase persistence, in which lactase production continues into adulthood probably as a response to the benefits of being able to digest milk from farm animals. Some have argued that this links intolerance to natural selection favoring lactase-persistent individuals, but it is also consistent with a physiological response to decrease lactase production when it is not needed in cultures in which dairy products are not an available food source.[24] Although populations in Europe, India, Arabia, and Africa were first thought to have high rates of lactase persistence because of a single mutation, lactase persistence has been traced to a number of mutations that occurred independently.[11] Different alleles for lactase persistence have developed at least three times in East African populations, with persistence extending from 26% in Tanzania to 88% in the Beja pastoralist population in Sudan.[25]
The accumulation of epigenetic factors, primarily DNA methylation, in the extended LCT region, including the gene enhancer located in the MCM6 gene near C/T-13910 SNP, may also contribute to the onset of lactose intolerance in adults.[26][27] Age-dependent expression of LCT in mice intestinal epithelium has been DNA methylation in the gene enhancer.[27]
Lactose intolerance is classified according to its causes as:
Primary hypolactasia
Primary hypolactasia, or primary lactase deficiency, is genetic, only affects adults, and is caused by the absence of a lactase persistence allele. In individuals without the lactase persistence allele, less lactase is produced by the body over time, leading to hypolactasia in adulthood.[2][28] The frequency of lactase persistence, which allows lactose tolerance, varies enormously worldwide, with the highest prevalence in Northwestern Europe, declines across southern Europe and the Middle East and is low in Asia and most of Africa, although it is common in pastoralist populations from Africa.[9]
Secondary hypolactasia
Secondary hypolactasia or secondary lactase deficiency, also called acquired hypolactasia or acquired lactase deficiency, is caused by an injury to the small intestine. This form of lactose intolerance can occur in both infants and lactase persistent adults and is generally reversible.[29] It may be caused by acute gastroenteritis, coeliac disease, Crohn's disease, ulcerative colitis,[30] chemotherapy, intestinal parasites (such as giardia), or other environmental causes.[2][31][32][33]
Primary congenital alactasia
Primary congenital alactasia, also called congenital lactase deficiency, is an extremely rare, autosomal recessive enzyme defect that prevents lactase expression from birth.[2] People with congenital lactase deficiency cannot digest lactose from birth, so cannot digest breast milk. This genetic defect is characterized by a complete lack of lactase (alactasia). About 40 cases have been reported worldwide, mainly limited to Finland. Before the 20th century, babies born with congenital lactase deficiency often did not survive,[2] but death rates decreased with soybean-derived infant formulas and manufactured lactose-free dairy products.[34]
Diagnosis
In order to assess lactose intolerance, intestinal function is challenged by ingesting more dairy products than can be readily digested. Clinical symptoms typically appear within 30 minutes, but may take up to two hours, depending on other foods and activities.[35] Substantial variability in response (symptoms of nausea, cramping, bloating, diarrhea, and flatulence) is to be expected, as the extent and severity of lactose intolerance varies among individuals.
The next step is to determine whether it is due to primary lactase deficiency or an underlying disease that causes secondary lactase deficiency.[2] Physicians should investigate the presence of undiagnosed coeliac disease, Crohn disease, or other enteropathies when secondary lactase deficiency is suspected and infectious gastroenteritis has been ruled out.[2]
Lactose intolerance is distinct from milk allergy, an immune response to cow's milk proteins. They may be distinguished in diagnosis by giving lactose-free milk, producing no symptoms in the case of lactose intolerance, but the same reaction as to normal milk in the presence of a milk allergy. A person can have both conditions. If positive confirmation is necessary, four tests are available.[36]
Hydrogen breath test
In a hydrogen breath test, the most accurate lactose intolerance test, after an overnight fast, 25 grams of lactose (in a solution with water) are swallowed. If the lactose cannot be digested, enteric bacteria metabolize it and produce hydrogen, which, along with methane, if produced, can be detected on the patient's breath by a clinical gas chromatograph or compact solid-state detector. The test takes about 2.5 hours to complete. If the hydrogen levels in the patient's breath are high, they may have lactose intolerance. This test is not usually done on babies and very young children, because it can cause severe diarrhea.[37]
Lactose tolerance test
In conjunction, measuring blood glucose level every 10 to 15 minutes after ingestion will show a "flat curve" in individuals with lactose malabsorption, while the lactase persistent will have a significant "top", with a typical elevation of 50% to 100%, within one to two hours. However, due to the need for frequent blood sampling, this approach has been largely replaced by breath testing.[38]
After an overnight fast, blood is drawn and then 50 grams of lactose (in aqueous solution) are swallowed. Blood is then drawn again at the 30-minute, 1-hour, 2-hour, and 3-hour marks. If the lactose cannot be digested, blood glucose levels will rise by less than 20 mg/dl.[39]
Stool acidity test
This test can be used to diagnose lactose intolerance in infants, for whom other forms of testing are risky or impractical.[40] The infant is given lactose to drink. If the individual is tolerant, the lactose is digested and absorbed in the small intestine; otherwise, it is not digested and absorbed, and it reaches the colon. The bacteria in the colon, mixed with the lactose, cause acidity in stools. Stools passed after the ingestion of the lactose are tested for level of acidity. If the stools are acidic, the infant is intolerant to lactose.[41] Stool pH in lactose intolerance is less than 5.5.
Intestinal biopsy
An intestinal biopsy must confirm lactase deficiency following discovery of elevated hydrogen in the hydrogen breath test.[42] Modern techniques have enabled a bedside test, identifying presence of lactase enzyme on upper gastrointestinal endoscopy instruments.[43] However, for research applications such as mRNA measurements, a specialist laboratory is required.
Stool sugar chromatography
Chromatography can be used to separate and identify undigested sugars present in faeces. Although lactose may be detected in the faeces of people with lactose intolerance, this test is not considered reliable enough to conclusively diagnose or exclude lactose intolerance.
Genetic diagnostic
Genetic tests may be useful in assessing whether a person has primary lactose intolerance. Lactase activity persistence in adults is associated with two polymorphisms: C/T 13910 and G/A 22018 located in the MCM6 gene.[28] These polymorphisms may be detected by molecular biology techniques at the DNA extracted from blood or saliva samples; genetic kits specific for this diagnosis are available. The procedure consists of extracting and amplifying DNA from the sample, following with a hybridation protocol in a strip. Colored bands are obtained as result, and depending on the different combinations, it would be possible to determine whether the patient is lactose intolerant. This test allows a noninvasive definitive diagnostic.
Frequency
Lactose intolerance is most common in people of East Asian descent, with 70 to 100 percent of people affected in these communities. Lactose intolerance is also very common in people of West African, Arab, Jewish, Greek, and Italian descent, while only about 5 percent of people of Northern European descent are lactose intolerant.[19]
Management
When lactose intolerance is due to secondary lactase deficiency, treatment of the underlying disease may allow lactase activity to return to normal levels.[6] In people with celiac disease, lactose intolerance normally reverts or improves several months after starting a gluten-free diet, but temporary dietary restriction of lactose may be needed.[4][44]
People with primary lactase deficiency cannot modify their body's ability to produce lactase.[1] In societies where lactose intolerance is the norm, it is not considered a condition that requires treatment. However, where dairy is a larger component of the normal diet, a number of efforts may be useful. There are four general principles in dealing with lactose intolerance: avoidance of dietary lactose, substitution to maintain nutrient intake, regulation of calcium intake, and use of enzyme substitute.[42] Regular consumption of dairy food by lactase deficient individuals may also reduce symptoms of intolerance by promoting colonic bacteria adaptation.[45]
Dietary avoidance
The primary way of managing the symptoms of lactose intolerance is to limit the intake of lactose to a level that can be tolerated.[46] Lactase deficient individuals vary in the amount of lactose they can tolerate,[1] and some report that their tolerance varies over time, depending on health status and pregnancy.[47][48] However, as a rule of thumb, people with primary lactase deficiency and no small intestine injury are usually able to consume at least 12 grams of lactose per sitting without symptoms, or with only mild symptoms, with greater amounts tolerated if consumed with a meal or throughout the day.[1][48][45]
| Dairy product | Serving size | Lactose content | Percentage |
|---|---|---|---|
| Milk, regular | 250 ml/g | 12 g | 4.80% |
| Milk, reduced fat | 250 ml/g | 13 g | 5.20% |
| Yogurt, plain, regular | 200 g | 9 g | 4.50% |
| Yogurt, plain, low-fat | 200 g | 12 g | 6.00% |
| Cheddar cheese | 30 g | 0.02 g | 0.07% |
| Cottage cheese | 30 g | 0.1 g | 0.33% |
| Butter | 5 g | 0.03 g | 0.6% |
| Ice cream | 50 g | 3 g | 6.00% |
Lactose is found primarily in dairy products, which vary in the amount of lactose they contain:
- Milk – unprocessed cow's milk is about 4.7% lactose; goat's milk 4.7%;[50] sheep's milk 4.7%;[51] buffalo milk 4.86%;[52] and yak milk 4.93%.[53]
- Sour cream and buttermilk – if made in the traditional way, this may be tolerable, but most modern brands add milk solids.[54]
- Butter – the process of making butter largely removes lactose, but it is still present in small quantities; clarified butter contains a negligible amount of lactose.[55]
- Yogurt – lactobacilli used in the production of yogurt metabolize lactose to varying degrees, depending on the type of yogurt.[56] Some bacteria found in yogurt also produce their own lactase, which facilitates digestion in the intestines of lactose intolerant individuals.[45]
- Cheese – fermentation also reduces the lactose content of cheeses and aging reduces it further; traditionally made hard cheeses might contain just 10% of the lactose found in an equivalent volume of milk.[57] However, manufactured cheeses may be produced using processes that do not have the same lactose-reducing properties.[58]
There is no standardized method for measuring the lactose content of food.[59] The stated dairy content of a product also varies according to manufacturing processes and labelling practices, and commercial terminology varies between languages and regions.[42] As a result, absolute figures for the amount of lactose consumed (by weight) may not be very reliable. Kosher products labeled pareve or fleishig are free of milk. However, if a "D" (for "dairy") is present next to the circled "K", "U", or other hechsher, the food product likely contains milk solids,[60] although it may also simply indicate the product was produced on equipment shared with other products containing milk derivatives.
Lactose is also a commercial food additive used for its texture, flavor, and adhesive qualities. It is found in additives labelled as casein, caseinate, whey, lactoserum, milk solids, modified milk ingredients, etc. As such lactose is found in foods such as processed meats (sausages/hot dogs, sliced meats, pâtés),[60] gravy stock powder, margarines,[61] sliced breads,[62][63] breakfast cereals, potato chips,[64] processed foods, medications, prepared meals, meal replacements (powders and bars), protein supplements (powders and bars), and even beers in the milk stout style. Some barbecue sauces and liquid cheeses used in fast-food restaurants may also contain lactose. Lactose is often used as the primary filler (main ingredient) in most prescription and non-prescription solid pill form medications, though product labeling seldom mentions the presence of 'lactose' or 'milk', and neither do product monograms provided to pharmacists, and most pharmacists are unaware of the very wide scale yet common use of lactose in such medications until they contact the supplier or manufacturer for verification.
Milk substitutes
Plant-based milks and derivatives such as soy milk, rice milk, almond milk, coconut milk, hazelnut milk, oat milk, hemp milk, macadamia nut milk, and peanut milk are inherently lactose-free. Low-lactose and lactose-free versions of foods are often available to replace dairy-based foods for those with lactose intolerance.[65]
Lactase supplements
When lactose avoidance is not possible, or on occasions when a person chooses to consume such items, then enzymatic lactase supplements may be used.[66][67]
Lactase enzymes similar to those produced in the small intestines of humans are produced industrially by fungi of the genus Aspergillus. The enzyme, β-galactosidase, is available in tablet form in a variety of doses, in many countries without a prescription. It functions well only in high-acid environments, such as that found in the human gut due to the addition of gastric juices from the stomach. Unfortunately, too much acid can denature it,[68] so it should not be taken on an empty stomach. Also, the enzyme is ineffective if it does not reach the small intestine by the time the problematic food does. Lactose-sensitive individuals can experiment with both timing and dosage to fit their particular needs.
While essentially the same process as normal intestinal lactose digestion, direct treatment of milk employs a different variety of industrially produced lactase. This enzyme, produced by yeast from the genus Kluyveromyces, takes much longer to act, must be thoroughly mixed throughout the product, and is destroyed by even mildly acidic environments. Its main use is in producing the lactose-free or lactose-reduced dairy products sold in supermarkets.[69]
Rehabituation to dairy products
Regular consumption of dairy foods containing lactose can promote a colonic bacteria adaptation, enhancing a favorable microbiome, which allows people with primary lactase deficiency to diminish their intolerance and to consume more dairy foods.[45][48][70] The way to induce tolerance is based on progressive exposure, consuming smaller amounts frequently, distributed throughout the day.[71] Lactose intolerance can also be managed by ingesting live yogurt cultures containing lactobacilli that are able to digest the lactose in other dairy products.[72]
Epidemiology

Overall, about 65% of people experience some form of lactose intolerance as they age past infancy, but there are significant differences between populations and regions; rates are as low as 5% among northern Europeans and as high as over 90% of adults in some communities of Asia.[74]
Some populations, from an evolutionary perspective, have a better genetic makeup for tolerating lactose than others. In northern European countries, early adoption of dairy farming conferred a selective evolutionary advantage to individuals that could better tolerate lactose. This led to higher frequencies of these countries' people having a tolerance to lactose. Conversely, regions of the south, such as Africa, did not adopt dairy farming as early historically and therefore tolerance from milk consumption did not develop the same way as in northern European countries.[45] Lactose intolerance is common among people of Jewish descent, as well as from West Africa, the Arab countries, Greece, and Italy.[74] Different populations will present certain gene constructs depending on the evolutionary and cultural pre-settings of the geographical region.[45]
History
Greater lactose tolerance has come about in two ways.[75] Some populations have developed genetic changes that resulted in ongoing production of lactase.[75] Other populations developed cooking methods like milk fermentation.[75]
Lactase persistence is the phenotype associated with various autosomal dominant alleles prolonging the activity of lactase beyond infancy; conversely, lactase nonpersistence is the phenotype associated with primary lactase deficiency. Among mammals, lactase persistence is unique to humans—it evolved relatively recently (in the last 10,000 years) among some populations, and the majority of people worldwide remain lactase nonpersistent.[9] Around 8,000 years ago in modern-day Turkey, humans became reliant on newly domesticated animals such as cows, sheep, and goats. This newfound reliance resulted in higher frequency near the gene responsible for producing the lactase enzyme.[76] Populations that domesticated animals that could be milked continued to be lactase persistent in areas such as North and North western Europe, Scandinavia, the modern Middle East and Northwestern India. Populations that raised animals not used for milk made up the rest of the world's populations. These populations tend to have 90-100 percent of a lactose intolerant rate.[77] For this reason, lactase persistence is of some interest to the fields of anthropology, human genetics, and archaeology, which typically use the genetically derived persistence/non-persistence terminology.[78]
The rise of dairy and producing dairy related products from cow milk alone, varies across different regions of the world, aside from genetic predisposition.[45] The process of turning milk into cheese dates back earlier than 5200 BC.[79]
DNA analysis in February 2012 revealed that Ötzi was lactose intolerant, supporting the theory that lactose intolerance was still common at that time, despite the increasing spread of agriculture and dairying.[80]
Genetic analysis shows lactase persistence has developed several times in different places independently in an example of convergent evolution.[25]
History of research
It is not until relatively recently that medicine recognised the worldwide prevalence of lactose intolerance and its genetic causes. Its symptoms were described as early as Hippocrates (460–370 BC),[81] but until the 1960s, the prevailing assumption was that tolerance was the norm. Intolerance was explained as the result of a milk allergy, intestinal pathogens, or as being psychosomatic – it being recognised that some cultures did not practice dairying, and people from those cultures often reacted badly to consuming milk.[82][83] Two reasons have been given for this misconception. One was that most European-descended populations have a low incidence of lactose intolerance[84] and an extensive cultural history of dairying. Therefore, tolerance actually was the norm in most of the societies investigated by early medical researchers. Another reason is that lactose intolerance tends to be under-reported: lactose intolerant individuals can tolerate at least some lactose before they show symptoms, and their symptoms differ in severity. Most people are able to digest a small quantity of milk, for example in tea or coffee, without developing any adverse effects.[16] Fermented dairy products, such as cheese, also contain significantly less lactose than plain milk. Therefore, in societies where tolerance is the norm, many lactose intolerant people who consume only small amounts of dairy, or have only mild symptoms, may be unaware that they cannot digest lactose.
Eventually, in the 1960s, it was recognised that lactose intolerance was correlated with race in the United States.[85][86][87] Subsequent research revealed that lactose intolerance was more common globally than tolerance,[88][89][90][91][92] and that the variation was due to genetic differences, not an adaptation to cultural practices.[83][93]
Other animals
Most mammals normally cease to produce lactase and become lactose intolerant after weaning.[9] The downregulation of lactase expression in mice could be attributed to the accumulation of DNA methylation in the Lct gene and the adjacent Mcm6 gene.[94]
See also
- Food intolerance
- Gastroenterology
- Glucose-galactose malabsorption
- Gluten intolerance
- Lactase persistence
- Soy cheese
- Soy milk and plant milk
- Sucrose intolerance
References
- "Lactose Intolerance". NIDDK. June 2014. Archived from the original on 25 October 2016. Retrieved 25 October 2016.
- Heyman MB (September 2006). "Lactose intolerance in infants, children, and adolescents". Pediatrics. 118 (3): 1279–86. doi:10.1542/peds.2006-1721. PMID 16951027. S2CID 2996092.
- Malik, TF; Panuganti, KK (January 2020). "Lactose Intolerance". (StatPearls [Internet]). StatPearls. PMID 30335318. NBK532285.
- Berni Canani R, Pezzella V, Amoroso A, Cozzolino T, Di Scala C, Passariello A (March 2016). "Diagnosing and Treating Intolerance to Carbohydrates in Children". Nutrients. 8 (3): 157. doi:10.3390/nu8030157. PMC 4808885. PMID 26978392.
- Storhaug CL, Fosse SK, Fadnes LT (October 2017). "Country, regional, and global estimates for lactose malabsorption in adults: a systematic review and meta-analysis". The Lancet. Gastroenterology & Hepatology. 2 (10): 738–746. doi:10.1016/S2468-1253(17)30154-1. PMID 28690131.
- Vandenplas Y (2015). "Lactose intolerance". Asia Pacific Journal of Clinical Nutrition. 24 (Suppl 1): S9–13. doi:10.6133/apjcn.2015.24.s1.02. PMID 26715083.
- Suchy FJ, Brannon PM, Carpenter TO, Fernandez JR, Gilsanz V, Gould JB, Hall K, Hui SL, Lupton J, Mennella J, Miller NJ, Osganian SK, Sellmeyer DE, Wolf MA (February 2010). "NIH consensus development conference statement: Lactose intolerance and health". NIH Consensus and State-Of-The-Science Statements (Consensus Development Conference, NIH. Review). 27 (2): 1–27. PMID 20186234. Archived from the original on 2016-12-18.
- Bayless TM, Brown E, Paige DM (May 2017). "Lactase Non-persistence and Lactose Intolerance". Current Gastroenterology Reports. 19 (5): 23. doi:10.1007/s11894-017-0558-9. PMID 28421381. S2CID 2941077.
- Swallow DM (2003). "Genetics of lactase persistence and lactose intolerance". Annual Review of Genetics. 37: 197–219. doi:10.1146/annurev.genet.37.110801.143820. PMID 14616060.
- Ségurel L, Bon C (August 2017). "On the Evolution of Lactase Persistence in Humans". Annual Review of Genomics and Human Genetics. 18 (1): 297–319. doi:10.1146/annurev-genom-091416-035340. PMID 28426286.
- Ingram CJ, Mulcare CA, Itan Y, Thomas MG, Swallow DM (January 2009). "Lactose digestion and the evolutionary genetics of lactase persistence". Human Genetics. 124 (6): 579–91. doi:10.1007/s00439-008-0593-6. PMID 19034520. S2CID 3329285.
- Silanikove, Nissim; Leitner, Gabriel; Merin, Uzi (31 August 2015). "The Interrelationships between Lactose Intolerance and the Modern Dairy Industry: Global Perspectives in Evolutional and Historical Backgrounds". Nutrients. 7 (9): 7312–7331. doi:10.3390/nu7095340. PMC 4586535. PMID 26404364.
- Wiley, Andrea S. (2004). ""Drink Milk for Fitness": The Cultural Politics of Human Biological Variation and Milk Consumption in the United States". American Anthropologist. 106 (3): 506–517. doi:10.1525/aa.2004.106.3.506. JSTOR 3567615.
- Lember M (2012). "Hypolactasia: a common enzymes deficiency leading to lactose malabsorption and intolerance". Polskie Archiwum Medycyny Wewnetrznej. 122 Suppl 1: 60–4. doi:10.20452/pamw.1519. PMID 23222197.
- Bahna SL (December 2002). "Cow's milk allergy versus cow milk intolerance". Annals of Allergy, Asthma & Immunology (Review. Comparative Study.). 89 (6 Suppl 1): 56–60. doi:10.1016/S1081-1206(10)62124-2. PMID 12487206.
- Savaiano DA, Levitt MD (February 1987). "Milk intolerance and microbe-containing dairy foods". Journal of Dairy Science. 70 (2): 397–406. doi:10.3168/jds.S0022-0302(87)80023-1. PMID 3553256.
- Mądry E, Krasińska B, Woźniewicz MG, Drzymała-Czyż SA, Bobkowski W, Torlińska T, Walkowiak JA (2011). "Tolerance of different dairy products in subjects with symptomatic lactose malabsorption due to adult type hypolactasia". Gastroenterology Review. 5: 310–315. doi:10.5114/pg.2011.25381.
- Lactose intolerance~overview at eMedicine
- "Lactose intolerance: MedlinePlus Genetics". medlineplus.gov. Retrieved 2022-03-22.
- Genetics Home Reference. "MCM6". Genetics Home Reference. Archived from the original on 2013-10-04.
- Benjamin Phelan (23 October 2012). "Evolution of lactose tolerance: Why do humans keep drinking milk?". Slate Magazine. Archived from the original on 31 August 2013.
- "Lactose Intolerance". Johns Hopkins Health Library. Archived from the original on 2014-02-26. Retrieved 2014-02-18.
- Gibbons, Ann (2 April 2015). "How Europeans evolved white skin". Science. doi:10.1126/science.aab2435.
- Beja-Pereira A, Luikart G, England PR, Bradley DG, Jann OC, Bertorelle G, Chamberlain AT, Nunes TP, Metodiev S, Ferrand N, Erhardt G (December 2003). "Gene-culture coevolution between cattle milk protein genes and human lactase genes". Nature Genetics. 35 (4): 311–3. doi:10.1038/ng1263. PMID 14634648. S2CID 20415396.
- Tishkoff SA, Reed FA, Ranciaro A, Voight BF, Babbitt CC, Silverman JS, Powell K, Mortensen HM, Hirbo JB, Osman M, Ibrahim M, Omar SA, Lema G, Nyambo TB, Ghori J, Bumpstead S, Pritchard JK, Wray GA, Deloukas P (January 2007). "Convergent adaptation of human lactase persistence in Africa and Europe". Nature Genetics. 39 (1): 31–40. doi:10.1038/ng1946. PMC 2672153. PMID 17159977.
- Labrie V, Buske OJ, Oh E, Jeremian R, Ptak C, Gasiūnas G, et al. (June 2016). "Lactase nonpersistence is directed by DNA-variation-dependent epigenetic aging". Nature Structural & Molecular Biology. 23 (6): 566–73. doi:10.1038/nsmb.3227. PMC 4899171. PMID 27159559.
- Oh, Edward; Jeremian, Richie; Oh, Gabriel; Groot, Daniel; Susic, Miki; Lee, KwangHo; Foy, Kelly; Laird, Peter W.; Petronis, Arturas; Labrie, Viviane (2017-01-31). "Transcriptional heterogeneity in the lactase gene within cell-type is linked to the epigenome". Scientific Reports. 7 (1): 41843. Bibcode:2017NatSR...741843O. doi:10.1038/srep41843. PMC 5282553. PMID 28139744.
- Enattah NS, Sahi T, Savilahti E, Terwilliger JD, Peltonen L, Järvelä I (February 2002). "Identification of a variant associated with adult-type hypolactasia". Nature Genetics. 30 (2): 233–7. doi:10.1038/ng826. PMID 11788828. S2CID 21430931.
- "Lactose intolerance". The Dairy Council UK. Archived from the original on 9 March 2016.
- Secondary lactase deficiency causes Archived 2016-07-31 at the Wayback Machine
- Lawson M, Bentley D, Lifschitz C (2002). Pediatric gastroenterology and clinical nutrition. London: Remedica. p. 109. ISBN 978-1-901346-43-5. Archived from the original on 2016-12-19.
- Pediatric Lactose Intolerance at eMedicine
- Swagerty DL, Walling AD, Klein RM (May 2002). "Lactose intolerance". American Family Physician. 65 (9): 1845–50. PMID 12018807.
- Sinden AA, Sutphen JL (December 1991). "Dietary treatment of lactose intolerance in infants and children". Journal of the American Dietetic Association. 91 (12): 1567–71. doi:10.1016/S0002-8223(21)01435-8. PMID 1960350. S2CID 32296893.
- R. Bowen (December 28, 2006). "Lactose Intolerance (Lactase Non-Persistence)". Pathophysiology of the Digestive System. Colorado State University. Archived from the original on June 23, 2010.
- Olivier CE, Lorena SL, Pavan CR, dos Santos RA, dos Santos Lima RP, Pinto DG, da Silva MD, de Lima Zollner R (2012). "Is it just lactose intolerance?". Allergy and Asthma Proceedings. 33 (5): 432–6. doi:10.2500/aap.2012.33.3584. PMID 23026186.
- "Lactose Intolerance Tests and Results". WebMD. Archived from the original on 2014-02-02.
- "Hydrogen Breath Test and Lactose Intolerance". WebMD. Archived from the original on 2017-08-16. Retrieved 2017-08-19.
- "Lactose tolerance tests". 3 May 2011. Archived from the original on 27 May 2016.
- National Digestive Diseases Information Clearinghouse (March 2006). "Lactose Intolerance — How is lactose intolerance diagnosed?". National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health. Archived from the original on 2011-11-25. Retrieved 2004-11-19.
- "Stool Acidity Test". Jay W. Marks, M.D. Archived from the original on 2011-05-16. Retrieved 2011-05-20.
- Hargrove JL, Berdanier CD (1993). Nutrition and gene expression. Boca Raton: CRC Press. ISBN 978-0-8493-6961-2.
- Kuokkanen M, Myllyniemi M, Vauhkonen M, Helske T, Kääriäinen I, Karesvuori S, Linnala A, Härkönen M, Järvelä I, Sipponen P (July 2006). "A biopsy-based quick test in the diagnosis of duodenal hypolactasia in upper gastrointestinal endoscopy". Endoscopy. 38 (7): 708–12. doi:10.1055/s-2006-925354. PMID 16761211.
- Levy J, Bernstein L, Silber N (December 2014). "Celiac disease: an immune dysregulation syndrome". Current Problems in Pediatric and Adolescent Health Care (Review). 44 (11): 324–7. doi:10.1016/j.cppeds.2014.10.002. PMID 25499458.
Initially, reduced levels of lactase and sucrase activities might necessitate further dietary restrictions until the villi have healed and those sugars are better tolerated.
- Silanikove N, Leitner G, Merin U (August 2015). "The Interrelationships between Lactose Intolerance and the Modern Dairy Industry: Global Perspectives in Evolutional and Historical Backgrounds". Nutrients (Review). 7 (9): 7312–31. doi:10.3390/nu7095340. PMC 4586535. PMID 26404364.
- "Lactose intolerance - Treatment". NHS UK. Archived from the original on 18 July 2017. Retrieved 11 August 2017.
- Lactose Intolerance at eMedicine Roy, Barakat, Nwakakwa, Shojamanesh, Khurana, July 5, 2006
- Szilagyi A (August 2015). "Adaptation to Lactose in Lactase Non Persistent People: Effects on Intolerance and the Relationship between Dairy Food Consumption and Evalution [sic] of Diseases". Nutrients (Review). 7 (8): 6751–79. doi:10.3390/nu7085309. PMC 4555148. PMID 26287234.
- "Diet for Lactose Intolerance". Archived from the original on 2005-12-24.
- Eddleman, Harold (25 December 2003). "Composition of Human, Cow, and Goat Milks". GoatWorld.com. Archived from the original on 28 September 2007.
- "Amount of Lactose in Milk Products". food-intolerance-network.com. Food Intolerance Network. 21 November 2013. Archived from the original on 7 September 2017. Retrieved 7 September 2017.
- Peeva (2001). "Composition of buffalo milk. Sources of specific effects on the separate components". Bulgarian Journal of Agricultural Science. 7: 329–35. Archived from the original on 2007-08-29.
- Jiang XP, Liu GQ, Wang C, Mao YJ, Xiong YZ (2004). "Milk trait heritability and correlation with heterozygosity in yak" (PDF). Journal of Applied Genetics. 45 (2): 215–24. PMID 15131352. Archived (PDF) from the original on 2008-03-07.
- Reger JV, Combs WB, Coulter ST, Koch RB (February 1, 1951). "A Comparison of Dry Sweet Cream Buttermilk and Non-Fat Dry Milk Solids in Breadmaking". Journal of Dairy Science. 34 (2): 136–44. doi:10.3168/jds.S0022-0302(51)91682-7.
- "Is Butter a Dairy Product, and Does It Contain Lactose?". Healthline. 30 July 2019. Retrieved 2020-06-11.
- Perkins, Sharon (19 November 2018). "Can a Lactose Intolerant Eat Some Yogurt & Aged Cheese?". SFGATE. Archived from the original on 2015-04-28.
- "Dairy Good: Home". Archived from the original on 2013-07-30.
- Muthukummarappan, K; Biswas, A.C.; Metzger, L.E.; Kapoor, R (2007). "Effect of Natural Cheese Characteristics on Process Cheese Properties". Journal of Dairy Science. Plum X Metrics. 90 (4): 1625–1634. doi:10.3168/jds.2006-746. PMID 17369202. Retrieved April 19, 2022.
- "Goat Dairy Foods". Archived from the original on 2007-11-11. Retrieved 2007-10-11.
- "General guidelines for milk allergy". Oregon Health & Science University. Archived from the original on 2012-12-12.
- "Margarine Regulations". Archived from the original on 2007-10-11.
- "Enriched White Bread in Canada". The Canadian Celiac Association. Archived from the original on 2007-12-03. Retrieved 2007-10-11.
- Riggs LK, Beaty A, Johnson AH (December 1946). "Influence of Nonfat Dry Milk Solids on the Nutritive Value of Bread". Journal of Dairy Science. 29 (12): 821–9. doi:10.3168/jds.S0022-0302(46)92546-5.
- "Bartek, food additive company" (PDF). Archived from the original (PDF) on 2008-12-17. Retrieved 2007-10-11.
- Trotta T, Posa F, Mori G, Porro C (2017). "Dairy Products and Their Role in Human Health". Advances in Dairy Products. pp. 248–61. doi:10.1002/9781118906460.ch2f. ISBN 978-1-118-90646-0.
- Montalto M, Curigliano V, Santoro L, Vastola M, Cammarota G, Manna R, Gasbarrini A, Gasbarrini G (January 2006). "Management and treatment of lactose malabsorption". World Journal of Gastroenterology. 12 (2): 187–91. doi:10.3748/wjg.v12.i2.187. PMC 4066025. PMID 16482616.
- He M, Yang Y, Bian L, Cui H (September 1999). "[Effect of exogenous lactase on the absorption of lactose and its intolerance symptoms]". Wei Sheng Yan Jiu = Journal of Hygiene Research (in Chinese). 28 (5): 309–11. PMID 12712706.
- O'Connell S, Walsh G (August 2006). "Physicochemical characteristics of commercial lactases relevant to their application in the alleviation of lactose intolerance". Applied Biochemistry and Biotechnology. 134 (2): 179–91. doi:10.1385/ABAB:134:2:179. PMID 16943638. S2CID 22205720.
- Belloch, C.; Querol, A.; Barrio, E. (2011-01-01), "Yeasts and Molds | Kluyveromyces spp.", in Fuquay, John W. (ed.), Encyclopedia of Dairy Sciences (2nd ed.), San Diego: Academic Press, pp. 754–764, ISBN 978-0-12-374407-4, retrieved 2022-01-14
- Tally, Steve (1998). "Lactose intolerant? Drink more milk" (PDF). Agricultures Magazine. Vol. 1, no. 2. p. 2. Archived (PDF) from the original on 2006-09-04. Steve Tally
- Grenov B, Briend A, Sangild PT, Thymann T, Rytter MH, Hother AL, Mølgaard C, Michaelsen KF (March 2016). "Undernourished Children and Milk Lactose". Food and Nutrition Bulletin. 37 (1): 85–99. doi:10.1177/0379572116629024. PMID 26893059. S2CID 39762161.
- "Scientific Opinion on the substantiation of health claims related to live yoghurt cultures and improved lactose digestion (ID 1143, 2976) pursuant to Article 13(1) of Regulation (EC) No 1924/2006". EFSA Journal. 8 (10). 2010. doi:10.2903/j.efsa.2010.1763.
- Itan Y, Jones BL, Ingram CJ, Swallow DM, Thomas MG (February 2010). "A worldwide correlation of lactase persistence phenotype and genotypes". BMC Evolutionary Biology. 10 (1): 36. doi:10.1186/1471-2148-10-36. PMC 2834688. PMID 20144208.
- "Lactose intolerance". Genetics Home Reference. Archived from the original on 19 November 2016. Retrieved 18 November 2016.
- Schnorr SL, Sankaranarayanan K, Lewis CM, Warinner C (December 2016). "Insights into human evolution from ancient and contemporary microbiome studies". Current Opinion in Genetics & Development. 41: 14–26. doi:10.1016/j.gde.2016.07.003. PMC 5534492. PMID 27507098.
- Thompson, Helen (28 December 2012). "An Evolutionary Whodunit: How Did Humans Develop Lactose Tolerance?". NPR.org. Retrieved 2019-11-14.
- Pray, W. Steven (2000). "Lactose Intolerance: The Norm Among the World's Peoples" (PDF). American Journal of Pharmaceutical Education. 64 (2): 205–207. ProQuest 211177586. Archived from the original (PDF) on 2021-04-30. Retrieved 2019-11-20.
- Curry A (August 2013). "Archaeology: The milk revolution". Nature. 500 (7460): 20–2. Bibcode:2013Natur.500...20C. doi:10.1038/500020a. PMID 23903732. S2CID 4315860.
- McClure SB, Magill C, Podrug E, Moore AM, Harper TK, Culleton BJ, et al. (2018). "Fatty acid specific δ13C values reveal earliest Mediterranean cheese production 7,200 years ago". PLOS ONE. 13 (9): e0202807. Bibcode:2018PLoSO..1302807M. doi:10.1371/journal.pone.0202807. PMC 6124750. PMID 30183735.
- Keller A, Graefen A, Ball M, Matzas M, Boisguerin V, Maixner F, Leidinger P, Backes C, Khairat R, Forster M, Stade B, Franke A, Mayer J, Spangler J, McLaughlin S, Shah M, Lee C, Harkins TT, Sartori A, Moreno-Estrada A, Henn B, Sikora M, Semino O, Chiaroni J, Rootsi S, Myres NM, Cabrera VM, Underhill PA, Bustamante CD, Vigl EE, Samadelli M, Cipollini G, Haas J, Katus H, O'Connor BD, Carlson MR, Meder B, Blin N, Meese E, Pusch CM, Zink A (2012). "New insights into the Tyrolean Iceman's origin and phenotype as inferred by whole-genome sequencing". Nat Commun. 3: 698. Bibcode:2012NatCo...3..698K. doi:10.1038/ncomms1701. PMID 22426219.
- Wilson J (December 2005). "Milk Intolerance: Lactose Intolerance and Cow's Milk Protein Allergy". Newborn and Infant Nursing Reviews. 5 (4): 203–7. doi:10.1053/j.nainr.2005.08.004.
- Auricchio S, Rubino A, Landolt M, Semenza G, Prader A (August 1963). "Isolated Intestinal Lactase Deficiency in the Adult". Lancet. 2 (7303): 324–6. doi:10.1016/s0140-6736(63)92991-x. PMID 14044269.
- Simoons FJ (December 1969). "Primary adult lactose intolerance and the milking habit: a problem in biological and cultural interrelations. I. Review of the medical research". The American Journal of Digestive Diseases. 14 (12): 819–36. doi:10.1007/bf02233204. PMID 4902756. S2CID 22597839.
- Itan Y, Jones BL, Ingram CJ, Swallow DM, Thomas MG (February 2010). "A worldwide correlation of lactase persistence phenotype and genotypes". BMC Evolutionary Biology. 10: 36. doi:10.1186/1471-2148-10-36. PMC 2834688. PMID 20144208.
- Bayless TM, Rosensweig NS (September 1966). "A racial difference in incidence of lactase deficiency. A survey of milk intolerance and lactase deficiency in healthy adult males". JAMA. 197 (12): 968–72. doi:10.1001/jama.1966.03110120074017. PMID 5953213.
- Welsh JD, Rohrer V, Knudsen KB, Paustian FF (1967). "Isolated Lactase Deficiency: Correlation of Laboratory Studies and Clinical Data". Archives of Internal Medicine. 120 (3): 261–269. doi:10.1001/archinte.1967.00300030003003.
- Huang SS, Bayless TM (April 1968). "Milk and lactose intolerance in healthy Orientals". Science. 160 (3823): 83–4. Bibcode:1968Sci...160...83H. doi:10.1126/science.160.3823.83-a. PMID 5694356. S2CID 33249040.
- Cook GC, Kajubi SK (April 1966). "Tribal incidence of lactase deficiency in Uganda". Lancet. 1 (7440): 725–9. doi:10.1016/s0140-6736(66)90888-9. PMID 4159716.
- Jersky J, Kinsley RH (1967). "Lactase Deficiency in the South African Bantu". South African Medical Journal. 41 (46): 1194–6. PMID 6080167.
- Bolin TD, Crane GG, Davis AE (November 1968). "Lactose intolerance in various ethnic groups in South-East Asia". Australasian Annals of Medicine. 17 (4): 300–6. doi:10.1111/imj.1968.17.4.300. PMID 5701921.
- Flatz G, Saengudom C, Sanguanbhokhai T (February 1969). "Lactose intolerance in Thailand". Nature. 221 (5182): 758–9. Bibcode:1969Natur.221..758F. doi:10.1038/221758b0. PMID 5818369. S2CID 4201371.
- Elliott RB, Maxwell GM, Vawser N (January 1967). "Lactose maldigestion in Australian Aboriginal children". The Medical Journal of Australia. 1 (2): 46–9. doi:10.5694/j.1326-5377.1967.tb21011.x. PMID 6016903. S2CID 44475025.
- Flatz G, Rotthauwe HW (1971). "Evidence against nutritional adaption of tolerance to lactose". Humangenetik. 13 (2): 118–25. doi:10.1007/bf00295793. PMID 5114667. S2CID 33253438.
- Oh E, Jeremian R, Oh G, Groot D, Susic M, Lee K, et al. (January 2017). "Transcriptional heterogeneity in the lactase gene within cell-type is linked to the epigenome". Scientific Reports. 7: 41843. Bibcode:2017NatSR...741843O. doi:10.1038/srep41843. PMC 5282553. PMID 28139744.
External links
- Lactose intolerance at Curlie
- Wade, Nicholas (1 March 2010). "Human Culture, an Evolutionary Force". New York Times.