Descending colon
| Descending colon | |
|---|---|
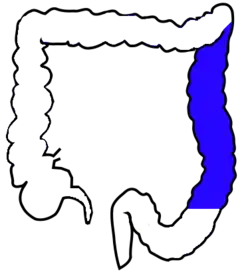 Drawing of colon seen from front (descending colon coloured blue) | |
 | |
| Details | |
| Precursor | Hindgut |
| System | Digestive system |
| Artery | Left colic artery |
| Vein | Left colic vein |
| Identifiers | |
| Latin | Colon descendens |
| MeSH | D044683 |
| TA98 | A05.7.03.006 |
| TA2 | 2986 |
| FMA | 14547 |
| Anatomical terminology | |
In the anatomy of humans and homologous primates, the descending colon is the part of the large intestine from the splenic flexure to the beginning of the sigmoid colon. The function of the descending colon in the digestive system is to store the remains of digested food that will be emptied into the rectum.
The descending colon is on the left side of the body (barring any malformations). The term left colon is hypernymous to descending colon in precise use; many casual mentions of the left colon chiefly concern the descending colon.
Structure

The descending colon begins at the splenic flexure at the upper left part of the abdomen. It passes downward through the left hypochondrium and lumbar regions, along the outer border of the left kidney and ends at the lower left part of the abdomen where it continues as the sigmoid colon. It is retroperitoneal in two-thirds of humans. In the other third, it has a (usually short) mesentery. The arterial supply comes via the left colic artery.
Function
While the first part of the large intestine is responsible for the absorption of water and other substances from the chyme, the main function of the descending colon is to store waste until it can be removed from the body in solid form, when a person has a bowel movement. The stools gradually solidify as they move along into the descending colon.[2]
Clinical significance
There are several diseases associated with the descending colon. Among the most common are the inflammatory bowel diseases (such as ulcerative colitis or Crohn’s disease) and colon cancer.
Ulcerative colitis
Ulcerative colitis can affect any part of the colon (and other mucosa, such as the mouth), but when it affects the descending colon, it is called left-sided colitis. Inflammation and ulcers on the lining of the intestine mark its presence. Symptoms of ulcerative colitis include diarrhea, bleeding, fever, abdominal pain, too much mucus in fecal material, and appetite and weight loss. Treatment methods can vary widely, ranging from changes in diet to drug therapy to corrective surgery, depending on the severity of the condition and the overall health of the patient.
Crohn’s disease
When a person has Crohn’s disease or Crohn’s colitis, they have lesions on the tissues of the intestine; this makes it hard for the intestine to absorb water and salt. The symptoms which may develop from this disease include abdominal pain, diarrhea or constipation, nausea and vomiting, fever, blood in the stool, weight loss, abscesses and fatigue. There is no cure for Crohn’s disease although many treatments are available. Symptomatic treatment with antidiarrhoeals is common in low level cases where the inflammation is reasonably under control. Steroid and/or sulphasalazine treatment are usually the first line of drug based management, although newer drugs along the TNF inhibitor line (such as infliximab and adalimumab) are becoming more widespread in the treatment of inflammatory colonic conditions. Diet and lifestyle changes can also be useful, as stress may exacerbate inflammatory processes.
Colon cancer
Cancer of the descending colon is a serious disease. A person can have colon cancer yet have no symptoms in the early stages. As such, regular colorectal examinations or fecal occult blood testing are necessary for catching the disease in its early stages. However, there are some signs that can indicate colon cancer; they include abrupt changes in bowel habits, bleeding from the rectum, black stools, frequent constipation, and mucus in the stools. Treatment options depend on the stage of the cancer and the overall health of the patient.
See also
References
- ↑ Nguyen H, Loustaunau C, Facista A, Ramsey L, Hassounah N, Taylor H, Krouse R, Payne CM, Tsikitis VL, Goldschmid S, Banerjee B, Perini RF, Bernstein C (2010). "Deficient Pms2, ERCC1, Ku86, CcOI in field defects during progression to colon cancer". J Vis Exp (41). doi:10.3791/1931. PMC 3149991. PMID 20689513.
- ↑ The Function Of The Colon Retrieved on 2010-01-21
External links
- Lotti M. Anatomy in relation to left colectomy
- Anatomy figure: 37:06-06 at Human Anatomy Online, SUNY Downstate Medical Center - "The large intestine."
- Anatomy photo:37:13-0100 at the SUNY Downstate Medical Center
| Authority control: Scientific databases |
|---|