Diagnosis of autism
The diagnosis of autism is based on a person's reported and directly observed behavior.[1] There are no known biomarkers for autism spectrum conditions that allow for a conclusive diagnosis.[2]
In most cases, diagnostic criteria codified in the World Health Organization's International Classification of Diseases (ICD) or the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM) are used. These reference manuals are regularly updated based on advances in research, systematic evaluation of clinical experience, and healthcare considerations. Currently, the DSM-5 published in 2013 and the ICD-10 that came into effect in 1994 are used, with the latter in the process of being replaced by the ICD-11 that came into effect in 2022 and is now implemented by healthcare systems across the world. Which autism spectrum diagnoses can be made and which criteria are used depends on the local healthcare system's regulations.
According to the DSM-5-TR (2022), in order to receive a diagnosis of autism spectrum disorder, one must present with "persistent deficits in social communication and social interaction" and "restricted, repetitive patterns of behavior, interests, or activities."[3] These behaviors must begin in early childhood and affect one's ability to perform everyday tasks. Furthermore, the symptoms must not be fully explainable by intellectual developmental disorder or global developmental delay.
Diagnostic process
There are several factors that make autism spectrum disorder difficult to diagnose. First off, there are no standardized imaging, molecular or genetic tests that can be used to diagnose ASD.[4] Additionally, there is a lot of variety in how ASD affects individuals. The behavioral manifestations of ASD depend on one's developmental stage, age of presentation, current support, and individual variability.[5][3] Lastly, there are multiple conditions that may present similarly to autism spectrum disorder, including intellectual disability, hearing impairment, a specific language impairment[6] such as Landau–Kleffner syndrome.[7] ADHD, anxiety disorder, and psychotic disorders.[8] Furthermore, the presence of autism can make it harder to diagnose coexisting psychiatric disorders such as depression.[9]
Ideally the diagnosis of ASD should be given by a team of clinicians (e.g. pediatricians, child psychiatrists, child neurologists) based on information provided from the affected individual, caregivers, other medical professionals and from direct observation.[10] Evaluation of a child or adult for autism spectrum disorder typically starts with a pediatrician or primary care physician taking a developmental history and performing a physical exam. If warranted, the physician may refer the individual to an ASD specialist who will observe and assess cognitive, communication, family, and other factors using standardized tools, and taking into account any associated medical conditions.[6] A pediatric neuropsychologist is often asked to assess behavior and cognitive skills, both to aid diagnosis and to help recommend educational interventions.[11] Further workup may be performed after someone is diagnosed with ASD. This may include a clinical genetics evaluation particularly when other symptoms already suggest a genetic cause.[12] Although up to 40% of ASD cases may be linked to genetic causes,[13] it is not currently recommended to perform complete genetic testing on every individual who is diagnosed with ASD. Consensus guidelines for genetic testing in patients with ASD in the US and UK are limited to high-resolution chromosome and fragile X testing.[12] Metabolic and neuroimaging tests are also not routinely performed for diagnosis of ASD.[12]
The age at which ASD is diagnosed varies. Sometimes ASD can be diagnosed as early as 18 months, however, diagnosis of ASD before the age of two years may not be reliable.[4] Diagnosis becomes increasingly stable over the first three years of life. For example, a one-year-old who meets diagnostic criteria for ASD is less likely than a three-year-old to continue to do so a few years later.[14] Additionally, age of diagnosis may depend on the severity of ASD, with more severe forms of ASD more likely to be diagnosed at an earlier age.[15] Issues with access to healthcare such as cost of appointments or delays in making appointments often lead to delays in the diagnosis of ASD.[16] In the UK the National Autism Plan for Children recommends at most 30 weeks from first concern to completed diagnosis and assessment, though few cases are handled that quickly in practice.[6] Lack of access to appropriate medical care, broadening diagnostic criteria and increased awareness surrounding ASD in recent years has resulted in an increased number of individuals receiving a diagnosis of ASD as adults. Diagnosis of ASD in adults poses unique challenges because it still relies on an accurate developmental history and because autistic adults sometimes learn coping strategies, known as "masking" or "camouflaging", which may make it more difficult to obtain a diagnosis.[17][18]
The presentation and diagnosis of autism spectrum disorder may vary based on sex and gender identity. Most studies that have investigated the impact of gender on presentation and diagnosis of autism spectrum disorder have not differentiated between the impact of sex versus gender.[19] There is some evidence that autistic women and girls tend to show less repetitive behavior and may engage in more camouflaging than autistic males.[20] Camouflaging may include making oneself perform normative facial expressions and eye contact.[21] Differences in behavioral presentation and gender-stereotypes may make it more challenging to diagnose autism spectrum disorder in a timely manner in females.[19][20] A notable percentage of autistic females may be misdiagnosed, diagnosed after a considerable delay, or not diagnosed at all.[20]
Considering the unique challenges in diagnosing ASD using behavioral and observational assessment, specific US practice parameters for its assessment were published by the American Academy of Neurology in the year 2000,[22] the American Academy of Child and Adolescent Psychiatry in 1999,[5] and a consensus panel with representation from various professional societies in 1999.[22] The practice parameters outlined by these societies include an initial screening of children by general practitioners (i.e., "Level 1 screening") and for children who fail the initial screening, a comprehensive diagnostic assessment by experienced clinicians (i.e. "Level 2 evaluation"). Furthermore, it has been suggested that assessments of children with suspected ASD be evaluated within a developmental framework, include multiple informants (e.g., parents and teachers) from diverse contexts (e.g., home and school), and employ a multidisciplinary team of professionals (e.g., clinical psychologists, neuropsychologists, and psychiatrists).[23]
As of 2019, psychologists wait until a child showed initial evidence of ASD tendencies, then administer various psychological assessment tools to assess for ASD.[23] Among these measurements, the Autism Diagnostic Interview-Revised (ADI-R) and the Autism Diagnostic Observation Schedule (ADOS) are considered the "gold standards" for assessing autistic children.[24][25] The ADI-R is a semi-structured parent interview that probes for symptoms of autism by evaluating a child's current behavior and developmental history. The ADOS is a semi-structured interactive evaluation of ASD symptoms that is used to measure social and communication abilities by eliciting several opportunities for spontaneous behaviors (e.g., eye contact) in standardized context. Various other questionnaires (e.g., The Childhood Autism Rating Scale, Autism Treatment Evaluation Checklist) and tests of cognitive functioning (e.g., The Peabody Picture Vocabulary Test) are typically included in an ASD assessment battery. The diagnostic interview for social and communication disorders (DISCO) may also be used.[26]
Screening
About half of parents of children with ASD notice their child's atypical behaviors by age 18 months, and about four-fifths notice by age 24 months.[14] If a child does not meet any of the following milestones, it "is an absolute indication to proceed with further evaluations. Delay in referral for such testing may delay early diagnosis and treatment and affect the [child's] long-term outcome."[22]
- No response to name (or gazing with direct eye contact) by 6 months.[27]
- No babbling by 12 months.
- No gesturing (pointing, waving, etc.) by 12 months.
- No single words by 16 months.
- No two-word (spontaneous, not just echolalic) phrases by 24 months.
- Loss of any language or social skills, at any age.
The Japanese practice is to screen all children for ASD at 18 and 24 months, using autism-specific formal screening tests. In contrast, in the UK, children whose families or doctors recognize possible signs of autism are screened. It is not known which approach is more effective.[28] The UK National Screening Committee does not recommend universal ASD screening in young children. Their main concerns includes higher chances of misdiagnosis at younger ages and lack of evidence of effectiveness of early interventions.[29] There is no consensus between professional and expert bodies in the US on screening for autism in children younger than 3 years.[31]
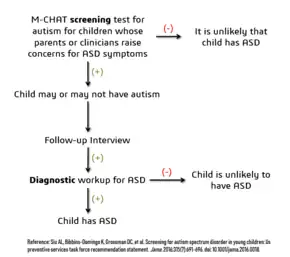
Screening tools include the Modified Checklist for Autism in Toddlers (M-CHAT), the Early Screening of Autistic Traits Questionnaire, and the First Year Inventory; initial data on M-CHAT and its predecessor, the Checklist for Autism in Toddlers (CHAT), on children aged 18–30 months suggests that it is best used in a clinical setting and that it has low sensitivity (many false-negatives) but good specificity (few false-positives).[14] It may be more accurate to precede these tests with a broadband screener that does not distinguish ASD from other developmental disorders.[32] Screening tools designed for one culture's norms for behaviors like eye contact may be inappropriate for a different culture.[33] Although genetic screening for autism is generally still impractical, it can be considered in some cases, such as children with neurological symptoms and dysmorphic features.[34]
Misdiagnosis
There is a significant level of misdiagnosis of autism in neurodevelopmentally typical children; 18–37% of children diagnosed with ASD eventually lose their diagnosis. This high rate of lost diagnosis cannot be accounted for by successful ASD treatment alone. The most common reason parents reported as the cause of lost ASD diagnosis was new information about the child (73.5%), such as a replacement diagnosis. Other reasons included a diagnosis given so the child could receive ASD treatment (24.2%), ASD treatment success or maturation (21%), and parents disagreeing with the initial diagnosis (1.9%).[30]
Many of the children who were later found not to meet ASD diagnosis criteria then received diagnosis for another developmental disorder. Most common was ADHD, but other diagnoses included sensory disorders, anxiety, personality disorder, or learning disability.[30] Neurodevelopment and psychiatric disorders that are commonly misdiagnosed as ASD include specific language impairment, social communication disorder, anxiety disorder, reactive attachment disorder, cognitive impairment, visual impairment, hearing loss and normal behavioral variation.[35] Some behavioral variations that resemble autistic traits are repetitive behaviors, sensitivity to change in daily routines, focused interests, and toe-walking. These are considered normal behavioral variations when they do not cause impaired function. Boys are more likely to exhibit repetitive behaviors especially when excited, tired, bored, or stressed. Some ways of distinguishing typical behavioral variations from autistic behaviors are the ability of the child to suppress these behaviors and the absence of these behaviors during sleep.[10]
See also
- Autism-spectrum quotient
References
- ↑ Baird G, Cass H, Slonims V (August 2003). "Diagnosis of autism". BMJ. 327 (7413): 488–493. doi:10.1136/bmj.327.7413.488. PMC 188387. PMID 12946972.
- ↑ Lord, Catherine; Charman, Tony; Havdahl, Alexandra; Carbone, Paul; Anagnostou, Evdokia; Boyd, Brian; Carr, Themba; de Vries, Petrus J; Dissanayake, Cheryl; Divan, Gauri; Freitag, Christine M; Gotelli, Marina M; Kasari, Connie; Knapp, Martin; Mundy, Peter (2022). "The Lancet Commission on the future of care and clinical research in autism". The Lancet. 399 (10321): 271–334. doi:10.1016/S0140-6736(21)01541-5. PMID 34883054. S2CID 244917920.
- 1 2 "Section 2: Neurodevelopmental Disorders". Diagnostic and statistical manual of mental disorders : DSM-5-TR (Print) (Fifth edition, text revision. ed.). Washington, DC: American Psychiatric Association Publishing. 2022. ISBN 978-0-89042-575-6.
- 1 2 CDC (31 March 2022). "Screening and Diagnosis | Autism Spectrum Disorder (ASD) | NCBDDD". Centers for Disease Control and Prevention. Retrieved 12 September 2022.
- 1 2 Volkmar F, Cook EH, Pomeroy J, Realmuto G, Tanguay P (December 1999). "Practice parameters for the assessment and treatment of children, adolescents, and adults with autism and other pervasive developmental disorders. American Academy of Child and Adolescent Psychiatry Working Group on Quality Issues". Journal of the American Academy of Child and Adolescent Psychiatry. 38 (12 Suppl): 32S–54S. doi:10.1016/s0890-8567(99)80003-3. PMID 10624084.
- 1 2 3 Dover CJ, Le Couteur A (June 2007). "How to diagnose autism". Archives of Disease in Childhood. 92 (6): 540–545. doi:10.1136/adc.2005.086280. PMC 2066173. PMID 17515625.
- ↑ Mantovani JF (May 2000). "Autistic regression and Landau-Kleffner syndrome: progress or confusion?". Developmental Medicine and Child Neurology. 42 (5): 349–353. doi:10.1017/S0012162200210621. PMID 10855658.
- ↑ Constantino JN, Charman T (March 2016). "Diagnosis of autism spectrum disorder: reconciling the syndrome, its diverse origins, and variation in expression" (PDF). The Lancet. Neurology. 15 (3): 279–91. doi:10.1016/s1474-4422(15)00151-9. PMID 26497771. S2CID 206162618.
- ↑ Matson JL, Neal D (2009). "Cormorbidity: diagnosing comorbid psychiatric conditions". Psychiatric Times. 26 (4). Archived from the original on 3 April 2013.
- 1 2 Simms MD (February 2017). "When Autistic Behavior Suggests a Disease Other than Classic Autism". Pediatric Clinics of North America. 64 (1): 127–138. doi:10.1016/j.pcl.2016.08.009. PMID 27894440.
- ↑ Kanne SM, Randolph JK, Farmer JE (December 2008). "Diagnostic and assessment findings: a bridge to academic planning for children with autism spectrum disorders". Neuropsychology Review. 18 (4): 367–384. doi:10.1007/s11065-008-9072-z. PMID 18855144. S2CID 21108225.
- 1 2 3 Caronna EB, Milunsky JM, Tager-Flusberg H (June 2008). "Autism spectrum disorders: clinical and research frontiers". Archives of Disease in Childhood. 93 (6): 518–523. doi:10.1136/adc.2006.115337. PMID 18305076. S2CID 18761374.
- ↑ Schaefer GB, Mendelsohn NJ (January 2008). "Genetics evaluation for the etiologic diagnosis of autism spectrum disorders". Genetics in Medicine. 10 (1): 4–12. doi:10.1097/GIM.0b013e31815efdd7. PMID 18197051. S2CID 4468548.
- 1 2 3 Landa RJ (March 2008). "Diagnosis of autism spectrum disorders in the first 3 years of life". Nature Clinical Practice. Neurology. 4 (3): 138–147. doi:10.1038/ncpneuro0731. PMID 18253102.
- ↑ Mandell DS, Novak MM, Zubritsky CD (December 2005). "Factors associated with age of diagnosis among children with autism spectrum disorders". Pediatrics. 116 (6): 1480–1486. doi:10.1542/peds.2005-0185. PMC 2861294. PMID 16322174.
- ↑ Shattuck PT, Grosse SD (2007). "Issues related to the diagnosis and treatment of autism spectrum disorders". Developmental Disabilities Research Reviews. 13 (2): 129–135. doi:10.1002/mrdd.20143. PMID 17563895.
- ↑ Huang Y, Arnold SR, Foley KR, Trollor JN (August 2020). "Diagnosis of autism in adulthood: A scoping review". Autism. 24 (6): 1311–1327. doi:10.1177/1362361320903128. PMID 32106698. S2CID 211556350.
- ↑ "6A02 Autism spectrum disorder". ICD-11 for Mortality and Morbidity Statistics. Retrieved 2023-05-05.
Some individuals with Autism Spectrum Disorder are capable of functioning adequately by making an exceptional effort to compensate for their symptoms during childhood, adolescence or adulthood. Such sustained effort, which may be more typical of affected females, can have a deleterious impact on mental health and well-being.
- 1 2 Lai MC, Szatmari P (March 2020). "Sex and gender impacts on the behavioural presentation and recognition of autism". Current Opinion in Psychiatry. 33 (2): 117–123. doi:10.1097/YCO.0000000000000575. PMID 31815760. S2CID 209164138.
- 1 2 3 Lockwood Estrin G, Milner V, Spain D, Happé F, Colvert E (29 October 2020). "Barriers to Autism Spectrum Disorder Diagnosis for Young Women and Girls: a Systematic Review". Review Journal of Autism and Developmental Disorders. Springer Science and Business Media LLC. 8 (4): 454–470. doi:10.1007/s40489-020-00225-8. PMC 8604819. PMID 34868805.
- ↑ Hull L, Petrides KV, Allison C, Smith P, Baron-Cohen S, Lai MC, Mandy W (August 2017). ""Putting on My Best Normal": Social Camouflaging in Adults with Autism Spectrum Conditions". Journal of Autism and Developmental Disorders. 47 (8): 2519–2534. doi:10.1007/s10803-017-3166-5. PMC 5509825. PMID 28527095.
- 1 2 3 Filipek PA, Accardo PJ, Ashwal S, Baranek GT, Cook EH, Dawson G, et al. (August 2000). "Practice parameter: screening and diagnosis of autism: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Child Neurology Society". Neurology. 55 (4): 468–79. doi:10.1212/wnl.55.4.468. PMID 10953176.
- 1 2 Ozonoff S, Goodlin-Jones BL, Solomon M (September 2005). "Evidence-based assessment of autism spectrum disorders in children and adolescents" (PDF). Journal of Clinical Child and Adolescent Psychology. Taylor & Francis. 34 (3): 523–40. doi:10.1207/s15374424jccp3403_8. ISSN 1537-4416. PMID 16083393. S2CID 14322690. Archived from the original (PDF) on 18 April 2021. Retrieved 3 September 2019.
- ↑ Corsello C, Hus V, Pickles A, Risi S, Cook EH, Leventhal BL, Lord C (September 2007). "Between a ROC and a hard place: decision making and making decisions about using the SCQ". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 48 (9): 932–40. doi:10.1111/j.1469-7610.2007.01762.x. eISSN 1469-7610. hdl:2027.42/74877. ISSN 0021-9630. OCLC 01307942. PMID 17714378.
- ↑ Huerta M, Lord C (February 2012). "Diagnostic evaluation of autism spectrum disorders". Pediatric Clinics of North America. 59 (1): 103–11, xi. doi:10.1016/j.pcl.2011.10.018. PMC 3269006. PMID 22284796.
- ↑ Kan CC, Buitelaar JK, van der Gaag RJ (June 2008). "Autismespectrumstoornissen bij volwassenen" [Autism spectrum disorders in adults]. Nederlands Tijdschrift voor Geneeskunde (in Dutch). 152 (24): 1365–1369. PMID 18664213.
- ↑ "Autism case training part 1: A closer look – key developmental milestones". CDC.gov. 18 August 2016. Retrieved 5 August 2019.
- ↑ Levy SE, Mandell DS, Schultz RT (November 2009). "Autism". Lancet. 374 (9701): 1627–1638. doi:10.1016/S0140-6736(09)61376-3. PMC 2863325. PMID 19819542. (Erratum: doi:10.1016/S0140-6736(11)61666-8, )
- 1 2 3 4 5 6 Siu AL, Bibbins-Domingo K, Grossman DC, Baumann LC, Davidson KW, Ebell M, et al. (February 2016). "Screening for Autism Spectrum Disorder in Young Children: US Preventive Services Task Force Recommendation Statement". JAMA. 315 (7): 691–696. doi:10.1001/jama.2016.0018. PMID 26881372.
- 1 2 3 Johnson CP, Myers SM (November 2007). "Identification and evaluation of children with autism spectrum disorders". Pediatrics. American Academy of Pediatrics. 120 (5): 1183–1215. doi:10.1542/peds.2007-2361. PMID 17967920. S2CID 218028., cited in Blumberg SJ, Zablotsky B, Avila RM, Colpe LJ, Pringle BA, Kogan MD (October 2016). "Diagnosis lost: Differences between children who had and who currently have an autism spectrum disorder diagnosis". Autism. 20 (7): 783–795. doi:10.1177/1362361315607724. PMC 4838550. PMID 26489772.
- ↑ For example:
- US Preventive Services Task Force does not recommend universal screen of young children for autism due to poor evidence of benefits of this screening when parents and clinicians have no concerns about ASD. The major concern is a false-positive diagnosis that would burden a family with very time-consuming and financially demanding treatment interventions when it is not truly required. The Task Force also did not find any robust studies showing effectiveness of behavioral therapies in reducing ASD symptom severity.[29]
- American Academy of Pediatrics recommends ASD screening of all children between the ages if 18 and 24 months.[29] The AAP also recommends that children who screen positive for ASD be referred to treatment services without waiting for a comprehensive diagnostic workup[30]
- The American Academy of Family Physicians did not find sufficient evidence of benefit of universal early screening for ASD[29]
- The American Academy of Neurology and Child Neurology Society recommends general routine screening for delayed or abnormal development in children followed by screening for ASD only if indicated by the general developmental screening[29]
- The American Academy of Child and Adolescent Psychiatry recommend routinely screening autism symptoms in young children[29]
- ↑ Wetherby AM, Brosnan-Maddox S, Peace V, Newton L (September 2008). "Validation of the Infant-Toddler Checklist as a broadband screener for autism spectrum disorders from 9 to 24 months of age". Autism. 12 (5): 487–511. doi:10.1177/1362361308094501. PMC 2663025. PMID 18805944.
- ↑ Wallis KE, Pinto-Martin J (May 2008). "The challenge of screening for autism spectrum disorder in a culturally diverse society". Acta Paediatrica. 97 (5): 539–540. doi:10.1111/j.1651-2227.2008.00720.x. PMID 18373717. S2CID 39744269.
- ↑ Lintas C, Persico AM (January 2009). "Autistic phenotypes and genetic testing: state-of-the-art for the clinical geneticist". Journal of Medical Genetics. 46 (1): 1–8. doi:10.1136/jmg.2008.060871. PMC 2603481. PMID 18728070.
- ↑ "Conditions That May Look Like Autism, but Aren't". WebMD. Retrieved 10 May 2020.