Diseases and epidemics of the 19th century

Diseases and epidemics of the 19th century included long-standing epidemic threats such as smallpox, typhus, yellow fever, and scarlet fever. In addition, cholera emerged as an epidemic threat and spread worldwide in six pandemics in the nineteenth century. The third plague pandemic emerged in China in the mid-nineteenth century and spread worldwide in the 1890s.
Medical responses
Medicine in the 19th century
Epidemics of the 19th century were faced without the medical advances that made 20th-century epidemics much rarer and less lethal. Micro-organisms (viruses and bacteria) had been discovered in the 18th century, but it was not until the late 19th century that the experiments of Lazzaro Spallanzani and Louis Pasteur disproved spontaneous generation conclusively, allowing germ theory and Robert Koch's discovery of micro-organisms as the cause of disease transmission. Thus throughout the majority of the 19th century, there was only the most basic, common-sense understanding of the causes, amelioration, and treatment of epidemic disease.
_1889.jpg.webp)
The 19th century did, however, mark a transformation period in medicine.[1] This included the first uses of chloroform and nitrous dioxides as anesthesia, important discoveries in regards of pathology and the perfection of the autopsy, and advances in our understanding of the human body.[1] Medical institutions were also transitioning to new hospital styles to try to prevent the spread of disease and stop over crowding with the mixing of the poor and the sick which had been a common practice.[1][2] With the increasing rise in urban population, disease and epidemic crisis became much more prevalent and was seen as a consequence of urban living.[1][2] Problems arose as both governments and the medical professionals at the time tried to get a handle on the spread of disease.[1] They had yet to figure out what actually causes disease.[1] So as those in authority scrambled to make leaps and bounds in science and track down what may be the cause of these epidemics, entire communities would be lost to the grips of terrible ailments.[1][2]
Exploring Potential Cures
During these many outbreaks, members of the medical professional rapidly began trying different cures to treat their patients.[3] During the cholera epidemic of 1832 in London one doctor had found a cure.[3] His name was Thomas Latta and he figured out that by injecting saline solutions into the arms of those infected, they would survive the disease.[3] But, because of the chaos of cures and treatments you could find being tried out on the streets, his cure was sub sequentially lost to the chaos of the times.[3] In fact, a lot was lost this way. At this time, with the increasing circulation of mass media and no form of content review in medical journals, almost anyone with or without proper education could publish a potential cure for disease.[3] Actual practicing medical professionals also had to compete with the ever expanding pharmacy companies that were all to ready to provide new elixirs and promising treatments for the epidemics of the time.[3]
Emerging from the medical chaos were legitimate and life changing treatments. The late 19th century was the beginning of widespread use of vaccines.[4][5] The cholera bacterium was isolated in 1854 by Italian anatomist Filippo Pacini,[6] and a vaccine, the first to immunize humans against a bacterial disease, was developed by Spanish physician Jaume Ferran i Clua in 1885,[7] and by Russian–Jewish bacteriologist Waldemar Haffkine in July 1892.[8]
Antibiotic drugs did not appear until the middle of the 20th century. Sulfonamides did not appear until 1935, and penicillin, discovered in 1928, was not available as a treatment until 1950.
A big response and potential cure to these epidemics were better sanitation in the cities.[9][10] Sanitation prior to this was very poor and sometimes attempts to get better sanitation often exacerbated the diseases, especially during the cholera epidemics because their understanding of diseases relied on the miasma (bad air) theory.[9] During the first cholera epidemic, Edwin Chadwick made an inquiry into sanitation and used quantitative data to link poor living conditions and disease and low life expectancy.[10][9] As a result, the Board of Health in London took measure to improve drainage and ventilation around the city. Unfortunately, the measures helped clean the city but it further contaminated the River Thames (the primary drinking water for the city) and the epidemic got worse.[9]
Beliefs about the Causes
During the second cholera pandemic of 1816–1837, the scientific community varied in its beliefs about its causes. In France, doctors believed cholera was associated with the poverty of certain communities or poor environment. Russians believed the disease was contagious and quarantined their citizens. The United States believed that cholera was brought by recent immigrants, specifically the Irish. Lastly, some British thought the disease might arise from divine intervention.[11]
During the third pandemic, Tunisia, which had not been affected by the two previous pandemics, thought Europeans had brought the disease. They blamed their sanitation practices. The prevalence of the disease in the South in areas of black populations convinced United States scientists that cholera was associated with African Americans. Current researchers note they lived near the waterways by which travelers and ships carried the disease and their populations were underserved with sanitation infrastructure and health care.[12]
The Soho outbreak in London in 1854 ended after the physician John Snow identified a neighborhood Broad Street pump as contaminated and convinced officials to remove its handle.[13] Snow believed that germ-contaminated water was the source of cholera, rather than particles in the air (referred to as "miasmata"). His study proved contaminated water was the main agent spreading cholera, although he did not identify the contaminant. Though Filippo Pacini had isolated Vibrio cholerae as the causative agent for cholera that year, it would be many years before miasma theory would fall out of favor.

In London, in June 1866[14]), a localized epidemic in the East End claimed 5,596 lives, just as the city was completing construction of its major sewage and water treatment systems. William Farr, using the work of John Snow, et al., as to contaminated drinking water being the likely source of the disease, relatively quickly identified the East London Water Company as the source of the contaminated water. Quick action prevented further deaths.[15]
During the fifth cholera pandemic, Robert Koch isolated Vibrio cholerae and proposed postulates to explain how bacteria caused disease. His work helped to establish the germ theory of disease. Prior to this time, many physicians believed that microorganisms were spontaneously generated, and disease was caused by direct exposure to filth and decay. Koch helped establish that the disease was more specifically contagious and was transmittable through the contaminated water supply. The fifth was the last serious European cholera outbreak, as cities improved their sanitation and water systems.
Cholera
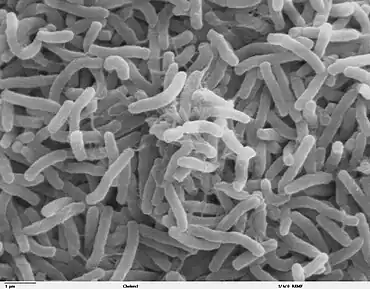
Cholera is an infection of the small intestine caused by the bacterium Vibrio cholerae. Cholera is transmitted primarily by drinking water or eating food[16] that has been contaminated by the cholera bacterium. The bacteria multiply in the small intestine;[17] the feces (waste product) of an infected person, including one with no apparent symptoms, can pass on the disease if it contacts the water supply by any means.[17]
History does not recount any incidents of cholera until the 19th century. Cholera came in seven waves, the last two of which occurred in the 20th century.
The first cholera pandemic started in 1816, spread across India by 1820,[18] and extended to Southeast Asia and Central Europe, lasting until 1826.
A second cholera pandemic began in 1829, reached Russia, causing the Cholera riots. It spread to Hungary, Germany and Egypt in 1831,[19] and London, Paris, Quebec, Ontario and New York City the following year.[15][20] Cholera reached the Pacific coast of North America by 1834, reaching into the center of the country by steamboat and other river traffic.[21]
The third cholera pandemic began in 1846 and lasted until 1860. It hit Russia hardest, with over one million deaths. In 1846, cholera struck Mecca, killing over 15,000.[22] A two-year outbreak began in England and Wales in 1848, and claimed 52,000 lives.[23] In 1849, outbreak occurred again in Paris, and in London, killing 14,137, over twice as many as the 1832 outbreak. Cholera hit Ireland in 1849 and killed many of the Irish Famine survivors, already weakened by starvation and fever.[24] In 1849, cholera claimed 5,308 lives in the major port city of Liverpool, England, an embarkation point for immigrants to North America, and 1,834 in Hull, England.[15] Cholera spread throughout the Mississippi River system.[15] Thousands died in New York City, a major destination for Irish immigrants.[15] Cholera claimed 200,000 victims in Mexico.[25] That year, cholera was transmitted along the California, Mormon and Oregon Trails, killing people that are believed to have died on their way to the California Gold Rush, Utah and Oregon in the cholera years of 1849–1855.[15][26][27][28] In 1851, a ship coming from Cuba carried the disease to Gran Canaria,[29] killing up to 6,000 people.[30]
The pandemic spread east to Indonesia by 1852, and China and Japan in 1854. The Philippines were infected in 1858 and Korea in 1859. In 1859, an outbreak in Bengal contributed to transmission of the disease by travelers and troops to Iran, Iraq, Arabia and Russia.[22] Japan suffered at least seven major outbreaks of cholera between 1858 and 1902. The Ansei outbreak of 1858–60, for example, is believed to have killed between 100,000 and 200,000 people in Tokyo alone.[31] An outbreak of cholera in Chicago in 1854 took the lives of 5.5% of the population (about 3,500 people).[15][32] In 1853–4, London's epidemic claimed 10,738 lives. Throughout Spain, cholera caused more than 236,000 deaths in 1854–55.[33] In 1854, it entered Venezuela; Brazil also suffered in 1855.[25]
The fourth cholera pandemic (1863–1875) spread mostly in Europe and Africa. At least 30,000 of the 90,000 Mecca pilgrims died from the disease. Cholera ravaged northern Africa in 1865 and southeastward to Zanzibar, killing 70,000 in 1869–70.[34] Cholera claimed 90,000 lives in Russia in 1866.[35] The epidemic of cholera that spread with the Austro-Prussian War (1866) is estimated to have taken 165,000 lives in the Austrian Empire.[36] In 1867, 113,000 lost their lives to cholera in Italy.[37] and 80,000 in Algeria.[34]
Outbreaks in North America in 1866–1873 killed some 50,000 Americans.[27] In 1866, localized epidemics occurred in the East End of London,[14][15] in southern Wales, and Amsterdam. In the 1870s, cholera spread in the U.S. as an epidemic from New Orleans along the Mississippi River and to ports on its tributaries.
In the fifth cholera pandemic (1881–1896), according to Dr A. J. Wall, the 1883–1887 part of the epidemic cost 250,000 lives in Europe and at least 50,000 in the Americas. Cholera claimed 267,890 lives in Russia (1892);[38] 120,000 in Spain;[39] 90,000 in Japan and over 60,000 in Persia.[38] In Egypt, cholera claimed more than 58,000 lives. The 1892 outbreak in Hamburg killed 8,600 people.
Smallpox
Smallpox is caused by either of the two viruses, Variola major and Variola minor. Smallpox vaccine was available in Europe, the United States, and the Spanish Colonies during the last part of the century.[4][5] The Latin names of this disease are Variola Vera. The words come from various (spotted) or varus (pimple). In England, this disease was first known as the "pox" or the "red plague". Smallpox settles itself in small blood vessels of the skin and in the mouth and throat. The symptoms of smallpox are rash on the skin and blisters filled with raised liquid.
The disease killed an estimated 400,000 Europeans annually during the 19th century and one-third of all the blindness of that time was caused by smallpox. 20 to 60% of all the people that were infected died and 80% of all the children with the infection also died. It caused also many deaths in the 20th century, over 300–500 million. Wolfgang Amadeus Mozart also had smallpox when he was only 11 years old. He survived the smallpox outbreak in Austria.
Typhus
Epidemic typhus is caused by the bacteria Rickettsia Prowazekii; it comes from lice. Murine typhus is caused by the Rickettsia Typhi bacteria, from the fleas on rats. Scrub typhus is caused by the Orientia Tsutsugamushi bacteria, from the harvest mites on humans and rodents. Queensland tick typhus is caused by the Rickettsia Australis bacteria, from ticks.
During Napoleon's retreat from Moscow in 1812, more French soldiers died of typhus than were killed by the Russians.[40] A major epidemic occurred in Ireland between 1816 and 1819, during the Year Without a Summer; an estimated 100,000 Irish perished. Typhus appeared again in the late 1830s, and between 1846 and 1849 during the Great Irish Famine. Spreading to England, and called "Irish fever", it was noted for its virulence. It killed people of all social classes, as lice were endemic and inescapable, but it hit particularly hard in the lower or "unwashed" social strata. In Canada alone, the typhus epidemic of 1847 killed more than 20,000 people from 1847 to 1848, mainly Irish immigrants in fever sheds and other forms of quarantine, who had contracted the disease aboard coffin ships.[41] In the United States, epidemics occurred in Baltimore, Memphis and Washington DC between 1865 and 1873, and during the US Civil War.
Yellow fever
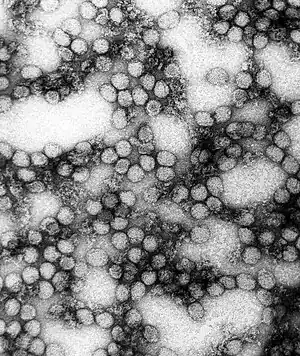
This disease is transmitted by the bite of female mosquito; the higher prevalence of transmission by Aedes aegypti has led to it being known as the Yellow Fever Mosquito. The transmission of yellow fever is entirely a matter of available habitat for vector mosquito and prevention such as mosquito netting. They mostly infect other primates, but humans can be infected. The symptoms of the fever are: Headaches, back and muscle pain, chills and vomiting, bleeding in the eyes and mouth, and vomit containing blood.
Yellow fever accounted for the largest number of the 19th-century's individual epidemic outbreaks, and most of the recorded serious outbreaks of yellow fever occurred in the 19th century. It is most prevalent in tropical-like climates, but the United States was not exempted from the fever.[42] New Orleans was plagued with major epidemics during the 19th century, most notably in 1833 and 1853. At least 25 major outbreaks took place in the Americas during the 18th and 19th centuries, including particularly serious ones in Santo Domingo in 1803[43][44] and Memphis in 1878.[45] Major outbreaks occurred repeatedly in Gibraltar; outbreaks in 1804, 1814, and again in 1828.[46] Barcelona suffered the loss of several thousand citizens during an outbreak in 1821. Urban epidemics continued in the United States until 1905, with the last outbreak affecting New Orleans.[47]
Plague
The third plague pandemic was a major bubonic plague pandemic that began in Yunnan, China in 1855.[48] This episode of bubonic plague spread to all inhabited continents in the 1890s and first years of the 1900s, and ultimately led to more than 12,000,000 deaths in India and China, with about 10,000,000 killed in India alone.[49]
A natural reservoir of plague is located in western Yunnan and is an ongoing health risk today. The third pandemic of plague originated in this area after a rapid influx of Han Chinese to exploit the demand for minerals, primarily copper, in the latter half of the 19th century.[50] By 1850, the population had exploded to over 7,000,000 people. Increasing transportation throughout the region brought people in contact with plague-infected fleas, the primary vector between the yellow-breasted rat (Rattus flavipectus) and humans. The spread of European empires and the development of new forms of transport such as the steam engine made it easier for both humans and rats to spread the disease along existing trade routes.
Scarlet Fever
Haemolytic streptococcus, which was identified in the 1880s,[51] causes scarlet fever, which is a bacterial disease.[52] Scarlet fever spreads through respiratory droplets and children between the ages of 5 to 15 years were most affected by scarlet fever.[53] Scarlet fever had several epidemic phases, and around 1825 to 1885 outbreaks began to recur cyclically and often highly fatal.[54] In the mid-19th century, the mortality caused by scarlet fever rose in England and Wales.[55] The major outbreak in England and Wales took place during 1825–1885 with high mortality marking this as remarkable.[52] There were several other notable outbreaks across Europe, South America, and the United States in the 19th century.[53]
Europe
In Europe, scarlet fever was considered benign for two centuries, but fatal epidemics were seen in the 1700s.[56] Scarlet fever broke out in England in the 19th century and was responsible for an enormous number of deaths in the 60-year period from 1825 to 1885; decades that followed had lower levels of annual mortality from scarlet fever.[52] In NW England there was heavy mortality in Liverpool.[52] Babies born in Liverpool with a birthday in 1861 were only expected to live 26 years, and in larger cities, life expectancy was less than 35 years.[51] Over time, the life expectancy changed as well as the number of fatalities from scarlet fever.[51] There was a reduction in child mortality from scarlet fever when you compare the decades, 1851–60 and 1891–1900.[51] The decline of mortality seen for scarlet fever was noticed after the identification of streptococcus,[51] but the decline was not associated with a treatment.[51] A treatment would not be available until the introduction of sulphonamides in the 1930s, and the decline in mortality was due to the quality of air, food, and water improving.[51] Outbreaks of scarlet fever also took place in Dublin in 1986 with 1,354 cases and 149 deaths, Norway from 1862 to 1884, Scotland in 1861, and in the United Kingdom.[53] The United Kingdom saw cases in Canterbury from 1839 to 1865 with 305 deaths, Bristol in 1870 with 106 deaths and in 1875, and Manchester in 1886 with six cases.[53]
South America
Chile reported scarlet fever the first time in 1827 and highest rates were seen during winter months.[53] The disease spread from Valparaiso to Santiago from 1831 to 1832 and claimed 7,000 lives.[53] There were multiple outbreaks in different locations of Chile, including Copaipo in 1875 and Caldera in 1876.[53]
United States
Similarly to Europe, America considered scarlet fever to be benign for two centuries.[56] In the early 19th century the scarlet fever impact drastically changed and lethal epidemics started to arise in the United States.[56] The United States had a notable outbreak of scarlet fever in Minnesota in 1847[53] and Augusta, Georgia had a lethal epidemic in 1832–1833.[56] Scarlet fever had low mortality rates in New York for many years before 1828, but remained high for long after.[56] Cases of scarlet fever were also seen in Boston during a period of decreasing severity after 1885.[56] Boston City Hospital opened a scarlet fever pavilion in 1887 to house patients with infectious diseases and saw nearly 25,000 patients during 1895–1905.[56] In the mid 1800s, more specific epidemiological information was emerging and incidence in infants were found to be low.[56] In 1870, the US census showed a decrease in scarlet fever mortality in children below the age of one.[56]
Citations
- 1 2 3 4 5 6 7 Bynun, W.F.; Hardy, Anne; Jacyn, Stephen; Lawrente, Christopher; Tanaey, E.M. (Tilli) (2006). The Western Medical Tradition 1800 to 2000. United States of America: Cambridge University Press. pp. 7–10, 150–156. ISBN 9780521475242.
- 1 2 3 Victoria and Albert Museum, Online Museum (14 July 2011). "Health & Medicine". www.vam.ac.uk. Retrieved 4 December 2020.
- 1 2 3 4 5 6 Johnson, Steven (2006). The Ghost Map: The Story of London's Most Terrifying Epidemic and How It Changed Science, Cities, and the Modern World. United States of America: Riverhead Books. ISBN 978-1-59448-925-9.
- 1 2 Stern AM, Markel H (2005). "The history of vaccines and immunization: familiar patterns, new challenges". Health Aff. (Millwood). 24 (3): 611–21. doi:10.1377/hlthaff.24.3.611. PMID 15886151.

- 1 2 Baxby, Derrick (1999). "Edward Jenner's Inquiry; a bicentenary analysis". Vaccine 17 (4): 301–07
- ↑ See:
- Fillipo Pacini (1854) "Osservazioni microscopiche e deduzioni patologiche sul cholera asiatico" (Microscopic observations and pathological deductions on Asiatic cholera), Gazzetta Medica Italiana: Toscana, 2nd series, 4 (50) : 397–401; 4 (51) : 405–412.
- Reprinted (more legibily) as a pamphlet.
- ↑ onlinelibrary.wiley.com
- ↑ haffkineinstitute.org
- 1 2 3 4 "Cholera in Victorian London". Science Museum. Retrieved 6 November 2020.
- 1 2 Mari, Christopher Mari (2007). Global Epidemics. New York: H.W Wilson Company. pp. 22–47. ISBN 9780824210687.
- ↑ Hayes, J.N. (2005). Epidemics and Pandemics: Their Impacts on Human History. Santa Barbara, CA: ABC-CLIO. pp. 214–219.
- ↑ Hayes, J.N. (2005). Epidemics and Pandemics: Their Impacts on Human History. Santa Barbara, CA: ABC-CLIO. p. 233.
- ↑ Snow, John (1855). On the Mode of Communication of Cholera.
- 1 2 Johnson, S: The Ghost Map(
- 1 2 3 4 5 6 7 8 Charles E. Rosenberg (1987). The cholera years: the United States in 1832, 1849 and 1866. Chicago: University of Chicago Press. ISBN 0-226-72677-0.
- ↑ Rita Colwell. Oceans, Climate, and Health: Cholera as a Model of Infectious Diseases in a Changing Environment. Rice University: James A Baker III Institute for Public Policy. Retrieved 23 October 2013.
- 1 2 Ryan KJ, Ray CG (editors) (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. pp. 376–7. ISBN 0-8385-8529-9.
{{cite book}}:|author=has generic name (help) - ↑ Pike J (23 October 2007). "Cholera – Biological Weapons". Weapons of Mass Destruction (WMD). GlobalSecurity.com. Retrieved 1 February 2010.
- ↑ Cholera Epidemic in Egypt (1947) Archived 22 November 2010 at the Wayback Machine.
- ↑ Asiatic Cholera Pandemic of 1826–37
- ↑ Wilford JN (15 April 2008). "How Epidemics Helped Shape the Modern Metropolis". The New York Times. Retrieved 1 February 2010.
On a Sunday in July 1832, a fearful and somber crowd of New Yorkers gathered in City Hall Park for more bad news. The epidemic of cholera, cause unknown and prognosis dire, had reached its peak.
- 1 2 Asiatic Cholera Pandemic of 1846–63. UCLA School of Public Health.
- ↑ Cholera's seven pandemics, cbc.ca, 2 December 2008.
- ↑ "The Irish Famine". Archived from the original on 27 October 2009. Retrieved 9 June 2014.
{{cite web}}: CS1 maint: bot: original URL status unknown (link) - 1 2 Byrne, Joseph Patrick (2008). Encyclopedia of Pestilence, Pandemics, and Plagues: A-M. ABC-CLIO. p. 101. ISBN 978-0-313-34102-1.
- ↑ Unruh, John David (1993). The plains across: the overland emigrants and the trans-Mississippi West, 1840–60. Urbana, IL: University of Illinois Press. pp. 408–10. ISBN 0-252-06360-0.
- 1 2 Beardsley GW (2000). "The 1832 Cholera Epidemic in New York State: 19th Century Responses to Cholerae Vibrio (part 2)". The Early America Review. 3 (2). Retrieved 1 February 2010.
- ↑ Vibrio cholerae in recreational beach waters and tributaries of Southern California.
- ↑ http://coloquioscanariasamerica.casadecolon.com/index.php/CHCA/article/viewFile/9072/8523 p.626
- ↑ mdc.ulpgc.es/cdm/ref/collection/MDC/id/44370 p.545–546
- ↑ Kaoru Sugihara, Peter Robb, Haruka Yanagisawa, Local Agrarian Societies in Colonial India: Japanese Perspectives, (1996), p. 313.
- ↑ Chicago Daily Tribune Archived 20 February 2008 at the Wayback Machine, 12 July 1854
- ↑ Kohn, George C. (2008). Encyclopedia of Plague and Pestilence: from Ancient Times to the Present. Infobase Publishing. p. 369. ISBN 978-0-8160-6935-4.
- 1 2 Byrne, Joseph Patrick (2008). Encyclopedia of Pestilence, Pandemics, and Plagues: A-M. ABC-CLIO. p. 107. ISBN 978-0-313-34102-1.
- ↑ Eastern European Plagues and Epidemics 1300–1918 Archived 5 June 2011 at the Wayback Machine.
- ↑ Matthew R. Smallman-Raynor PhD and Andrew D. Cliff DSc, Impact of Infectious Diseases on War. .
- ↑ Vibrio Cholerae and Cholera – The History and Global Impact Archived 16 December 2008 at the Wayback Machine.
- 1 2 Chisholm, Hugh, ed. (1911). . Encyclopædia Britannica. Vol. 6 (11th ed.). Cambridge University Press. pp. 262–267.
- ↑ "The cholera in Spain". The New York Times. 20 June 1890. Retrieved 8 December 2008.
- ↑ The Historical Impact of Epidemic Typhus Archived 14 November 2009 at WebCite. Joseph M. Conlon.
- ↑ "M993X.5.1529.1 | The government inspector's office". McCord Museum. Montreal. Retrieved 22 January 2012.
- ↑ Miller, Jacquelyn C (2005). "The Wages of Blackness: African American Workers and the Meanings of Race during Philadelphia's 1793 Yellow Fever Epidemic". The Pennsylvania Magazine of History and Biography. 129 (2): 163–194.
- ↑ Bruns, Roger (2000). Almost History: Close Calls, Plan B's, and Twists of Fate in American History. Hyperion. ISBN 0-7868-8579-3.
- ↑ Marr, J. S., & Cathey, J. T. (n.d.). The 1802 Saint-Domingue yellow fever epidemic and the Louisiana Purchase. Journal of Public Health Management and Practice, 19(1), 77–82. doi:10.1097/PHH.0b013e318252eea8
- ↑ Khaled J. Bloom, The Mississippi Valley's Great Yellow Fever Epidemic of 1878, Louisiana State U. Press, 1993
- ↑ "Gibraltar's 1804 Yellow Fever Scourge: The Search for Scapegoats". Oxford Journals—Journal of the History of Medicine and Allied Sciences. Archived from the original on 16 March 2011. Retrieved 5 April 2013.
- ↑ John Pierce; Jim Writer (2005). Yellow Jack: How Yellow Fever ravaged America and Walter Reed Discovered Its Deadly Secrets. Hoboken: John Wiley & Sons. p. 3.
- ↑ Cohn, Samuel K. (2003). The Black Death Transformed: Disease and Culture in Early Renaissance Europe. A Hodder Arnold. p. 336. ISBN 0-340-70646-5.
- ↑ Infectious Diseases: Plague Through History, sciencemag.org
- ↑ Benedict, Carol (1996). Bubonic plague in eighteenth-century China. Stanford, CA: Stanford Univ. Press. pp. 47, 70. ISBN 978-0804726610.
- 1 2 3 4 5 6 7 Woods, Robert; Woodward, John (1984). Urban Disease and Mortality in the Nineteenth Century. St. Martin's Press Inc. pp. 37–67.
- 1 2 3 4 Duncan, S.R.; Scott, Susan; Duncan, C.T. (2000). "Modelling the Dynamics of Scarlet Fever Epidemics in the 19th Century". European Journal of Epidemiology. Springer. 16 (7): 619–626. doi:10.1023/A:1007645110006. PMID 11078118. S2CID 12451068 – via JSTOR.
- 1 2 3 4 5 6 7 8 Berger, Stephen. Rheumatic Fever and Scarlet Fever: Global Status. Gideon Informatics, Inc. pp. 54–104. ISBN 978-1-4988-1653-3.
- ↑ Looper, Michael de (2017). "'This Most Dreadful Scourge': Scarlet Fever in Sydney". Health and History, Incarceration, Migration, Dispossession, and Discovery: Medicine in Colonial Australia. Australian and New Zealand Society of the History of Medicine. 19 (2): 116–133 – via JSTOR.
- ↑ Duncan, C.T.; Duncan, S.R.; Scott, S. (December 1996). "The Dynamics of Scarlet Fever Epidemics in England and Wales in the 19th Century". Epidemiology and Infection. Cambridge University Press. 117 (3): 493–499. doi:10.1017/S0950268800059161. PMC 2271647. PMID 8972674 – via JSTOR.
- 1 2 3 4 5 6 7 8 9 Katz, Alan R.; Morens, David M. (January 1992). "Severe Streptoccal Infections in Historical Perspective". Clinical Infectious Diseases. 14: 298–307. doi:10.1093/clinids/14.1.298. PMID 1571445 – via JSTOR.