Persistent cloaca
| Persistent cloaca | |
|---|---|
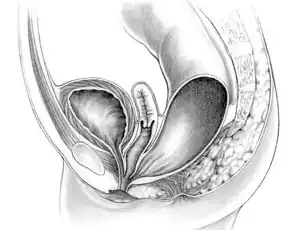 | |
| Diagram of a female with persistent cloaca | |
| Specialty | Medical genetics |
A persistent cloaca is a symptom of a complex anorectal congenital disorder, in which the rectum, vagina, and urinary tract meet and fuse, creating a cloaca, a single common channel.[1]
Signs and symptoms
Cloacas appear in a wide spectrum of variation in females born with the malformation. The single orifice, called a common channel, may occur varying in length from 1 to 10 cm. The length of the common channel can be used to judge prognostic outcomes and technical challenges during surgical repair. A common channel less than 3 cm in length usually has good sphincter muscles and a well-developed sacrum.
Diagnosis
Diagnosis of a female with cloaca should be suspected in a female born with an imperforate anus and small looking genitalia. The diagnosis can be made clinically. Failure to identify a cloaca as being present in a newborn may be dangerous, as more than 90% have associated urological problems. The goal for treatment of a female born with cloaca is to achieve bowel control, urinary control, and sexual function, which includes menstruation, sexual intercourse, and possibly pregnancy. Cloacas probably occur in 1 in 20,000 live births.[2][3]
Treatment
The prognostic outcomes for this type of cloaca are good for bowel control and urinary function. The surgical repair for this type of cloaca can usually be done by performing posterior sagittal approach without opening of the abdomen. A common channel longer than 3 cm in length usually has poor sphincter muscles and a poor sacrum, suggesting a prognostic outcome for bowel control and urinary function to be less likely. Common channels longer than 3 cm are generally considered more complex and more technically challenging in surgical repair.[2]
See also
- Cloaca (embryology)
- Cloaca
References
- ↑ Jenkins D, Bitner-Glindzicz M, Thomasson L, et al. (2007), "Mutational analyses of UPIIIA, SHH, EFNB2 and HNF1β in persistent cloaca and associated kidney malformations", J Pediatr Urol, 3 (1): 2–9, doi:10.1016/j.jpurol.2006.03.002, PMC 1864944, PMID 17476318.
- 1 2 Spitz, Lewis; Coran, Arnold G (2006), Operative Pediatric Surgery (6th ed.), London: Hodder Arnold, pp. 503–519.
- ↑ Ashcroft, Keith; Holcomb, George; Murphy, J Patrick (2005), Pediatric Surgery (4th ed.), Philadelphia: Elsevier Saunders, pp. 496–517.