Cryptosporidium
Cryptosporidium, sometimes called crypto, is an apicomplexan genus of alveolates which are parasites that can cause a respiratory and gastrointestinal illness (cryptosporidiosis) that primarily involves watery diarrhea (intestinal cryptosporidiosis), sometimes with a persistent cough (respiratory cryptosporidiosis).[1][2]
| Cryptosporidium | |
|---|---|
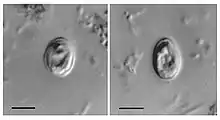 | |
| Oocysts of C. muris found in human feces | |
| Scientific classification | |
| Domain: | Eukaryota |
| Clade: | Diaphoretickes |
| Clade: | SAR |
| Clade: | Alveolata |
| Phylum: | Apicomplexa |
| Class: | Conoidasida |
| Order: | Eucoccidiorida |
| Suborder: | Eimeriorina |
| Family: | Cryptosporidiidae |
| Genus: | Cryptosporidium Tyzzer, 1907 |
| Species | |
|
See § Species | |
Treatment of gastrointestinal infection in humans involves fluid rehydration, electrolyte replacement, and management of any pain. For cryptosporidiosis, supportive treatment and symptom management are the primary treatments for immunocompetent individuals.[3] Anti-diarrheal medication may be effective in slowing the rate of diarrhea, including Loperamide. Nitazoxanide is the only drug approved for the treatment of cryptosporidiosis in immunocompetent persons.[4] Supplemental zinc may improve symptoms,[5] particularly in recurrent or persistent infections or in others at risk for zinc deficiency. Cryptosporidium oocysts are 4–6 μm in diameter and exhibit partial acid-fast staining. They must be differentiated from other partially acid-fast organisms including Cyclospora cayetanensis.
General characteristics
Cryptosporidium causes cryptosporidiosis, an infection that may present as a diarrhea, sometimes with a persistent cough in immunocompetent hosts.[1] Other apicomplexan pathogens include the malaria parasite Plasmodium and the toxoplasmosis parasite Toxoplasma. Unlike Plasmodium, which transmits via a mosquito vector, Cryptosporidium does not use an insect vector, and is capable of completing its lifecycle within a single host, resulting in cyst stages that are excreted in feces or through inhalation of coughed on fomites and are capable of transmission to a new host.[1][6][7]
A number of species infect mammals. In humans, the main causes of disease are C. parvum and C. hominis (previously C. parvum genotype 1). C. canis, C. felis, C. meleagridis, and C. muris can also cause disease in humans.[6]
Cryptosporidiosis is typically an acute, short-term infection, can be recurrent through reinfection in immunocompetent hosts, and become severe or life-threatening in immunocompromised individuals. In humans, it remains in the lower intestine and may remain for up to five weeks.[6] The parasite is transmitted by environmentally hardy cysts (oocysts) that, once ingested, exist in the small intestine and result in an infection of intestinal epithelial tissue.[6] Transmission by ingestion or inhalation of coughed on fomites is a second, less likely route of infection.[1]
The genome of C. parvum, sequenced in 2004, was found to be unusual amongst eukaryotes in that the mitochondria seem not to contain DNA.[8] A closely related species, C. hominis, also has its genome sequence available.[9]
Life cycle

Cryptosporidium has three developmental stages: meronts, gamonts and oocysts.[10] They reproduce within the intestinal epithelial cells.[11] The Cryptosporidium spore phase (oocyst) can survive for lengthy periods outside a host. It can also resist many common disinfectants, including chlorine-based disinfectants.[12]
Water treatment and detection
Many treatment plants that take raw water from rivers, lakes, and reservoirs for public drinking water production use conventional filtration technologies. Direct filtration, which is typically used to treat water with low particulate levels, includes coagulation and filtration but not sedimentation. Other common filtration processes including slow sand filters, diatomaceous earth filters, and membranes will remove 99% of Cryptosporidium.[13] Membranes and bag- and cartridge-filter products remove Cryptosporidium specifically.
Cryptosporidium is highly resistant to chlorine disinfection;[14] but with high enough concentrations and contact time, Cryptosporidium inactivation will occur with chlorine dioxide and ozone treatment. In general, the required levels of chlorine preclude the use of chlorine disinfection as a reliable method to control Cryptosporidium in drinking water. Ultraviolet light treatment at relatively low doses will inactivate Cryptosporidium. Calgon Carbon-funded research originally discovered UV's efficacy in inactivating Cryptosporidium.[15][16]
One of the largest challenges in identifying outbreaks is the ability to verify the results in a laboratory. The oocytes may be seen by microscopic examination of a stool sample, but they may be confused with other objects or artifacts similar in appearance.[17] Most cryptosporidia are 3–6 μm in size, although some reports have described larger cells.[17]
Boiling is believed to be the safest option for water contaminated by Cryptosporidium.[18][19]
Epidemiology

Exposure risks
- People who swim regularly in pools with insufficient sanitation (certain strains of Cryptosporidium are chlorine-resistant)
- Child-care workers
- Parents of infected children
- People caring for other people with cryptosporidiosis
- Backpackers, hikers, and campers who drink unfiltered, untreated water
- People who visit petting farms and open farms with public access[20]
- People, including swimmers, who swallow water from contaminated sources
- People handling infected cattle
- People exposed to human feces
- People who turn compost that has not gone through its phase where temperatures over 50 °C are reached[21]
Dealing with stabilized compost - i.e. composting material that has gone through the phases where micro-organisms are digesting the organic matter and the temperature inside the composting pile has reached temperature up to 50–70 °C – poses very little risk as these temperatures kill pathogens and even make oocysts unviable.[21]
Like many fecal-oral pathogens, the disease can also be transmitted by contaminated food, poor hygiene or turning compost in a local compost site. Testing of water, as well as epidemiological study, are necessary to determine the sources of specific infections. Cryptosporidium typically does not cause serious illness in healthy people. It may chronically sicken some children, as well as adults exposed and immunocompromised.
Species
- Cryptosporidium andersoni
- Cryptosporidium bailey
- Cryptosporidium bovis
- Cryptosporidium cervine
- Cryptosporidium canis
- Cryptosporidium cuniculus
- Cryptosporidium ducismarci
- Cryptosporidium fayeri
- Cryptosporidium felis
- Cryptosporidium fragile
- Cryptosporidium galli
- Cryptosporidium hominis
- Cryptosporidium marcopodum
- Cryptosporidium meleagridis
- Cryptosporidium molnari
- Cryptosporidium muris
- Cryptosporidium parvum
- Cryptosporidium ryanae
- Cryptosporidium saurophilum
- Cryptosporidium serpentis
- Cryptosporidium suis
- Cryptosporidium ubiquitum
- Cryptosporidium viatorum
- Cryptosporidium wrairi
- Cryptosporidium xiaoi
See also
References
- Sponseller JK, Griffiths JK, Tzipori S (July 2014). "The evolution of respiratory Cryptosporidiosis: evidence for transmission by inhalation". Clinical Microbiology Reviews. 27 (3): 575–86. doi:10.1128/CMR.00115-13. PMC 4135895. PMID 24982322.
Recent evidence indicates that respiratory cryptosporidiosis may occur commonly in immunocompetent children with cryptosporidial diarrhea and unexplained cough. Findings from animal models, human case reports, and a few epidemiological studies suggest that Cryptosporidium may be transmitted via respiratory secretions, in addition to the more recognized fecal-oral route. ... Upper respiratory cryptosporidiosis may cause inflammation of the nasal mucosa, sinuses, larynx, and trachea, accompanied by nasal discharge and voice change (54, 61, 62). Cryptosporidiosis of the lower respiratory tract typically results in productive cough, dyspnea, fever, and hypoxemia (63,–66). ... While fecal-oral transmission is indisputably the major route of infection, transmission via coughing and fomites is also possible in situations of close contact (20). ... Because they lacked gastrointestinal symptoms and oocyst excretion, the latter cases establish the possibility of primary respiratory infection with Cryptosporidium, which may have been acquired by inhalation of expectorated droplets or by contact with fomites. ... This finding suggests that respiratory cryptosporidiosis may occur commonly in immunocompetent individuals.
- Chalmers, Rachel M.; Davies, Angharad P.; Tyler, Kevin (1 May 2019). "Cryptosporidium". Microbiology. 165 (5): 500–502. doi:10.1099/mic.0.000764. ISSN 1350-0872. PMID 31268415. S2CID 243706992.
- Leder, Karin. "Cryptosporidiosis: Treatment and Prevention". UpToDate. Retrieved 4 August 2023.
- Love, MS; Choy, RKM (1 October 2021). "Emerging treatment options for cryptosporidiosis". Current Opinion in Infectious Diseases. 34 (5): 455–462. doi:10.1097/QCO.0000000000000761. PMC 7611666. PMID 34261904.
- Cabada MM, White AC, Venugopalan P, Sureshbabu J (18 August 2015). Bronze MS (ed.). "Cryptosporidiosis Treatment & Management". Medscape. WebMD. Retrieved 8 January 2016.
Infection may improve with nutritional supplementation, particularly with regimens including zinc or glutamine. ... Nitazoxanide significantly shortens the duration of diarrhea and can decrease the risk of mortality in malnourished children.[22] Trials have also demonstrated efficacy in adults.[26, 27] ... Symptomatic therapy includes replacement of fluids, provision of appropriate nutrition, and treatment with antimotility agents. ... Replacement of fluids and electrolytes is the critically important first step in the management of cryptosporidiosis, particularly in patients with large diarrheal losses. Fluids should include sodium, potassium, bicarbonate, and glucose.
- "Parasites – Cryptosporidium (also known as "Crypto")". Centers for Disease Control and Prevention. 20 February 2015.
- Widmer, Giovanni; Carmena, David; Kváč, Martin; Chalmers, Rachel M.; Kissinger, Jessica C.; Xiao, Lihua; Sateriale, Adam; Striepen, Boris; Laurent, Fabrice; Lacroix-Lamandé, Sonia; Gargala, Gilles; Favennec, Loïc (2020). "Update on Cryptosporidium spp.: highlights from the Seventh International Giardia and Cryptosporidium Conference". Parasite. 27: 14. doi:10.1051/parasite/2020011. ISSN 1776-1042. PMC 7069357. PMID 32167464.

- Abrahamsen MS, Templeton TJ, Enomoto S, Abrahante JE, Zhu G, Lancto CA, Deng M, Liu C, Widmer G, Tzipori S, Buck GA, Xu P, Bankier AT, Dear PH, Konfortov BA, Spriggs HF, Iyer L, Anantharaman V, Aravind L, Kapur V (April 2004). "Complete genome sequence of the apicomplexan, Cryptosporidium parvum". Science. 304 (5669): 441–5. Bibcode:2004Sci...304..441A. doi:10.1126/science.1094786. PMID 15044751. S2CID 26434820.
- Xu P, Widmer G, Wang Y, Ozaki LS, Alves JM, Serrano MG, Puiu D, Manque P, Akiyoshi D, Mackey AJ, Pearson WR, Dear PH, Bankier AT, Peterson DL, Abrahamsen MS, Kapur V, Tzipori S, Buck GA (October 2004). "The genome of Cryptosporidium hominis". Nature. 431 (7012): 1107–12. Bibcode:2004Natur.431.1107X. doi:10.1038/nature02977. PMID 15510150.
- "Cryptosporidium". The Australian Society for Parasitology Inc. Retrieved 7 August 2019.
- Ash, Lawrence; Orihel, Thomas (2007). Ash & Orihel's Atlas of Human Parasitology (5th ed.). American Society for Clinical Pathology Press.
- "Chlorine Disinfection of Recreational Water for Cryptosporidium parvum". CDC. Retrieved 6 May 2007.
- "The Interim Enhanced Surface Water Treatment Rule – What Does it Mean to You?" (PDF). USEPA. Retrieved 6 May 2007.
- Korich DG, Mead JR, Madore MS, Sinclair NA, Sterling CR (May 1990). "Effects of ozone, chlorine dioxide, chlorine, and monochloramine on Cryptosporidium parvum oocyst viability". Applied and Environmental Microbiology. 56 (5): 1423–8. Bibcode:1990ApEnM..56.1423K. doi:10.1128/aem.56.5.1423-1428.1990. PMC 184422. PMID 2339894.
- Bolton, JR, Dussert, B, Bukhari, Z, Hargy, TM, Clancy, JL (1998). "Inactivation of Cryptosporidium parvum by Medium-Pressure Ultraviolet Light in Finished Drinking Water". Proc. AWWA 1998 Annual Conference, Dallas, TX. A: 389–403.
- Bukhari Z, Hargy TM, Bolton JR, Dussert B, Clancy JL (1999). "Medium Pressure UV Light for Oocyst Inactivation". Journal of the American Water Works Association. 91 (3): 86–94. doi:10.1002/j.1551-8833.1999.tb08602.x. S2CID 87880510.
- Casemore DP, Armstrong M, Sands RL (December 1985). "Laboratory diagnosis of cryptosporidiosis". Journal of Clinical Pathology. 38 (12): 1337–41. doi:10.1136/jcp.38.12.1337. PMC 499488. PMID 2416782.
- "Boil water warning 'precaution'". BBC News. 2 September 2008.
- "Boil water 'into January' warning". BBC News. 30 November 2005.
- Walker MD (2018). "Reducing the risk of zoonotic infection". Conservation Land Management. 16 (2): 19–22.
- Gerba, C. (1 August 1995). "Occurrence of enteric pathogens in composted domestic solid waste containing disposable diapers". Waste Management & Research. 13 (4): 315–324. doi:10.1016/S0734-242X(95)90081-0. ISSN 0734-242X.
Further reading
- White AC (2005). "Cryptosporidiosis". In Mandell G (ed.). Principles and Practice of Infectious Diseases (6th ed.). Elsevier. pp. 3215–28.
- Upton SJ (12 September 2003). "Basic Biology of Cryptosporidium". Kansas State University: Parasitology Laboratory.
- Brands SJ (2000). "The Taxonomicon & Systema Naturae". Taxon: Genus Cryptosporidium. Universal Taxonomic Services, Amsterdam, the Netherlands. Archived from the original on 23 September 2018. Retrieved 13 October 2006.
- United States Environmental Protection Agency (March 2001). "Cryptosporidium: Drinking Water Advisory" (PDF). EPA-822-R-01-009. Retrieved 4 March 2013.
- World Health Organization (2009). "Risk Assessment of Cryptosporidium in Drinking Water" (PDF). WHO/HSE/WSH/09.04. Retrieved 4 March 2013.