Caffeinism
Caffeinism is a state of intoxication caused by excessive consumption of caffeine. This intoxication covers a variety of unpleasant physical and mental symptoms associated with the consumption of excessive amounts of caffeine.[1]
| Caffeinism | |
|---|---|
| Other names | Caffeine overdose |
| Specialty | Toxicology, psychiatry |
Caffeine is considered one of the most widely consumed drugs around the world. Around 80% of the world population consumes caffeine in one form or another.[2] It is found in coffee, tea, caffeinated alcoholic drinks, cocoa, chocolate, soft drinks, especially cola, and is an important component of energy drinks and other dietary supplements.[1]
Caffeine is also an ingredient of several medications, many of them over-the-counter and prescription drugs. The consensus is to consider caffeine a drug with pharmacological effects acting throughout the body.
Signs and symptoms
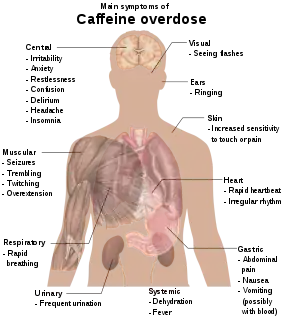
In moderate doses, caffeine is used to reduce physical fatigue, to prevent drowsiness and sleep, and to maintain and restore mental alertness and wakefulness. However, at higher doses, these stimulatory effects can become excessive and lead to a wide range of unpleasant symptoms including a dysphoric physical and mental state that is labeled caffeinism and is also known colloquially as "coffee nerves" or "caffeine jitters." These symptoms including nervousness, irritability, restlessness, insomnia, headaches, and palpitations after caffeine use.[4]
Caffeinism usually occurs when consumption of caffeine reaches 1–1.5 grams (0.035–0.053 oz) per day.[5] For reference, a brewed 8oz (227ml) cup of coffee contains ~95 mg of caffeine (per USDA).[6]
According to the Diagnostic and Statistical Manual of Mental Disorders, caffeine overdose can result in a state of excessive stimulation of the central nervous system and the essential feature of Caffeine Intoxication is the recent consumption of caffeine. This diagnosis requires the presence of at least five signs or symptoms, from a list of 12, that develop during or shortly after caffeine use.[7] This syndrome regularly happens when a person ingested large amounts of caffeine from any source (e.g., more than 400–500 mg at a time).
The signs and symptoms are divided into one group that can appear after an intake of as little as 100 mg of caffeine (roughly the amount contained in a cup of brewed coffee) and another group of symptoms that appear at higher levels of intake (more than 1 g per day). Low-dose symptoms include
- restlessness,
- nervousness,
- excitement,
- insomnia,
- flushed face,
- diuresis (increased urination), and
- gastrointestinal disturbance.
Symptoms associated with high doses of caffeine include
- muscle twitching,
- rambling flow of thought and speech,
- tachycardia and cardiac arrhythmia,
- periods of inexhaustibility, and
- psychomotor agitation,[1]
- anorexia (loss of appetite).
The symptoms of caffeine intoxication are comparable to the symptoms of overdoses of other stimulants.[3] In cases of much larger overdoses, mania, depression, lapses in judgment, disorientation, disinhibition, delusions, weight loss, loss of appetite, hallucinations, or psychosis may occur.[8][9]
Death can occur when a person had a caffeine overdose.[10][11] The LD50 of caffeine in humans is dependent on individual sensitivity, but is estimated to be 150–200 milligrams per kilogram of body mass (75–100 cups of coffee for a 70 kilogram adult).[12] A number of fatalities have been caused by overdoses of readily available powdered caffeine supplements, for which the estimated lethal amount is less than a tablespoon.[13] The lethal dose is lower in individuals whose ability to metabolize caffeine is impaired due to genetics or chronic liver disease.[14] A death was reported in a man with liver cirrhosis who overdosed on caffeinated mints.[15][16][17] Caffeinism can also result in severe injury. In one case, energy drink caffeinism, led to a severe brain hemorrhage and massive loss of brain matter.[18]
Treatment
Treatment of mild caffeine intoxication is directed toward symptom relief; severe intoxication may require peritoneal dialysis, hemodialysis, or hemofiltration.[3] Control of caffeine intake requires awareness of the caffeine content of caffeinated beverages, over-the-counter drugs, and other sources of caffeine in the diet. Such information is not easy to obtain. The content of brewed beverages such as coffee and tea varies greatly based on the method of preparation.[19]
There is no standard value for "a cup of coffee." The caffeine content of cola drinks and most energy drinks can be difficult to determine, because in many cases the labels do not indicate the dose per serving. Caffeine doses in these beverages range from 20 to 30 mg in some soft drinks, up to 350 mg or more in some energy drinks. Although some Internet web sites report caffeine content for beverages, official lists are not available and the number of brands continually grows.[1]
Attempting to abruptly discontinue all consumption of caffeine-containing products from the diet is not usually recommended. The person could suffer from severe symptoms of caffeine withdrawal including headaches, fatigue, and difficulty concentrating. It is recommended that the person reduces caffeine consumption gradually to avoid withdrawal as attempts to suddenly discontinue all caffeine consumption are frequently abandoned due to the severity of the withdrawal symptoms.[1][19]
Epidemiology
Little is known about the prevalence of caffeinism in the general population. Although most people are familiar with the disorder, it probably remains underdiagnosed, because patients are rarely questioned about the use of caffeine.[2]
See also
References
- Stolerman, Ian P. (2010). Encyclopedia of Psychopharmacology (Online-Ausg. ed.). Berlin, Heidelberg: Springer-Verlag Berlin Heidelberg. pp. 261–264. ISBN 978-3-540-68706-1.
- Iancu, I; Strous, RD (February 2006). "Caffeine intoxication: history, clinical features, diagnosis and treatment". Harefuah. 145 (2): 147–51, 163–4. PMID 16509422.
- "Caffeine (Systemic)". MedlinePlus. 25 May 2000. Archived from the original on 23 February 2007. Retrieved 3 August 2009.
- Iancu I, Olmer A, Strous RD (2007). "Caffeinism: History, clinical features, diagnosis, and treatment". In Smith BD, Gupta U, Gupta BS (eds.). Caffeine and Activation Theory: Effects on Health and Behavior. CRC Press. pp. 331–344. ISBN 978-0-8493-7102-8. Retrieved 15 January 2014.
- Winston AP, Hardwick E, Jaberi N (2005). "Neuropsychiatric effects of caffeine". Advances in Psychiatric Treatment. 11 (6): 432–439. doi:10.1192/apt.11.6.432.
- "FoodData Central". ndb.nal.usda.gov. Retrieved 2020-10-02.
- American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental Disorders (4th ed.). American Psychiatric Association. ISBN 978-0-89042-062-1.
- "Caffeine overdose". MedlinePlus. 4 April 2006. Retrieved 3 August 2009.
- Verkhratsky A (January 2005). "Physiology and pathophysiology of the calcium store in the endoplasmic reticulum of neurons". Physiological Reviews. 85 (1): 201–79. doi:10.1152/physrev.00004.2004. PMID 15618481. S2CID 11820734.
- Holmgren P, Nordén-Pettersson L, Ahlner J (January 2004). "Caffeine fatalities – four case reports". Forensic Science International. 139 (1): 71–3. doi:10.1016/j.forsciint.2003.09.019. PMID 14687776.
- "FDA Consumer Advice on Powdered Pure Caffeine". FDA. Retrieved 20 August 2014.
- Peters JM (1967). "Factors Affecting Caffeine Toxicity: A Review of the Literature". The Journal of Clinical Pharmacology and the Journal of New Drugs. 7 (3): 131–141. doi:10.1002/j.1552-4604.1967.tb00034.x. Archived from the original on 12 January 2012.
- Murray Carpenter (18 May 2015). "Caffeine powder poses deadly risks". New York Times. Retrieved 18 May 2015.
- Rodopoulos N, Wisén O, Norman A (May 1995). "Caffeine metabolism in patients with chronic liver disease". Scandinavian Journal of Clinical and Laboratory Investigation. 55 (3): 229–42. doi:10.3109/00365519509089618. PMID 7638557.
- Cheston P, Smith L (11 October 2013). "Man died after overdosing on caffeine mints". The Independent. Retrieved 13 October 2013.
- Prynne M (11 October 2013). "Warning over caffeine sweets after father dies from overdose". The Telegraph. Archived from the original on 11 October 2013. Retrieved 13 October 2013.
- Fricker M (12 October 2013). "John Jackson: Family of dad who died from caffeine overdose after eating MINTS want them removed from sale". Daily Mirror. Retrieved 13 October 2013.
- "Woman Shares What Energy Drinks Did to Her Husband While She Was 9 Months Pregnant".
- Haenel, H. (1992). "J. E. James: Caffeine and Health. 432 Seiten. Academic Press, London, San Diego, New York u. a. Preis: 29,50 £; 59,95 $". Food/Nahrung. 36 (4): 431. doi:10.1002/food.19920360453.