Portal vein
The portal vein or hepatic portal vein (HPV) is a blood vessel that carries blood from the gastrointestinal tract, gallbladder, pancreas and spleen to the liver. This blood contains nutrients and toxins extracted from digested contents. Approximately 75% of total liver blood flow is through the portal vein, with the remainder coming from the hepatic artery proper. The blood leaves the liver to the heart in the hepatic veins.
| Portal vein | |
|---|---|
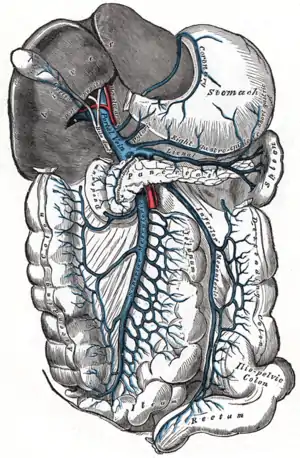 The portal vein and its tributaries. It is formed by the superior mesenteric vein, inferior mesenteric vein, and splenic vein. Lienal vein is an old term for splenic vein. | |
| Details | |
| System | Hepatic portal system |
| Drains from | Gastrointestinal tract, spleen, pancreas |
| Source | splenic vein, superior mesenteric vein, inferior mesenteric vein, pancreatic vein |
| Drains to | liver sinusoid |
| Identifiers | |
| Latin | vena portae hepatis |
| MeSH | D011169 |
| TA98 | A12.3.12.001 |
| TA2 | 5092 |
| FMA | 50735 |
| Anatomical terminology | |
The portal vein is not a true vein, because it conducts blood to capillary beds in the liver and not directly to the heart. It is a major component of the hepatic portal system, one of only two portal venous systems in the body – with the hypophyseal portal system being the other.
The portal vein is usually formed by the confluence of the superior mesenteric, splenic veins, inferior mesenteric, left, right gastric veins and the pancreatic vein.
Conditions involving the portal vein cause considerable illness and death. An important example of such a condition is elevated blood pressure in the portal vein. This condition, called portal hypertension, is a major complication of cirrhosis. In abdominal obesity fats, inflammatory cytokines and other toxic substances are transported by the portal vein from visceral fat into the liver, leading to hepatic insulin resistance and non-alcoholic fatty liver disease.[1][2]
Structure
Measuring approximately 8 cm (3 inches) long in adults,[3] the portal vein is located in the right upper quadrant of the abdomen, originating behind the neck of the pancreas.[4]
In most individuals, the portal vein is formed by the union of the superior mesenteric vein and the splenic vein.[5] For this reason, the portal vein is occasionally called the splenic-mesenteric confluence.[4] Occasionally, the portal vein also directly communicates with the inferior mesenteric vein, although this is highly variable. Other tributaries of the portal vein include the cystic and the left and right gastric veins.[6] and also pararumbilical vein and prepyloric vein.
Immediately before reaching the liver, the portal vein divides into right and left. It ramifies further, forming smaller venous branches and ultimately portal venules. Each portal venule courses alongside a hepatic arteriole and the two vessels form the vascular components of the portal triad. These vessels ultimately empty into the hepatic sinusoids to supply blood to the liver.[6]
Portacaval anastomoses
The portal venous system has several anastomoses with the systemic venous system. In cases of portal hypertension these anastomoses may become engorged, dilated, or varicosed and subsequently rupture.
Accessory hepatic portal veins
Accessory hepatic portal veins are those veins that drain directly into the liver without joining the hepatic portal vein. These include the paraumbilical veins as well as veins of the lesser omentum, falciform ligament, and those draining the gallbladder wall.[4]
Function
The portal vein and hepatic arteries form the liver's dual blood supply. Approximately 75% of hepatic blood flow is derived from the portal vein, while the remainder is from the hepatic arteries.[4]
Unlike most veins, the portal vein does not drain into the heart. Rather, it is part of a portal venous system that delivers venous blood into another capillary system, the hepatic sinusoids of the liver. In carrying venous blood from the gastrointestinal tract to the liver, the portal vein accomplishes two tasks: it supplies the liver with metabolic substrates and it ensures that substances ingested are first processed by the liver before reaching the systemic circulation. This accomplishes two things. First, possible toxins that may be ingested can be detoxified by the hepatocytes before they are released into the systemic circulation. Second, the liver is the first organ to absorb nutrients just taken in by the intestines. After draining into the liver sinusoids, blood from the liver is drained by the hepatic vein.
Clinical significance
Portal hypertension
Increased blood pressure in the portal vein, called portal hypertension, is a major complication of liver disease, most commonly cirrhosis.[7] A dilated portal vein (diameter of greater than 13 or 15 mm) is a sign of portal hypertension, with a sensitivity estimated at 12.5% or 40%.[8] On Doppler ultrasonography, the main portal vein (MPV) peak systolic velocity normally ranges between 20 cm/s and 40 cm/s.[9] A slow velocity of <16 cm/s in addition to dilatation in the MPV are diagnostic of portal hypertension.[9]
Clinical signs of portal hypertension include those of chronic liver disease: ascites, esophageal varices, spider nevi, caput medusae, and palmar erythema.[10]
Pulsatility

Portal vein pulsatility can be measured by Doppler ultrasonography. An increased pulsatility may be caused by cirrhosis, as well as increased right atrial pressure (which in turn may be caused by right heart failure or tricuspid regurgitation).[9] Portal vein pulsatility can be quantified by pulsatility indices (PI), where an index above a certain cutoff indicates pathology:
| Index | Calculation | Cutoff |
|---|---|---|
| Average-based | (Max - Min) / Average[9] | 0.5[9] |
| Max-based | (Max - Min) / Max[11] | 0.5[11][12] - 0.54[12] |
Infection
Pylephlebitis is infection of the portal vein, usually arising from an infectious intra-abdominal process such as diverticulitis.[13][14]
Portal venous gas
Hepatic portal venous gas is a rare finding on radiological exams. Gas is shown to enter the portal venous system. It is most commonly caused by intestinal ischemia but has also been associated with colon cancer.[15]
Additional images
 Human embryo with heart and anterior body-wall removed to show the sinus venosus and its tributaries
Human embryo with heart and anterior body-wall removed to show the sinus venosus and its tributaries Section across the portal triad of the pig
Section across the portal triad of the pig Longitudinal section of a small portal vein and canal
Longitudinal section of a small portal vein and canal Hepatic portal vein. Plastination technique.
Hepatic portal vein. Plastination technique. Hepatic portal vein. Abdominal cavity. Deep dissection.
Hepatic portal vein. Abdominal cavity. Deep dissection. Hepatic portal vein. Visceral surface of liver.
Hepatic portal vein. Visceral surface of liver.
References
- Item F, Konrad D (2012). "Visceral fat and metabolic inflammation: the portal theory revisited" (PDF). Obesity Reviews. 13 (Suppl 2): 30–39. doi:10.1111/j.1467-789X.2012.01035.x. PMID 23107257. S2CID 25169877.
- Dhawan D, Sharma S (2020). "Abdominal Obesity, Adipokines and Non-communicable Diseases". The Journal of Steroid Biochemistry and Molecular Biology. 203: 105737. doi:10.1016/j.jsbmb.2020.105737. PMC 7431389. PMID 32818561.
- Harold M Chung; Chung, Kyung Won (2008). Gross anatomy. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. pp. 208. ISBN 978-0-7817-7174-0.
- Plinio Rossi; L. Broglia (2000). Portal Hypertension: Diagnostic Imaging and Imaging-Guided Therapy. Berlin: Springer. p. 51. ISBN 978-3-540-65797-2.
- Benjamin L. Shneider; Sherman, Philip M. (2008). Pediatric Gastrointestinal Disease. Connecticut: PMPH-USA. p. 751. ISBN 978-1-55009-364-3.
- Henry Gray (1901). Anatomy, Descriptive and Surgical (16 ed.). Philadelphia: Lea Brothers. p. 619.
- Dooley, James; Sherlock, Sheila (2002). Diseases of the liver and biliary system. Oxford: Blackwell Science. ISBN 978-0-632-05582-1.
- Al-Nakshabandi NA (2006). "The role of ultrasonography in portal hypertension". Saudi J Gastroenterol. 12 (3): 111–7. doi:10.4103/1319-3767.29750. PMID 19858596.
- Iranpour, Pooya; Lall, Chandana; Houshyar, Roozbeh; Helmy, Mohammad; Yang, Albert; Choi, Joon-Il; Ward, Garrett; Goodwin, Scott C (2016). "Altered Doppler flow patterns in cirrhosis patients: an overview". Ultrasonography. 35 (1): 3–12. doi:10.14366/usg.15020. ISSN 2288-5919. PMC 4701371. PMID 26169079.
- Key Topics in General Surgery (2 ed.). Informa Healthcare. 2002. ISBN 978-1-85996-164-3.
- Goncalvesova, E.; Varga, I.; Tavacova, M.; Lesny, P. (2013). "Changes of portal vein flow in heart failure patients with liver congestion". European Heart Journal. 34 (suppl 1): P627. doi:10.1093/eurheartj/eht307.P627. ISSN 0195-668X.
- Page 367 in: Henryk Dancygier (2009). Clinical Hepatology: Principles and Practice of Hepatobiliary Diseases. Vol. 1. Springer Science & Business Media. ISBN 9783540938422.
- Plemmons RM, Dooley DP, Longfield RN (November 1995). "Septic thrombophlebitis of the portal vein (pylephlebitis): diagnosis and management in the modern era". Clin. Infect. Dis. 21 (5): 1114–20. doi:10.1093/clinids/21.5.1114. PMID 8589130.
- Perez-Cruet MJ, Grable E, Drapkin MS, Jablons DM, Cano G (May 1993). "Pylephlebitis associated with diverticulitis". South. Med. J. 86 (5): 578–80. doi:10.1097/00007611-199305000-00020. PMID 8488411.
- Li, Z; Su, Y; Wang, X; Yan, H; Sun, M; Shu, Z (December 2017). "Hepatic portal venous gas associated with colon cancer: A case report and literature review". Medicine. 96 (50): e9352. doi:10.1097/MD.0000000000009352. PMC 5815821. PMID 29390409.
External links
- Anatomy photo:38:12-0109 at the SUNY Downstate Medical Center - "Stomach, Spleen and Liver: The Visceral Surface of the Liver"
- Anatomy image:7959 at the SUNY Downstate Medical Center
- Anatomy image:8565 at the SUNY Downstate Medical Center
- Anatomy image:8697 at the SUNY Downstate Medical Center
- Cross section image: pembody/body8a—Plastination Laboratory at the Medical University of Vienna
- figures/chapter_30/30-2.HTM: Basic Human Anatomy at Dartmouth Medical School
{kind=link}
{kind=link}
{kind=link}