

Medical Screening of US-Bound Refugees
Burmese Refugee Health Profile
 ShareCompartir
ShareCompartir
Figure 7: Medical assessment of US-Bound Burmese Refugees
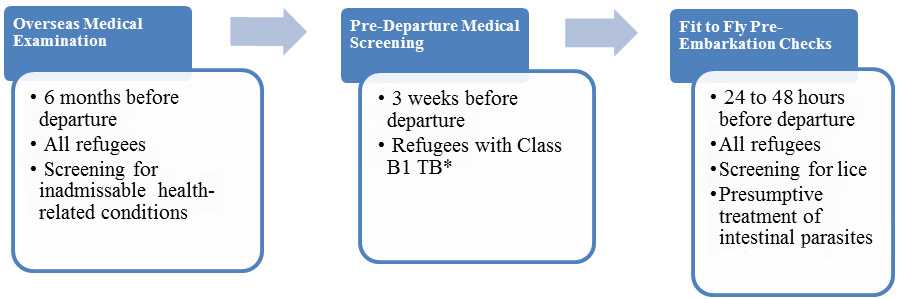
* Class B1 TB refers to TB fully treated by directly observed therapy (DOT), abnormal chest X-ray with negative sputum smears and cultures, or extrapulmonary TB.
Overseas Medical Examination
An overseas medical examination is mandatory for all refugees resettling to the United States and must be performed according to the CDC’s Technical Instructions for overseas medical examinations. The purpose of the overseas medical examination is to identify applicants with inadmissible health-related conditions. These examinations are performed by panel physicians who are selected by Department of State (DOS) Consular Officials. In some countries, the panel physicians are from the International Organization for Migration (IOM). CDC provides the regulatory and technical oversight and training for all panel physicians. Information collected during the refugee overseas medical examination is reported to CDC’s Electronic Disease Notification System (EDN) and is available to the state refugee health programs in the areas where the refugees are resettled.
Pre-Departure Medical Screening
For refugees previously diagnosed with Class B1 TB (TB fully treated using DOT, or abnormal chest X-ray with negative sputum smears and cultures, or extrapulmonary TB) a pre-departure medical screening is conducted about three weeks before departure for the United States. The screening includes a repeat physical examination, with a focus on TB signs and symptoms, chest X-ray, and sputum collection for acid fast bacilli (ADB) smear microscopy.
Pre-Embarkation Checks
For all departing refugees, IOM clinicians perform two pre-embarkation checks within 48 hours of the refugee’s departure to the United States to assess their health for travel and to administer presumptive therapy for intestinal parasites (worms).
Burmese refugees departing from Thailand and Malaysia receive pre-departure treatment for soil-transmitted helminthes (Ascaris, whipworm and hookworm), according to current CDC guidance . Except when contraindicated, soil-transmitted helminths are presumptively treated with a single dose of albendazole and Strongyloides with two consecutive days of ivermectin.
Information on presumptive therapy for intestinal parasites will be noted on IOM’s Pre-departure Medical Screening form included in the packet provided for each refugee during the pre-departure process. Information on presumptive therapy for intestinal parasites given to refugees will also appear in CDC’s EDN.
Post-Arrival Medical Screening
Once refugees have arrived in the United States, CDC recommends that they receive a post-arrival medical screening (domestic medical screening) within 30 days after arrival. The Department of Health and Human Services, Office of Refugee Resettlement (ORR) reimburses providers for screenings conducted during the first 90 days after arrival. The purpose of these more comprehensive examinations is to identify conditions that may not have been screened for during overseas medical examinations and to serve as an introduction to the U.S. healthcare system. CDC provides guidelines and recommendations, and state health departments oversee and administer the domestic medical screenings. State refugee health programs and panel physicians conduct the examinations themselves. Health departments determine who conducts the examinations within their jurisdiction. Data from the screenings are collected by most state health departments.
- Page last reviewed: June 6, 2016
- Page last updated: June 6, 2016
- Content source: