Asperger syndrome
| Asperger syndrome | |
|---|---|
| Other names: Asperger's syndrome, Asperger disorder (AD), Asperger's, schizoid disorder of childhood,[1] autistic psychopathy,[1] high-functioning autism,[2] level 1 autism spectrum disorder[3] | |
 | |
| Restricted interests or repetitive behaviors, such as this boy's interest in playing with a toy model of molecules, may be features of Asperger's. | |
| Pronunciation | |
| Specialty | Psychiatry |
| Symptoms | Problems with social interaction, non-verbal communication, restricted interests, repetitive behavior[6] |
| Complications | Social isolation, employment problems, family stress, bullying, self-harm[7] |
| Usual onset | Before two years old[6] |
| Duration | Long term[6] |
| Causes | Unknown[6] |
| Diagnostic method | Based on the symptoms[8] |
| Medication | For associated conditions[9] |
| Frequency | 37.2 million (2015)[10] |
Asperger syndrome (AS), also known as Asperger's, is a developmental disorder characterized by significant difficulties in social interaction and nonverbal communication, along with restricted and repetitive patterns of behavior and interests.[6] As a milder autism spectrum disorder (ASD), it differs from other ASDs by relatively normal language and intelligence.[11] Although not required for diagnosis, physical clumsiness and unusual use of language are common.[12][13] Signs usually begin before two years of age and typically last for a person's entire life.[6]
The exact cause of Asperger's is unknown.[6] While it is largely inherited, the underlying genetics have not been determined conclusively.[12][14] Environmental factors are also believed to play a role.[6] Brain imaging has not identified a common underlying condition.[12] In 2013, the diagnosis of Asperger's was removed from the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), and people with these symptoms are now included within the autism spectrum disorder along with autism and pervasive developmental disorder not otherwise specified (PDD-NOS).[6][15] It remains within the International Classification of Diseases (ICD-11) as of 2019 as a subtype of autism spectrum disorder.[16][17]
There is no single treatment, and the effectiveness of particular interventions is supported by only limited data.[12] Treatment is aimed at lowering obsessive or repetitive routines, and improving communication skills and physical clumsiness.[9] Interventions may include social skills training, cognitive behavioral therapy, physical therapy, speech therapy, parent training, and medications for associated problems, such as mood or anxiety.[9] Most children improve as they grow up, but social and communication difficulties usually persist.[18] Some researchers and people on the autism spectrum have advocated a shift in attitudes toward the view that autism spectrum disorder is a difference rather than a disease that must be treated or cured.[19][20]
In 2015, Asperger's was estimated to affect 37.2 million people globally.[10] Autism spectrum disorder affects males more often than females, and females are typically diagnosed at a later age.[21][22] The syndrome is named after the Austrian pediatrician Hans Asperger, who, in 1944, described children in his care who struggled to form friendships, did not understand others' gestures or feelings, engaged in one-sided conversations about their favorite interests, and were clumsy.[23] The modern conception of Asperger syndrome came into existence in 1981 and went through a period of popularization.[24][25][26] It became a standardized diagnosis in the early 1990s.[27] Many questions and controversies remain.[18] There is doubt about whether it is distinct from high-functioning autism (HFA).[28] Partly because of this, the percentage of people affected is not firmly established.[12]
Classification
The extent of the overlap between AS and high-functioning autism (HFA – autism unaccompanied by intellectual disability) is unclear.[28][29][30] The ASD classification is to some extent an artifact of how autism was discovered,[31] and may not reflect the true nature of the spectrum;[32] methodological problems have beset Asperger syndrome as a valid diagnosis from the outset.[33][34] In the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published in May 2013,[35] AS, as a separate diagnosis, was eliminated and folded into autism spectrum disorder.[36] Like the diagnosis of Asperger syndrome,[37] the change was controversial[37][38] and AS was not removed from the WHO's ICD-10 or ICD-11.[16][39]
The World Health Organization (WHO) defined Asperger syndrome (AS) as one of the autism spectrum disorders (ASD) or pervasive developmental disorders (PDD), which are a spectrum of psychological conditions that are characterized by abnormalities of social interaction and communication that pervade the individual's functioning, and by restricted and repetitive interests and behavior. Like other psychological development disorders, ASD begins in infancy or childhood, has a steady course without remission or relapse, and has impairments that result from maturation-related changes in various systems of the brain.[40] ASD, in turn, is a subset of the broader autism phenotype, which describes individuals who may not have ASD but do have autistic-like traits, such as social deficits.[41] Of the other four ASD forms, autism is the most similar to AS in signs and likely causes, but its diagnosis requires impaired communication and allows delay in cognitive development; Rett syndrome and childhood disintegrative disorder share several signs with autism but may have unrelated causes; and pervasive developmental disorder not otherwise specified (PDD-NOS) is diagnosed when the criteria for a more specific disorder are unmet.[42]
Characteristics

As a pervasive developmental disorder, Asperger syndrome is distinguished by a pattern of symptoms rather than a single symptom. It is characterized by qualitative impairment in social interaction, by stereotyped and restricted patterns of behavior, activities, and interests, and by no clinically significant delay in cognitive development or general delay in language.[43] Intense preoccupation with a narrow subject, one-sided verbosity, restricted prosody, and physical clumsiness are typical of the condition, but are not required for diagnosis.[28] Suicidal behavior appears to occur at rates similar to those without ASD.[44]
Social interaction
A lack of demonstrated empathy affects aspects of communal living for persons with Asperger syndrome.[13] Individuals with AS experience difficulties in basic elements of social interaction, which may include a failure to develop friendships or to seek shared enjoyments or achievements with others (for example, showing others objects of interest); a lack of social or emotional reciprocity (social "games" give-and-take mechanic); and impaired nonverbal behaviors in areas such as eye contact, facial expression, posture, and gesture.[12]
People with AS may not be as withdrawn around others, compared with those with other, more debilitating forms of autism; they approach others, even if awkwardly. For example, a person with AS may engage in a one-sided, long-winded speech about a favorite topic, while misunderstanding or not recognizing the listener's feelings or reactions, such as a wish to change the topic of talk or end the interaction.[28] This social awkwardness has been called "active but odd".[12] Such failures to react appropriately to social interaction may appear as disregard for other people's feelings and may come across as insensitive.[28] However, not all individuals with AS will approach others. Some of them may even display selective mutism, not speaking at all to most people and excessively to specific others. Some may choose only to talk to people they like.[45]
The cognitive ability of children with AS often allows them to articulate social norms in a laboratory context,[12] where they may be able to show a theoretical understanding of other people's emotions; however, they typically have difficulty acting on this knowledge in fluid, real-life situations.[28] People with AS may analyze and distill their observations of social interaction into rigid behavioral guidelines and apply these rules in awkward ways, such as forced eye contact, resulting in a demeanor that appears rigid or socially naïve. Childhood desire for companionship can become numbed through a history of failed social encounters.[12]
Violent or criminal behavior
The hypothesis that individuals with AS are predisposed to violent or criminal behavior has been investigated, but is not supported by data.[12][46] More evidence suggests that children diagnosed with Asperger syndrome are victims rather than offenders.[47]
A 2008 review found that an overwhelming number of reported violent criminals with Asperger syndrome also had other coexisting psychotic psychiatric disorders such as schizoaffective disorder.[48]
Restricted and repetitive interests and behavior
People with Asperger syndrome can display behavior, interests, and activities that are restricted and repetitive and are sometimes abnormally intense or focused. They may stick to inflexible routines, move in stereotyped and repetitive ways, preoccupy themselves with parts of objects, or engage in compulsive behaviors like lining objects up to form patterns.[43]
Pursuit of specific and narrow areas of interest is one of the most striking among possible features of AS.[12] Individuals with AS may collect volumes of detailed information on a relatively narrow topic such as weather data or star names without necessarily having a genuine understanding of the broader topic.[12][28] For example, a child might memorize camera model numbers while caring little about photography.[12] This behavior is usually apparent by age 5 or 6.[12] Although these special interests may change from time to time, they typically become more unusual and narrowly focused and often dominate social interaction so much that the entire family may become immersed. Because narrow topics often capture the interest of children, this symptom may go unrecognized.[28]
Stereotyped and repetitive motor behaviors are a core part of the diagnosis of AS and other ASDs.[49] They include hand movements such as flapping or twisting, and complex whole-body movements.[43] These are typically repeated in longer bursts and look more voluntary or ritualistic than tics, which are usually faster, less rhythmical, and less often symmetrical.[50] However, in addition to this, various studies have reported a consistent comorbidity between AS and Tourette syndrome in the range of 8–20%,[50][51][52][53] with one figure as high as 80% for tics of some kind or another,[53] for which several explanations have been put forward, including common genetic factors and dopamine, glutamate, or serotonin abnormalities.[54]
According to the Adult Asperger Assessment (AAA) diagnostic test, a lack of interest in fiction and a positive preference towards non-fiction is common among adults with AS.[55]
Speech and language
Although individuals with Asperger syndrome acquire language skills without significant general delay and their speech typically lacks significant abnormalities, language acquisition and use is often atypical.[28] Abnormalities include verbosity; abrupt transitions; literal interpretations and miscomprehension of nuance; use of metaphor meaningful only to the speaker; auditory perception deficits; unusually pedantic, formal, or idiosyncratic speech; and oddities in loudness, pitch, intonation, prosody, and rhythm.[12] Echolalia has also been observed in individuals with AS.[56]
Three aspects of communication patterns are of clinical interest: poor prosody, tangential and circumstantial speech, and marked verbosity. Although inflection and intonation may be less rigid or monotonic than in classic autism, people with AS often have a limited range of intonation: speech may be unusually fast, jerky, or loud. Speech may convey a sense of incoherence; the conversational style often includes monologues about topics that bore the listener, fails to provide context for comments, or fails to suppress internal thoughts. Individuals with AS may fail to detect whether the listener is interested or engaged in the conversation. The speaker's conclusion or point may never be made, and attempts by the listener to elaborate on the speech's content or logic, or to shift to related topics, are often unsuccessful.[28]
Children with AS may have a sophisticated vocabulary at a young age and such children have often been colloquially called "little professors", but have difficulty understanding figurative language and tend to use language literally.[12] Children with AS appear to have particular weaknesses in areas of nonliteral language that include humor, irony, teasing, and sarcasm. Although individuals with AS usually understand the cognitive basis of humor, they seem to lack understanding of the intent of humor to share enjoyment with others.[29] Despite strong evidence of impaired humor appreciation, anecdotal reports of humor in individuals with AS seem to challenge some psychological theories of AS and autism.[57]
Motor and sensory perception
Individuals with Asperger syndrome may have signs or symptoms that are independent of the diagnosis, but can affect the individual or the family.[58] These include differences in perception and problems with motor skills, sleep, and emotions.
Individuals with AS often have excellent auditory and visual perception.[59] Children with ASD often demonstrate enhanced perception of small changes in patterns such as arrangements of objects or well-known images; typically this is domain-specific and involves processing of fine-grained features.[60] Conversely, compared with individuals with high-functioning autism, individuals with AS have deficits in some tasks involving visual-spatial perception, auditory perception, or visual memory.[12] Many accounts of individuals with AS and ASD report other unusual sensory and perceptual skills and experiences. They may be unusually sensitive or insensitive to sound, light, and other stimuli;[61] these sensory responses are found in other developmental disorders and are not specific to AS or to ASD. There is little support for increased fight-or-flight response or failure of habituation in autism; there is more evidence of decreased responsiveness to sensory stimuli, although several studies show no differences.[62]
Hans Asperger's initial accounts[12] and other diagnostic schemes[63] include descriptions of physical clumsiness. Children with AS may be delayed in acquiring skills requiring dexterity, such as riding a bicycle or opening a jar, and may seem to move awkwardly or feel "uncomfortable in their own skin". They may be poorly coordinated or have an odd or bouncy gait or posture, poor handwriting, or problems with motor coordination.[12][28] They may show problems with proprioception (sensation of body position) on measures of developmental coordination disorder (motor planning disorder), balance, tandem gait, and finger-thumb apposition. There is no evidence that these motor skills problems differentiate AS from other high-functioning ASDs.[12]
Children with AS are more likely to have sleep problems, including difficulty in falling asleep, frequent nocturnal awakenings, and early morning awakenings.[64][65] AS is also associated with high levels of alexithymia, which is difficulty in identifying and describing one's emotions.[66] Although AS, lower sleep quality, and alexithymia are associated with each other, their causal relationship is unclear.[65]
Causes
Hans Asperger described common traits among his patients' family members, especially fathers, and research supports this observation and suggests a genetic contribution to Asperger syndrome. Although no specific genetic factor has yet been identified, multiple factors are believed to play a role in the expression of autism, given the variability in symptoms seen in children.[12][67] Evidence for a genetic link is that AS tends to run in families where more family members have limited behavioral symptoms similar to AS (for example, some problems with social interaction, or with language and reading skills).[9] Most behavioral genetic research suggests that all autism spectrum disorders have shared genetic mechanisms, but AS may have a stronger genetic component than autism.[12] There may be shared genes in which particular alleles make an individual vulnerable, and varying combinations result in differing severity and symptoms in each person with AS.[9]
A few ASD cases have been linked to exposure to teratogens (agents that cause birth defects) during the first eight weeks from conception. Although this does not exclude the possibility that ASD can be initiated or affected later, it is strong evidence that ASD arises very early in development.[68] Many environmental factors have been hypothesized to act after birth, but none has been confirmed by scientific investigation.[69]
Mechanism
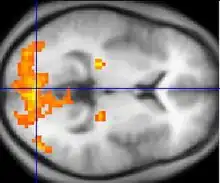
Asperger syndrome appears to result from developmental factors that affect many or all functional brain systems, as opposed to localized effects.[72] Although the specific underpinnings of AS or factors that distinguish it from other ASDs are unknown, and no clear pathology common to individuals with AS has emerged,[12] it is still possible that AS's mechanism is separate from other ASDs.[73] Neuroanatomical studies and the associations with teratogens strongly suggest that the mechanism includes alteration of brain development soon after conception.[68] Abnormal fetal development may affect the final structure and connectivity of the brain, resulting in altered neural circuits controlling thought and behavior.[74] Several theories of mechanism are available; none are likely to provide a complete explanation.[75]
The underconnectivity theory hypothesizes underfunctioning high-level neural connections and synchronization, along with an excess of low-level processes.[70] It maps well to general-processing theories such as weak central coherence theory, which hypothesizes that a limited ability to see the big picture underlies the central disturbance in ASD.[76] A related theory—enhanced perceptual functioning—focuses more on the superiority of locally oriented and perceptual operations in autistic individuals.[77]
The mirror neuron system (MNS) theory hypothesizes that alterations to the development of the MNS interfere with imitation and lead to Asperger's core feature of social impairment.[71][78] One study found that activation is delayed in the core circuit for imitation in individuals with AS.[79] This theory maps well to social cognition theories like the theory of mind, which hypothesizes that autistic behavior arises from impairments in ascribing mental states to oneself and others;[80] or hyper-systemizing, which hypothesizes that autistic individuals can systematize internal operation to handle internal events but are less effective at empathizing when handling events generated by other agents.[81]
Changes in brain neurotransmitter activity have been found. There is increased dopaminergic activity, whereas there is reduced serotonin due to reduced tryptophan.[82]
Diagnosis
Standard diagnostic criteria require impairment in social interaction and repetitive and stereotyped patterns of behavior, activities, and interests, without significant delay in language or cognitive development. Unlike the international standard,[40] the DSM-IV-TR criteria also required significant impairment in day-to-day functioning;[43] DSM-5 eliminated AS as a separate diagnosis in 2013, and folded it into the umbrella of autism spectrum disorders.[36] Other sets of diagnostic criteria have been proposed by Szatmari et al.[83] and by Gillberg and Gillberg.[84]
Diagnosis is most commonly made between the ages of four and eleven.[12] A comprehensive assessment involves a multidisciplinary team[9][13][85] that observes across multiple settings,[12] and includes neurological and genetic assessment as well as tests for cognition, psychomotor function, verbal and nonverbal strengths and weaknesses, style of learning, and skills for independent living.[9] The "gold standard" in diagnosing ASDs combines clinical judgment with the Autism Diagnostic Interview-Revised (ADI-R), a semistructured parent interview; and the Autism Diagnostic Observation Schedule (ADOS), a conversation and play-based interview with the child.[18] Delayed or mistaken diagnosis can be traumatic for individuals and families; for example, misdiagnosis can lead to medications that worsen behavior.[85][86]
Underdiagnosis and overdiagnosis may be problems. The cost and difficulty of screening and assessment can delay diagnosis. Conversely, the increasing popularity of drug treatment options and the expansion of benefits has motivated providers to overdiagnose ASD.[87] There are indications AS has been diagnosed more frequently in recent years, partly as a residual diagnosis for children of normal intelligence who are not autistic but have social difficulties.[88]
There are questions about the external validity of the AS diagnosis. That is, it is unclear whether there is a practical benefit in distinguishing AS from HFA and from PDD-NOS;[88] different screening tools render different diagnoses depending in the same child.[9]
Differential diagnosis
Many children with AS are initially misdiagnosed with attention deficit hyperactivity disorder (ADHD).[12] Diagnosing adults is more challenging, as standard diagnostic criteria are designed for children and the expression of AS changes with age.[89][90] Adult diagnosis requires painstaking clinical examination and thorough medical history gained from both the individual and other people who know the person, focusing on childhood behavior.[55]
Conditions that must be considered in a differential diagnosis along with ADHD include other ASDs, the schizophrenia spectrum, personality disorders, obsessive–compulsive disorder, major depressive disorder, semantic pragmatic disorder, nonverbal learning disorder, social anxiety disorder,[85][89] Tourette syndrome,[50] stereotypic movement disorder, bipolar disorder,[67] social-cognitive deficits due to brain damage from alcohol abuse,[91] and obsessive–compulsive personality disorder (OCPD).[53][92]
Screening
Parents of children with Asperger syndrome can typically trace differences in their children's development to as early as 30 months of age.[67] Developmental screening during a routine check-up by a general practitioner or pediatrician may identify signs that warrant further investigation.[9][12] The United States Preventive Services Task Force in 2016 found it was unclear if screening was beneficial or harmful among children in whom there are no concerns.[93]
Different screening instruments are used to diagnose AS,[9][63] including the Asperger Syndrome Diagnostic Scale (ASDS); Autism Spectrum Screening Questionnaire (ASSQ); Childhood Autism Spectrum Test (CAST), previously called the Childhood Asperger Syndrome Test;[94] Gilliam Asperger's disorder scale (GADS); Krug Asperger's Disorder Index (KADI);[95] and the autism-spectrum quotient (AQ), with versions for children,[96] adolescents,[97] and adults.[98] None have been shown to reliably differentiate between AS and other ASDs.[12]
Management
Asperger syndrome treatment attempts to manage distressing symptoms and to teach age-appropriate social, communication, and vocational skills that are not naturally acquired during development,[12] with intervention tailored to the needs of the individual based on multidisciplinary assessment.[99] Although progress has been made, data supporting the efficacy of particular interventions are limited.[12][100]
Therapies
Managing AS ideally involves multiple therapies that address core symptoms of the disorder. While most professionals agree that the earlier the intervention, the better, there is no treatment combination that is recommended above others.[9] AS treatment resembles that of other high-functioning ASDs, except that it takes into account the linguistic capabilities, verbal strengths, and nonverbal vulnerabilities of individuals with AS.[12] A typical program generally includes:[9]
- Applied behavior analysis (ABA) procedures, including positive behavior support (PBS)—or training and support of parents and school faculty in behavior management strategies to use in the home and school, and social skills training for more effective interpersonal interactions;[101]
- Cognitive behavioral therapy to improve stress management relating to anxiety or explosive emotions[102] and to help reduce obsessive interests and repetitive routines;
- Medication for coexisting conditions such as major depressive disorder and anxiety disorders;[103]
- Occupational or physical therapy to assist with poor sensory processing and motor coordination; and,
- Social communication intervention, which is specialized speech therapy to help with the pragmatics and give-and-take of normal conversation.[104]
Of the many studies on behavior-based early intervention programs, most are case reports of up to five participants and typically examine a few problem behaviors such as self-injury, aggression, noncompliance, stereotypies, or spontaneous language; unintended side effects are largely ignored.[105] Despite the popularity of social skills training, its effectiveness is not firmly established.[106] A randomized controlled study of a model for training parents in problem behaviors in their children with AS showed that parents attending a one-day workshop or six individual lessons reported fewer behavioral problems, while parents receiving the individual lessons reported less intense behavioral problems in their AS children.[107] Vocational training is important to teach job interview etiquette and workplace behavior to older children and adults with AS, and organization software and personal data assistants can improve the work and life management of people with AS.[12]
Medications
No medications directly treat the core symptoms of AS.[103] Although research into the efficacy of pharmaceutical intervention for AS is limited,[12] it is essential to diagnose and treat comorbid conditions.[13] Deficits in self-identifying emotions or in observing effects of one's behavior on others can make it difficult for individuals with AS to see why medication may be appropriate.[103] Medication can be effective in combination with behavioral interventions and environmental accommodations in treating comorbid symptoms such as anxiety disorders, major depressive disorder, inattention, and aggression.[12] The atypical antipsychotic medications risperidone, olanzapine and aripiprazole have been shown to reduce the associated symptoms of AS;[12][108][109] risperidone can reduce repetitive and self-injurious behaviors, aggressive outbursts, and impulsivity, and improve stereotypical patterns of behavior and social relatedness. The selective serotonin reuptake inhibitors (SSRIs) fluoxetine, fluvoxamine, and sertraline have been effective in treating restricted and repetitive interests and behaviors,[12][13][67] while stimulant medication, such as methylphenidate, can reduce inattention.[110]
Care must be taken with medications, as side effects may be more common and harder to evaluate in individuals with AS, and tests of drugs' effectiveness against comorbid conditions routinely exclude individuals from the autism spectrum.[103] Abnormalities in metabolism, cardiac conduction times, and an increased risk of type 2 diabetes have been raised as concerns with antipsychotic medications,[111][112] along with serious long-term neurological side effects.[105] SSRIs can lead to manifestations of behavioral activation such as increased impulsivity, aggression, and sleep disturbance.[67] Weight gain and fatigue are commonly reported side effects of risperidone, which may also lead to increased risk for extrapyramidal symptoms such as restlessness and dystonia[67] and increased serum prolactin levels.[113] Sedation and weight gain are more common with olanzapine,[112] which has also been linked with diabetes.[111] Sedative side-effects in school-age children[114] have ramifications for classroom learning. Individuals with AS may be unable to identify and communicate their internal moods and emotions or to tolerate side effects that for most people would not be problematic.[115]
Prognosis
There is some evidence that children with AS may see a lessening of symptoms; up to 20% of children may no longer meet the diagnostic criteria as adults, although social and communication difficulties may persist.[18] As of 2006, no studies addressing the long-term outcome of individuals with Asperger syndrome are available and there are no systematic long-term follow-up studies of children with AS.[28] Individuals with AS appear to have normal life expectancy, but have an increased prevalence of comorbid psychiatric conditions, such as major depressive disorder and anxiety disorders that may significantly affect prognosis.[12][18] Although social impairment may be lifelong, the outcome is generally more positive than with individuals with lower-functioning autism spectrum disorders;[12] for example, ASD symptoms are more likely to diminish with time in children with AS or HFA.[116] Most students with AS and HFA have average mathematical ability and test slightly worse in mathematics than in general intelligence, but some are gifted in mathematics.[117]
Although many attend regular education classes, some children with AS may utilize special education services because of their social and behavioral difficulties.[28] Adolescents with AS may exhibit ongoing difficulty with self-care or organization, and disturbances in social and romantic relationships. Despite high cognitive potential, most young adults with AS remain at home, yet some do marry and work independently.[12] The "different-ness" adolescents experience can be traumatic.[118] Anxiety may stem from preoccupation over possible violations of routines and rituals, from being placed in a situation without a clear schedule or expectations, or from concern with failing in social encounters;[12] the resulting stress may manifest as inattention, withdrawal, reliance on obsessions, hyperactivity, or aggressive or oppositional behavior.[102] Depression is often the result of chronic frustration from repeated failure to engage others socially, and mood disorders requiring treatment may develop.[12] Clinical experience suggests the rate of suicide may be higher among those with AS, but this has not been confirmed by systematic empirical studies.[119]
Education of families is critical in developing strategies for understanding strengths and weaknesses;[13] helping the family to cope improves outcomes in children.[47] Prognosis may be improved by diagnosis at a younger age that allows for early interventions, while interventions in adulthood are valuable but less beneficial.[13] There are legal implications for individuals with AS as they run the risk of exploitation by others and may be unable to comprehend the societal implications of their actions.[13]
Epidemiology
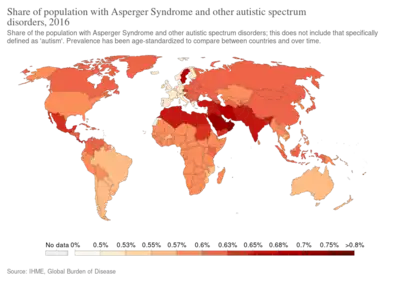
Frequency estimates vary. In 2015, it was estimated that 37.2 million people globally are affected.[10] A 2003 review of epidemiological studies of children found autism rates ranging from 0.03 to 4.84 per 1,000, with the ratio of autism to Asperger syndrome ranging from 1.5:1 to 16:1;[120] combining the geometric mean ratio of 5:1 with a conservative prevalence estimate for autism of 1.3 per 1,000 suggests indirectly that the prevalence of AS might be around 0.26 per 1,000.[121] Part of the variance in estimates arises from differences in diagnostic criteria. For example, a relatively small 2007 study of 5,484 eight-year-old children in Finland found 2.9 children per 1,000 met the ICD-10 criteria for an AS diagnosis, 2.7 per 1,000 for Gillberg and Gillberg criteria, 2.5 for DSM-IV, 1.6 for Szatmari et al., and 4.3 per 1,000 for the union of the four criteria. Boys seem to be more likely to have AS than girls; estimates of the sex ratio range from 1.6:1 to 4:1, using the Gillberg and Gillberg criteria.[122] Females with autism spectrum disorders may be underdiagnosed.[123]
Anxiety disorders and major depressive disorder are the most common conditions seen at the same time; comorbidity of these in persons with AS is estimated at 65%.[12] Reports have associated AS with medical conditions such as aminoaciduria and ligamentous laxity, but these have been case reports or small studies and no factors have been associated with AS across studies.[12] One study of males with AS found an increased rate of epilepsy and a high rate (51%) of nonverbal learning disorder.[124] AS is associated with tics, Tourette syndrome and bipolar disorder. The repetitive behaviors of AS have many similarities with the symptoms of obsessive–compulsive disorder and obsessive–compulsive personality disorder,[53] and 26% of a sample of young adults with AS were found to meet the criteria for schizoid personality disorder (which is characterised by severe social seclusion and emotional detachment), more than any other personality disorder in the sample.[125][126][127] However many of these studies are based on clinical samples or lack standardized measures; nonetheless, comorbid conditions are relatively common.[18]
History
Named after the Austrian pediatrician Hans Asperger (1906–1980), Asperger syndrome is a relatively new diagnosis in the field of autism,[128] though a syndrome like it was described as early as 1925 by Grunya Sukhareva (1891–1981).[129] As a child, Asperger appears to have exhibited some features of the very condition named after him, such as remoteness and talent in language.[130][131] In 1944, Asperger described four children in his practice[13] who had difficulty in integrating themselves socially and showing empathy towards peers. They also lacked nonverbal communication skills and were physically clumsy. Asperger described this "autistic psychopathy" as social isolation.[9] Fifty years later, several standardizations of AS as a medical diagnosis were tentatively proposed, many of which diverge significantly from Asperger's original work.[132]
Unlike today's AS, autistic psychopathy could be found in people of all levels of intelligence, including those with intellectual disability.[133] Asperger defended the value of high-functioning autistic individuals, writing: "We are convinced, then, that autistic people have their place in the organism of the social community. They fulfill their role well, perhaps better than anyone else could, and we are talking of people who as children had the greatest difficulties and caused untold worries to their care-givers."[23] Asperger also believed some would be capable of exceptional achievement and original thought later in life.[13]
Asperger's paper was published during World War II and in German, so it was not widely read elsewhere. Lorna Wing used the term Asperger syndrome in 1976,[134] and popularized it to the English-speaking medical community in her February 1981 publication[135][136][137] of case studies of children showing the symptoms described by Asperger,[128] and Uta Frith translated his paper to English in 1991.[23] Sets of diagnostic criteria were outlined by Gillberg and Gillberg in 1989 and by Szatmari et al. in the same year.[122] In 1992, AS became a standard diagnosis when it was included in the tenth edition of the World Health Organization's diagnostic manual, International Classification of Diseases (ICD-10). It was added to the fourth edition of the American Psychiatric Association's diagnostic reference, Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), published in 1994.[9]
Hundreds of books, articles and websites now describe AS and prevalence estimates have increased dramatically for ASD, with AS recognized as an important subgroup.[128] Whether it should be seen as distinct from high-functioning autism is a fundamental issue requiring further study,[13] and there are questions about the empirical validation of the DSM-IV and ICD-10 criteria.[28] In 2013, DSM-5 eliminated AS as a separate diagnosis, folding it into the autism spectrum on a severity scale.[36]
Society and culture

People identifying with Asperger syndrome may refer to themselves in casual conversation as aspies (a term first used in print by Liane Holliday Willey in 1999).[138] Some autistic people have advocated a shift in perception of autism spectrum disorders as complex syndromes rather than diseases that must be cured. Proponents of this view reject the notion that there is an "ideal" brain configuration and that any deviation from the norm is pathological; they promote tolerance for what they call neurodiversity.[139] These views are the basis for the autistic rights and autistic pride movements.[140] There is a contrast between the attitude of adults with self-identified AS, who typically do not want to be cured and are proud of their identity; and parents of children with AS, who typically seek assistance and a cure for their children.[141]
Some researchers have argued that AS can be viewed as a different cognitive style, not a disorder,[19] and that it should be removed from the standard Diagnostic and Statistical Manual, much as homosexuality was removed.[142] In a 2002 paper, Simon Baron-Cohen wrote of those with AS: "In the social world, there is no great benefit to a precise eye for detail, but in the worlds of maths, computing, cataloging, music, linguistics, engineering, and science, such an eye for detail can lead to success rather than failure." Baron-Cohen cited two reasons why it might still be useful to consider AS to be a disability: to ensure provision for legally required special support, and to recognize emotional difficulties from reduced empathy.[20] Baron-Cohen argues that the genes for Asperger's combination of abilities have operated throughout recent human evolution and have made remarkable contributions to human history.[143]
By contrast, Pier Jaarsma and Welin wrote in 2011 that the "broad version of the neurodiversity claim, covering low-functioning as well as high-functioning autism, is problematic. Only a narrow conception of neurodiversity, referring exclusively to high-functioning autists, is reasonable."[144] They say that "higher functioning" individuals with autism may "not [be] benefited with such a psychiatric defect-based diagnosis [...] some of them are being harmed by it, because of the disrespect the diagnosis displays for their natural way of being", but "think that it is still reasonable to include other categories of autism in the psychiatric diagnostics. The narrow conception of the neurodiversity claim should be accepted but the broader claim should not."[144] Jonathan Mitchell, an autistic author and blogger who advocates a cure for autism, has described autism as having "prevented me from making a living or ever having a girlfriend. It's given me bad fine motor coordination problems where I can hardly write. I have an impaired ability to relate to people. I can't concentrate or get things done."[145] He describes neurodiversity as a "tempting escape valve".[146]
References
- 1 2 World Health Organization (2016). "International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10): F84.5 Asperger syndrome". Archived from the original on 8 February 2017. Retrieved 2 November 2018.
- ↑ Shiland, Betsy J. (2014). Medical Terminology & Anatomy for ICD-10 Coding (E-book). Elsevier Health Sciences. p. 518. ISBN 9780323290784. Archived from the original on 14 April 2021. Retrieved 6 August 2020.
- ↑ "Neurodevelopmental Disorders". Diagnostic and Statistical Manual of Mental Disorders (5 ed.). American Psychiatric Association. 18 May 2013. pp. 50–59. ISBN 978-0-89042-554-1.
- ↑ "Asperger syndrome definition and meaning | Collins English Dictionary". www.collinsdictionary.com. Archived from the original on 12 May 2018. Retrieved 16 May 2018.
- ↑ "Asperger's syndrome". Oxford Dictionaries. Archived from the original on 3 October 2016. Retrieved 16 May 2018.
- 1 2 3 4 5 6 7 8 9 "Autism Spectrum Disorder". National Institute of Mental Health. September 2015. Archived from the original on 12 March 2016. Retrieved 12 March 2016.
- ↑ "Autism spectrum disorder - Symptoms and causes". Mayo Clinic. Archived from the original on 14 July 2019. Retrieved 13 July 2019.
- ↑ "Autism Spectrum Disorders – Pediatrics". Merck Manuals Professional Edition. Archived from the original on 26 January 2019. Retrieved 26 January 2019.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 National Institute of Neurological Disorders and Stroke (NINDS) (31 July 2007). "Asperger syndrome fact sheet". Archived from the original on 21 August 2007. Retrieved 24 August 2007. NIH Publication No. 05-5624.
- 1 2 3 Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, et al. (GBD 2015 Disease and Injury Incidence and Prevalence Collaborators) (October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
- ↑ "F84.5 Asperger syndrome". World Health Organization. 2015. Archived from the original on 2 November 2015. Retrieved 13 March 2016.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 McPartland J, Klin A (October 2006). "Asperger's syndrome". Adolescent Medicine Clinics. 17 (3): 771–88, abstract xiii. doi:10.1016/j.admecli.2006.06.010 (inactive 4 June 2020). PMID 17030291.
{{cite journal}}: CS1 maint: DOI inactive as of June 2020 (link) - 1 2 3 4 5 6 7 8 9 10 11 Baskin JH, Sperber M, Price BH (2006). "Asperger syndrome revisited". Reviews in Neurological Diseases. 3 (1): 1–7. PMID 16596080.
- ↑ Klauck SM (June 2006). "Genetics of autism spectrum disorder". European Journal of Human Genetics. 14 (6): 714–20. doi:10.1038/sj.ejhg.5201610. PMID 16721407.
- ↑ "Autism Spectrum Disorder". National Institute of Mental Health. Archived from the original on 9 March 2016. Retrieved 12 March 2016.
- 1 2 "Asperger syndrome". Genetic and Rare Diseases Information Center (GARD) – an NCATS Program. Archived from the original on 14 October 2019. Retrieved 26 January 2019.
- ↑ "ICD-11". icd.who.int. Archived from the original on 19 November 2019. Retrieved 12 February 2019.
- 1 2 3 4 5 6 Woodbury-Smith MR, Volkmar FR (January 2009). "Asperger syndrome". European Child & Adolescent Psychiatry (Submitted manuscript). 18 (1): 2–11. doi:10.1007/s00787-008-0701-0. PMID 18563474. Archived from the original on 31 March 2019. Retrieved 6 August 2020.
- 1 2 Clarke J, van Amerom G (2007). "'Surplus suffering': differences between organizational understandings of Asperger's syndrome and those people who claim the 'disorder'". Disability & Society. 22 (7): 761–76. doi:10.1080/09687590701659618.
- 1 2 Baron-Cohen S (2002). "Is Asperger syndrome necessarily viewed as a disability?". Focus Autism Other Dev Disabl. 17 (3): 186–91. doi:10.1177/10883576020170030801. A preliminary, freely readable draft, with slightly different wording in the quoted text, is in: Baron-Cohen S (2002). "Is Asperger's syndrome necessarily a disability?" (PDF). Cambridge: Autism Research Centre. Archived from the original (PDF) on 17 December 2008. Retrieved 2 December 2008.
- ↑ Ferri, Fred F. (2014). Ferri's Clinical Advisor 2015 (E-Book). Elsevier Health Sciences. p. 162. ISBN 9780323084307. Archived from the original on 14 April 2021. Retrieved 6 August 2020.
- ↑ Lai MC, Baron-Cohen S (November 2015). "Identifying the lost generation of adults with autism spectrum conditions". The Lancet. Psychiatry. 2 (11): 1013–27. doi:10.1016/S2215-0366(15)00277-1. PMID 26544750.
- 1 2 3 Frith, Uta (1991). "'Autistic psychopathy' in childhood". Autism and Asperger Syndrome. Cambridge: Cambridge University Press. pp. 37–92. ISBN 978-0-521-38608-1.
- ↑ Klin A, Pauls D, Schultz R, Volkmar F (April 2005). "Three diagnostic approaches to Asperger syndrome: implications for research". Journal of Autism and Developmental Disorders. 35 (2): 221–34. doi:10.1007/s10803-004-2001-y. PMID 15909408. S2CID 19076633.
- ↑ Wing L (1998). "The history of Asperger syndrome". In Schopler E, Mesibov GB, Kunce LJ (eds.). Asperger syndrome or high-functioning autism?. New York: Plenum press. pp. 11–25. ISBN 978-0-306-45746-3. Archived from the original on 13 March 2016.
- ↑ Woodbury-Smith M, Klin A, Volkmar F (April 2005). "Asperger's syndrome: a comparison of clinical diagnoses and those made according to the ICD-10 and DSM-IV". Journal of Autism and Developmental Disorders. 35 (2): 235–40. doi:10.1007/s10803-004-2002-x. PMID 15909409. S2CID 12417580.
- ↑ Baker, Linda (2004). Asperger's Syndrome: Intervening in Schools, Clinics, and Communities. Routledge. p. 44. ISBN 978-1-135-62414-9. Archived from the original on 13 March 2016.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Klin A (May 2006). "[Autism and Asperger syndrome: an overview]". Revista Brasileira de Psiquiatria. 28 Suppl 1 (suppl 1): S3–11. doi:10.1590/S1516-44462006000500002. PMID 16791390. S2CID 34035031.
- 1 2 Kasari C, Rotheram-Fuller E (September 2005). "Current trends in psychological research on children with high-functioning autism and Asperger disorder". Current Opinion in Psychiatry. 18 (5): 497–501. doi:10.1097/01.yco.0000179486.47144.61. PMID 16639107.
- ↑ Witwer AN, Lecavalier L (October 2008). "Examining the validity of autism spectrum disorder subtypes". Journal of Autism and Developmental Disorders. 38 (9): 1611–24. doi:10.1007/s10803-008-0541-2. PMID 18327636. S2CID 5316399.
- ↑ Sanders JL (November 2009). "Qualitative or quantitative differences between Asperger's disorder and autism? Historical considerations". Journal of Autism and Developmental Disorders. 39 (11): 1560–67. doi:10.1007/s10803-009-0798-0. PMID 19548078. S2CID 26351778.
- ↑ Szatmari P (October 2000). "The classification of autism, Asperger's syndrome, and pervasive developmental disorder". Canadian Journal of Psychiatry. 45 (8): 731–38. doi:10.1177/070674370004500806. PMID 11086556.
- ↑ Matson JL, Minshawi NF (2006). "History and development of autism spectrum disorders". Early intervention for autism spectrum disorders: a critical analysis. Amsterdam: Elsevier Science. p. 21. ISBN 978-0-08-044675-2. Archived from the original on 27 August 2021. Retrieved 6 August 2020.
- ↑ Schopler E (1998). "Premature popularization of Asperger syndrome". In Schopler E, Mesibov GB, Kunce LJ (eds.). Asperger syndrome or high-functioning autism?. New York: Plenum press. pp. 388–90. ISBN 978-0-306-45746-3. Archived from the original on 24 February 2021. Retrieved 6 August 2020.
- ↑ "DSM-5 development". American Psychiatric Association. 2010. Archived from the original on 13 February 2010. Retrieved 20 February 2010.
- 1 2 3 "299.80 Asperger's Disorder". DSM-5 Development. American Psychiatric Association. Archived from the original on 25 December 2010. Retrieved 21 December 2010.
- 1 2 Ghaziuddin M (September 2010). "Should the DSM V drop Asperger syndrome?". Journal of Autism and Developmental Disorders. 40 (9): 1146–48. doi:10.1007/s10803-010-0969-z. PMID 20151184. S2CID 7490308.
- ↑ Faras H, Al Ateeqi N, Tidmarsh L (2010). "Autism spectrum disorders". Annals of Saudi Medicine. 30 (4): 295–300. doi:10.4103/0256-4947.65261. PMC 2931781. PMID 20622347.
- ↑ "ICD-10 Version:2016". apps.who.int. Archived from the original on 8 February 2017. Retrieved 6 November 2018.
- 1 2 World Health Organization (2006). "F84. Pervasive developmental disorders". International Statistical Classification of Diseases and Related Health Problems (10th (ICD-10) ed.). ISBN 978-92-4-154419-1. Archived from the original on 28 June 2009. Retrieved 6 August 2020.
- ↑ Piven J, Palmer P, Jacobi D, Childress D, Arndt S (February 1997). "Broader autism phenotype: evidence from a family history study of multiple-incidence autism families". The American Journal of Psychiatry. 154 (2): 185–90. doi:10.1176/ajp.154.2.185. PMID 9016266. S2CID 14403967.
- ↑ Lord C, Cook EH, Leventhal BL, Amaral DG (November 2000). "Autism spectrum disorders". Neuron. 28 (2): 355–63. doi:10.1016/S0896-6273(00)00115-X. PMID 11144346.
- 1 2 3 4 American Psychiatric Association (2000). "Diagnostic criteria for 299.80 Asperger's Disorder (AD)". Diagnostic and Statistical Manual of Mental Disorders (4th, text revision (DSM-IV-TR) ed.). ISBN 978-0-89042-025-6. Archived from the original on 7 June 2007. Retrieved 6 August 2020.
- ↑ Hannon G, Taylor EP (December 2013). "Suicidal behaviour in adolescents and young adults with ASD: findings from a systematic review" (PDF). Clinical Psychology Review. 33 (8): 1197–204. doi:10.1016/j.cpr.2013.10.003. PMID 24201088. Archived (PDF) from the original on 9 March 2021. Retrieved 6 August 2020.
- ↑ Brasic JR (7 July 2010). "Asperger's Syndrome". Medscape eMedicine. Archived from the original on 23 December 2010. Retrieved 25 November 2010.
- ↑ Allen D, Evans C, Hider A, Hawkins S, Peckett H, Morgan H (April 2008). "Offending behaviour in adults with Asperger syndrome". Journal of Autism and Developmental Disorders. 38 (4): 748–58. doi:10.1007/s10803-007-0442-9. PMID 17805955. S2CID 12999370.
- 1 2 Tsatsanis KD (January 2003). "Outcome research in Asperger syndrome and autism". Child and Adolescent Psychiatric Clinics of North America. 12 (1): 47–63, vi. doi:10.1016/S1056-4993(02)00056-1. PMID 12512398.
- ↑ Newman SS, Ghaziuddin M (November 2008). "Violent crime in Asperger syndrome: the role of psychiatric comorbidity". Journal of Autism and Developmental Disorders. 38 (10): 1848–52. doi:10.1007/s10803-008-0580-8. PMID 18449633. S2CID 207158193.
- ↑ South M, Ozonoff S, McMahon WM (April 2005). "Repetitive behavior profiles in Asperger syndrome and high-functioning autism". Journal of Autism and Developmental Disorders. 35 (2): 145–58. doi:10.1007/s10803-004-1992-8. PMID 15909401. S2CID 36078197.
- 1 2 3 Rapin I (2001). "Autism spectrum disorders: relevance to Tourette syndrome". Advances in Neurology. 85: 89–101. PMID 11530449.
- ↑ Steyaert JG, De la Marche W (2008). "What's new in autism?". Eur J Pediatr. 167 (10): 1091–101. doi:10.1007/s00431-008-0764-4. PMID 18597114. Archived from the original on 17 October 2019. Retrieved 6 August 2020.
- ↑ Mazzone L, Ruta L, Reale L (June 2012). "Psychiatric comorbidities in asperger syndrome and high functioning autism: diagnostic challenges". Annals of General Psychiatry. 11 (1): 16. doi:10.1186/1744-859X-11-16. PMC 3416662. PMID 22731684.
- 1 2 3 4 Gillberg C, Billstedt E (November 2000). "Autism and Asperger syndrome: coexistence with other clinical disorders". Acta Psychiatrica Scandinavica. 102 (5): 321–30. doi:10.1034/j.1600-0447.2000.102005321.x. PMID 11098802.
- ↑ Zafeiriou DI, Ververi A, Vargiami E (June 2007). "Childhood autism and associated comorbidities". Brain & Development. 29 (5): 257–72. doi:10.1016/j.braindev.2006.09.003. PMID 17084999.
- 1 2 Roy M, Dillo W, Emrich HM, Ohlmeier MD (January 2009). "Asperger's syndrome in adulthood". Deutsches Ärzteblatt International. 106 (5): 59–64. doi:10.3238/arztebl.2009.0059. PMC 2695286. PMID 19562011.
- ↑ Frith U (January 1996). "Social communication and its disorder in autism and Asperger syndrome". Journal of Psychopharmacology. 10 (1): 48–53. doi:10.1177/026988119601000108. PMID 22302727. S2CID 978233.
- ↑ Lyons V, Fitzgerald M (October 2004). "Humor in autism and Asperger syndrome". Journal of Autism and Developmental Disorders. 34 (5): 521–31. doi:10.1007/s10803-004-2547-8. PMID 15628606. S2CID 22187553.
- ↑ Filipek PA, Accardo PJ, Baranek GT, Cook EH, Dawson G, Gordon B, Gravel JS, Johnson CP, Kallen RJ, Levy SE, Minshew NJ, Ozonoff S, Prizant BM, Rapin I, Rogers SJ, Stone WL, Teplin S, Tuchman RF, Volkmar FR (December 1999). "The screening and diagnosis of autistic spectrum disorders". Journal of Autism and Developmental Disorders. 29 (6): 439–84. doi:10.1023/A:1021943802493. PMID 10638459. S2CID 145113684.
- ↑ Frith U (May 2004). "Emanuel Miller lecture: confusions and controversies about Asperger syndrome". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 45 (4): 672–86. doi:10.1111/j.1469-7610.2004.00262.x. PMID 15056300.
- ↑ Prior M, Ozonoff S (2007). "Psychological factors in autism". In Volkmar FR (ed.). Autism and Pervasive Developmental Disorders (2nd ed.). Cambridge University Press. pp. 69–128. ISBN 978-0-521-54957-8.
- ↑ Bogdashina O (2003). Sensory Perceptional Issues in Autism and Asperger Syndrome: Different Sensory Experiences, Different Perceptual Worlds. Jessica Kingsley. ISBN 978-1-84310-166-6.
- ↑ Rogers SJ, Ozonoff S (December 2005). "Annotation: what do we know about sensory dysfunction in autism? A critical review of the empirical evidence". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 46 (12): 1255–68. doi:10.1111/j.1469-7610.2005.01431.x. PMID 16313426.
- 1 2 Ehlers S, Gillberg C (November 1993). "The epidemiology of Asperger syndrome. A total population study". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 34 (8): 1327–50. doi:10.1111/j.1469-7610.1993.tb02094.x. PMID 8294522.
- ↑ Polimeni MA, Richdale AL, Francis AJ (April 2005). "A survey of sleep problems in autism, Asperger's disorder and typically developing children". Journal of Intellectual Disability Research. 49 (Pt 4): 260–68. doi:10.1111/j.1365-2788.2005.00642.x. PMID 15816813.
- 1 2 Tani P, Lindberg N, Joukamaa M, Nieminen-von Wendt T, von Wendt L, Appelberg B, Rimón R, Porkka-Heiskanen T (2004). "Asperger syndrome, alexithymia and perception of sleep". Neuropsychobiology. 49 (2): 64–70. doi:10.1159/000076412. PMID 14981336. S2CID 45311366.
- ↑ Alexithymia and AS:
- Fitzgerald M, Bellgrove MA (May 2006). "The overlap between alexithymia and Asperger's syndrome". Journal of Autism and Developmental Disorders. 36 (4): 573–76. doi:10.1007/s10803-006-0096-z. PMC 2092499. PMID 16755385.
- Hill EL, Berthoz S (November 2006). "Response to "Letter to the Editor: The overlap between alexithymia and Asperger's syndrome", Fitzgerald and Bellgrove, Journal of Autism and Developmental Disorders, 36(4)". Journal of Autism and Developmental Disorders. 36 (8): 1143–45. doi:10.1007/s10803-006-0287-7. PMID 17080269. S2CID 28686022.
- Lombardo MV, Barnes JL, Wheelwright SJ, Baron-Cohen S (September 2007). Zak P (ed.). "Self-referential cognition and empathy in autism". PLOS ONE. 2 (9): e883. Bibcode:2007PLoSO...2..883L. doi:10.1371/journal.pone.0000883. PMC 1964804. PMID 17849012.
- 1 2 3 4 5 6 Foster B, King BH (October 2003). "Asperger syndrome: to be or not to be?". Current Opinion in Pediatrics. 15 (5): 491–94. doi:10.1097/00008480-200310000-00008. PMID 14508298.
- 1 2 Arndt TL, Stodgell CJ, Rodier PM (2005). "The teratology of autism". International Journal of Developmental Neuroscience. 23 (2–3): 189–99. doi:10.1016/j.ijdevneu.2004.11.001. PMID 15749245. S2CID 17797266.
- ↑ Rutter M (January 2005). "Incidence of autism spectrum disorders: changes over time and their meaning". Acta Paediatrica. 94 (1): 2–15. doi:10.1111/j.1651-2227.2005.tb01779.x. PMID 15858952.
- 1 2 Just MA, Cherkassky VL, Keller TA, Kana RK, Minshew NJ (April 2007). "Functional and anatomical cortical underconnectivity in autism: evidence from an FMRI study of an executive function task and corpus callosum morphometry". Cerebral Cortex. 17 (4): 951–61. doi:10.1093/cercor/bhl006. PMC 4500121. PMID 16772313.
- 1 2 Iacoboni M, Dapretto M (December 2006). "The mirror neuron system and the consequences of its dysfunction". Nature Reviews. Neuroscience. 7 (12): 942–51. doi:10.1038/nrn2024. PMID 17115076. S2CID 9463011.
- ↑ Müller RA (2007). "The study of autism as a distributed disorder". Mental Retardation and Developmental Disabilities Research Reviews. 13 (1): 85–95. doi:10.1002/mrdd.20141. PMC 3315379. PMID 17326118.
- ↑ Rinehart NJ, Bradshaw JL, Brereton AV, Tonge BJ (December 2002). "A clinical and neurobehavioural review of high-functioning autism and Asperger's disorder". The Australian and New Zealand Journal of Psychiatry. 36 (6): 762–70. doi:10.1046/j.1440-1614.2002.01097.x. PMID 12406118. S2CID 563134.
- ↑ Berthier ML, Starkstein SE, Leiguarda R (1990). "Developmental cortical anomalies in Asperger's syndrome: neuroradiological findings in two patients". The Journal of Neuropsychiatry and Clinical Neurosciences. 2 (2): 197–201. doi:10.1176/jnp.2.2.197. PMID 2136076.
- ↑ Happé F, Ronald A, Plomin R (October 2006). "Time to give up on a single explanation for autism". Nature Neuroscience. 9 (10): 1218–20. doi:10.1038/nn1770. PMID 17001340. S2CID 18697986.
- ↑ Happé F, Frith U (January 2006). "The weak coherence account: detail-focused cognitive style in autism spectrum disorders". Journal of Autism and Developmental Disorders. 36 (1): 5–25. doi:10.1007/s10803-005-0039-0. PMID 16450045. S2CID 14999943.
- ↑ Mottron L, Dawson M, Soulières I, Hubert B, Burack J (January 2006). "Enhanced perceptual functioning in autism: an update, and eight principles of autistic perception". Journal of Autism and Developmental Disorders. 36 (1): 27–43. doi:10.1007/s10803-005-0040-7. PMID 16453071. S2CID 327253.
- ↑ Ramachandran VS, Oberman LM (November 2006). "Broken mirrors: a theory of autism" (PDF). Scientific American. 295 (5): 62–69. Bibcode:2006SciAm.295e..62R. doi:10.1038/scientificamerican1106-62. PMID 17076085. Archived (PDF) from the original on 5 February 2009.
- ↑ Nishitani N, Avikainen S, Hari R (April 2004). "Abnormal imitation-related cortical activation sequences in Asperger's syndrome". Annals of Neurology. 55 (4): 558–62. doi:10.1002/ana.20031. PMID 15048895.
- ↑ Baron-Cohen S, Leslie AM, Frith U (October 1985). "Does the autistic child have a "theory of mind"?". Cognition. 21 (1): 37–46. doi:10.1016/0010-0277(85)90022-8. PMID 2934210. S2CID 14955234.
{{cite journal}}: Cite has empty unknown parameter:|1=(help) Pdf. - ↑ Baron-Cohen S (July 2006). "The hyper-systemizing, assortative mating theory of autism" (PDF). Progress in Neuro-Psychopharmacology & Biological Psychiatry. 30 (5): 865–72. doi:10.1016/j.pnpbp.2006.01.010. PMID 16519981. Archived from the original (PDF) on 14 June 2007.
- ↑ Faridi F, Khosrowabadi R (September–October 2017). "Behavioral, cognitive and neural markers of Asperger syndrome". Basic and Clinical Neuroscience. 8 (5): 349–59. doi:10.18869/nirp.bcn.8.5.349. PMC 5691167. PMID 29167722.
- ↑ Szatmari P, Bremner R, Nagy J (August 1989). "Asperger's syndrome: a review of clinical features". Canadian Journal of Psychiatry. 34 (6): 554–60. doi:10.1177/070674378903400613. PMID 2766209. S2CID 45611340.
- ↑ Gillberg IC, Gillberg C (July 1989). "Asperger syndrome--some epidemiological considerations: a research note". Journal of Child Psychology and Psychiatry, and Allied Disciplines. 30 (4): 631–38. doi:10.1111/j.1469-7610.1989.tb00275.x. PMID 2670981.
- 1 2 3 Fitzgerald M, Corvin A (2001). "Diagnosis and differential diagnosis of Asperger syndrome". Adv Psychiatric Treat. 7 (4): 310–18. doi:10.1192/apt.7.4.310. Archived from the original on 10 September 2007.
- ↑ Leskovec TJ, Rowles BM, Findling RL (2008). "Pharmacological treatment options for autism spectrum disorders in children and adolescents". Harvard Review of Psychiatry. 16 (2): 97–112. doi:10.1080/10673220802075852. PMID 18415882.
- ↑ Shattuck PT, Grosse SD (2007). "Issues related to the diagnosis and treatment of autism spectrum disorders". Mental Retardation and Developmental Disabilities Research Reviews. 13 (2): 129–35. doi:10.1002/mrdd.20143. PMID 17563895.
- 1 2 Klin A, Volkmar FR (January 2003). "Asperger syndrome: diagnosis and external validity". Child and Adolescent Psychiatric Clinics of North America. 12 (1): 1–13, v. doi:10.1016/S1056-4993(02)00052-4. PMID 12512395.
- 1 2 Lehnhardt FG, Gawronski A, Pfeiffer K, Kockler H, Schilbach L, Vogeley K (November 2013). "The investigation and differential diagnosis of Asperger syndrome in adults". Deutsches Ärzteblatt International. 110 (45): 755–63. doi:10.3238/arztebl.2013.0755. PMC 3849991. PMID 24290364.
- ↑ Tantam D (January 2003). "The challenge of adolescents and adults with Asperger syndrome". Child and Adolescent Psychiatric Clinics of North America. 12 (1): 143–63, vii–viii. doi:10.1016/S1056-4993(02)00053-6. PMID 12512403.
- ↑ Uekermann J, Daum I (May 2008). "Social cognition in alcoholism: a link to prefrontal cortex dysfunction?". Addiction. 103 (5): 726–35. doi:10.1111/j.1360-0443.2008.02157.x. PMID 18412750.
- ↑ Fitzgerald M (1 July 2001). "Diagnosis and differential diagnosis of Asperger syndrome". Advances in Psychiatric Treatment. 7 (4): 310–18. doi:10.1192/apt.7.4.310. S2CID 3814840.
- ↑ Siu AL, Bibbins-Domingo K, Grossman DC, Baumann LC, Davidson KW, Ebell M, García FA, Gillman M, Herzstein J, Kemper AR, Krist AH, Kurth AE, Owens DK, Phillips WR, Phipps MG, Pignone MP (February 2016). "Screening for Autism Spectrum Disorder in Young Children: US Preventive Services Task Force Recommendation Statement". JAMA. 315 (7): 691–96. doi:10.1001/jama.2016.0018. PMID 26881372.
- ↑ The CAST has been renamed from the Childhood Asperger Syndrome Test to the Childhood Autism Spectrum Test, reflecting the removal of Asperger's Syndrome from the DSM-5. Archived 3 July 2013 at the Wayback Machine
- ↑ Campbell JM (February 2005). "Diagnostic assessment of Asperger's disorder: a review of five third-party rating scales". Journal of Autism and Developmental Disorders. 35 (1): 25–35. doi:10.1007/s10803-004-1028-4. PMID 15796119. S2CID 16437469.
- ↑ Auyeung B, Baron-Cohen S, Wheelwright S, Allison C (August 2008). "The Autism Spectrum Quotient: Children's Version (AQ-Child)" (PDF). Journal of Autism and Developmental Disorders. 38 (7): 1230–40. doi:10.1007/s10803-007-0504-z. PMID 18064550. Archived (PDF) from the original on 5 February 2009.
- ↑ Baron-Cohen S, Hoekstra RA, Knickmeyer R, Wheelwright S (April 2006). "The Autism-Spectrum Quotient (AQ)--adolescent version" (PDF). Journal of Autism and Developmental Disorders. 36 (3): 343–50. CiteSeerX 10.1.1.654.1966. doi:10.1007/s10803-006-0073-6. PMID 16552625. Archived (PDF) from the original on 5 February 2009.
- ↑ Woodbury-Smith MR, Robinson J, Wheelwright S, Baron-Cohen S (June 2005). "Screening adults for Asperger Syndrome using the AQ: a preliminary study of its diagnostic validity in clinical practice" (PDF). Journal of Autism and Developmental Disorders. 35 (3): 331–35. CiteSeerX 10.1.1.653.8639. doi:10.1007/s10803-005-3300-7. PMID 16119474. Archived from the original (PDF) on 17 December 2008.
- ↑ Khouzam HR, El-Gabalawi F, Pirwani N, Priest F (2004). "Asperger's disorder: a review of its diagnosis and treatment". Comprehensive Psychiatry. 45 (3): 184–91. doi:10.1016/j.comppsych.2004.02.004. PMID 15124148.
- ↑ Attwood T (January 2003). "Frameworks for behavioral interventions". Child and Adolescent Psychiatric Clinics of North America. 12 (1): 65–86, vi. doi:10.1016/S1056-4993(02)00054-8. PMID 12512399.
- ↑ Krasny L, Williams BJ, Provencal S, Ozonoff S (January 2003). "Social skills interventions for the autism spectrum: essential ingredients and a model curriculum". Child and Adolescent Psychiatric Clinics of North America. 12 (1): 107–22. doi:10.1016/S1056-4993(02)00051-2. PMID 12512401.
- 1 2 Myles BS (January 2003). "Behavioral forms of stress management for individuals with Asperger syndrome". Child and Adolescent Psychiatric Clinics of North America. 12 (1): 123–41. doi:10.1016/S1056-4993(02)00048-2. PMID 12512402.
- 1 2 3 4 Towbin KE (January 2003). "Strategies for pharmacologic treatment of high functioning autism and Asperger syndrome". Child and Adolescent Psychiatric Clinics of North America. 12 (1): 23–45. doi:10.1016/S1056-4993(02)00049-4. PMID 12512397. Archived from the original on 9 November 2019. Retrieved 6 August 2020.
- ↑ Paul R (January 2003). "Promoting social communication in high functioning individuals with autistic spectrum disorders". Child and Adolescent Psychiatric Clinics of North America. 12 (1): 87–106, vi–vii. doi:10.1016/S1056-4993(02)00047-0. PMID 12512400.
- 1 2 Matson JL (2007). "Determining treatment outcome in early intervention programs for autism spectrum disorders: a critical analysis of measurement issues in learning based interventions". Research in Developmental Disabilities. 28 (2): 207–18. doi:10.1016/j.ridd.2005.07.006. PMID 16682171.
- ↑ Rao PA, Beidel DC, Murray MJ (February 2008). "Social skills interventions for children with Asperger's syndrome or high-functioning autism: a review and recommendations". Journal of Autism and Developmental Disorders. 38 (2): 353–61. doi:10.1007/s10803-007-0402-4. PMID 17641962. S2CID 2507088.
- ↑ Sofronoff K, Leslie A, Brown W (September 2004). "Parent management training and Asperger syndrome: a randomized controlled trial to evaluate a parent based intervention". Autism. 8 (3): 301–17. doi:10.1177/1362361304045215. PMID 15358872.
- ↑ Hirsch LE, Pringsheim T (June 2016). "Aripiprazole for autism spectrum disorders (ASD)". The Cochrane Database of Systematic Reviews (6): CD009043. doi:10.1002/14651858.CD009043.pub3. PMC 7120220. PMID 27344135.
- ↑ Blankenship K, Erickson CA, Stigler KA, Posey DJ, McDougle CJ (September 2010). "Aripiprazole for irritability associated with autistic disorder in children and adolescents aged 6–17 years". Pediatric Health. 4 (4): 375–81. doi:10.2217/phe.10.45. PMC 3043611. PMID 21359119.
- ↑ Myers SM, Johnson CP (November 2007). "Management of children with autism spectrum disorders". Pediatrics. 120 (5): 1162–82. doi:10.1542/peds.2007-2362. PMID 17967921. Archived from the original on 23 March 2019. Retrieved 6 August 2020.
- 1 2 Newcomer JW (2007). "Antipsychotic medications: metabolic and cardiovascular risk". The Journal of Clinical Psychiatry. 68 Suppl 4 (suppl 4): 8–13. PMID 17539694.
- 1 2 Chavez B, Chavez-Brown M, Sopko MA, Rey JA (2007). "Atypical antipsychotics in children with pervasive developmental disorders". Paediatric Drugs. 9 (4): 249–66. CiteSeerX 10.1.1.659.4150. doi:10.2165/00148581-200709040-00006. PMID 17705564.
- ↑ Staller J (June 2006). "The effect of long-term antipsychotic treatment on prolactin". Journal of Child and Adolescent Psychopharmacology. 16 (3): 317–26. doi:10.1089/cap.2006.16.317. PMID 16768639.
- ↑ Stachnik JM, Nunn-Thompson C (April 2007). "Use of atypical antipsychotics in the treatment of autistic disorder". The Annals of Pharmacotherapy. 41 (4): 626–34. doi:10.1345/aph.1H527. PMID 17389666. S2CID 31715163.
- ↑ Blacher J, Kraemer B, Schalow M (2003). "Asperger syndrome and high functioning autism: research concerns and emerging foci". Current Opinion in Psychiatry. 16 (5): 535–42. doi:10.1097/00001504-200309000-00008.
- ↑ Coplan J, Jawad AF (July 2005). "Modeling clinical outcome of children with autistic spectrum disorders". Pediatrics. 116 (1): 117–22. doi:10.1542/peds.2004-1118. PMID 15995041.
- ↑ Chiang HM, Lin YH (November 2007). "Mathematical ability of students with Asperger syndrome and high-functioning autism: a review of literature". Autism. 11 (6): 547–56. doi:10.1177/1362361307083259. PMID 17947290. – via SAGE Journals (subscription required)
- ↑ Moran M (2006). "Asperger's may be answer to diagnostic mysteries". Psychiatric News. 41 (19): 21–36. doi:10.1176/pn.41.19.0021.
- ↑ Gillberg C (2008). "Asperger syndrome – mortality and morbidity". In Rausch JL, Johnson ME, Casanova MF (eds.). Asperger's Disorder. Informa Healthcare. pp. 63–80. ISBN 978-0-8493-8360-1.
- ↑ Fombonne E, Tidmarsh L (January 2003). "Epidemiologic data on Asperger disorder". Child and Adolescent Psychiatric Clinics of North America. 12 (1): 15–21, v–vi. doi:10.1016/S1056-4993(02)00050-0. PMID 12512396.
- ↑ Fombonne E (2007). "Epidemiological surveys of pervasive developmental disorders". In Volkmar FR (ed.). Autism and Pervasive Developmental Disorders (2nd ed.). Cambridge University Press. pp. 33–68. ISBN 978-0-521-54957-8.
- 1 2 Mattila ML, Kielinen M, Jussila K, Linna SL, Bloigu R, Ebeling H, Moilanen I (May 2007). "An epidemiological and diagnostic study of Asperger syndrome according to four sets of diagnostic criteria". Journal of the American Academy of Child and Adolescent Psychiatry. 46 (5): 636–46. doi:10.1097/chi.0b013e318033ff42. PMID 17450055.
- ↑ Galanopoulos, Anastasios; Robertson, Dene; Woodhouse, Emma (4 January 2016). "The assessment of autism spectrum disorders in adults". Advances in Autism. 2 (1): 31–40. doi:10.1108/AIA-09-2015-0017.
- ↑ Cederlund M, Gillberg C (October 2004). "One hundred males with Asperger syndrome: a clinical study of background and associated factors". Developmental Medicine and Child Neurology. 46 (10): 652–60. doi:10.1111/j.1469-8749.2004.tb00977.x. PMID 15473168.
- ↑ Lugnegård T, Hallerbäck MU, Gillberg C (May 2012). "Personality disorders and autism spectrum disorders: what are the connections?". Comprehensive Psychiatry. 53 (4): 333–40. doi:10.1016/j.comppsych.2011.05.014. PMID 21821235.
- ↑ Tantam D (December 1988). "Lifelong eccentricity and social isolation. II: Asperger's syndrome or schizoid personality disorder?". The British Journal of Psychiatry. 153: 783–91. doi:10.1192/bjp.153.6.783. PMID 3256377.
- ↑ Ekleberry, Sharon C. (2008). "Cluster A – Schizoid Personality Disorder and Substance Use Disorders". Integrated Treatment for Co-Occurring Disorders: Personality Disorders and Addiction. Routledge. pp. 31–32. ISBN 978-0789036933. Archived from the original on 25 February 2021. Retrieved 6 August 2020.
- 1 2 3 Baron-Cohen S, Klin A (June 2006). "What's so special about Asperger Syndrome?". Brain and Cognition. 61 (1): 1–4. doi:10.1016/j.bandc.2006.02.002. PMID 16563588. S2CID 12554302.
- ↑ Manouilenko I, Bejerot S (August 2015). "Sukhareva – Prior to Asperger and Kanner". Nordic Journal of Psychiatry (Report). 69 (6): 479–82. doi:10.3109/08039488.2015.1005022. PMID 25826582. Archived from the original on 27 August 2021. Retrieved 6 August 2020.
- ↑ Lyons V, Fitzgerald M (November 2007). "Did Hans Asperger (1906–1980) have Asperger syndrome?". Journal of Autism and Developmental Disorders. 37 (10): 2020–21. doi:10.1007/s10803-007-0382-4. PMID 17917805. S2CID 21595111.
- ↑ Osborne L (2002). American Normal: The Hidden World of Asperger Syndrome. Copernicus. p. 19. ISBN 978-0-387-95307-6.
- ↑ Hippler K, Klicpera C (February 2003). "A retrospective analysis of the clinical case records of 'autistic psychopaths' diagnosed by Hans Asperger and his team at the University Children's Hospital, Vienna". Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 358 (1430): 291–301. doi:10.1098/rstb.2002.1197. PMC 1693115. PMID 12639327.
- ↑ Wing L (1991). "The relationship between Asperger's syndrome and Kanner's autism". In Frith U (ed.). Autism and Asperger syndrome. Cambridge University Press. pp. 93–121. ISBN 978-0-521-38608-1.
- ↑ Cole, Carolyn (24 January 2018). "What is Asperger's Syndrome". Guiding Pathways header logo. Archived from the original on 21 July 2019. Retrieved 21 July 2019.
- ↑ Wing L (February 1981). "Asperger's syndrome: a clinical account". Psychological Medicine. 11 (1): 115–29. doi:10.1017/S0033291700053332. PMID 7208735. Archived from the original on 17 August 2007.
- ↑ Mnookin, Seth (18 June 2018). "Asperger's Children". New York Times. Archived from the original on 27 March 2019. Retrieved 22 July 2019.
- ↑ Wing, Lorna (February 1981). "Asperger's syndrome: a clinical account". Psychological Medicine. Archived from the original on 6 September 2019. Retrieved 22 July 2019.
- ↑ Willey LH (1999). Pretending to be Normal: Living with Asperger's Syndrome. Jessica Kingsley. pp. 71, 104. ISBN 978-1-85302-749-9.
- ↑ Williams CC (2005). "In search of an Asperger". In Stoddart KP (ed.). Children, Youth and Adults with Asperger Syndrome: Integrating Multiple Perspectives. Jessica Kingsley. pp. 242–52. ISBN 978-1-84310-319-6.
The life prospects of people with AS would change if we shifted from viewing AS as a set of dysfunctions, to viewing it as a set of differences that have merit.
- ↑ Dakin CJ (2005). "Life on the outside: A personal perspective of Asperger syndrome". In Stoddart KP (ed.). Children, Youth and Adults with Asperger Syndrome: Integrating Multiple Perspectives. Jessica Kingsley. pp. 352–61. ISBN 978-1-84310-319-6.
- ↑ Clarke J, van Amerom G (2008). "Asperger's syndrome: differences between parents' understanding and those diagnosed". Social Work in Health Care. 46 (3): 85–106. doi:10.1300/J010v46n03_05. PMID 18551831.
- ↑ Allred S (2009). "Reframing Asperger syndrome: lessons from other challenges to the Diagnostic and Statistical Manual and ICIDH approaches". Disability & Society. 24 (3): 343–55. doi:10.1080/09687590902789511.
- ↑ Baron-Cohen S (2008). "The evolution of brain mechanisms for social behavior". In Crawford C, Krebs D (eds.). Foundations of Evolutionary Psychology. Lawrence Erlbaum. pp. 415–32. ISBN 978-0-8058-5957-7.
- 1 2 Jaarsma P, Welin S (March 2012). "Autism as a natural human variation: reflections on the claims of the neurodiversity movement" (PDF). Health Care Analysis. 20 (1): 20–30. doi:10.1007/s10728-011-0169-9. PMID 21311979. Archived from the original (PDF) on 1 November 2013.
- ↑ Hamilton, Jon. "Shortage of Brain Tissue Hinders Autism Research". NPR. Archived from the original on 11 March 2015. Retrieved 10 May 2015.
- ↑ Solomon A (25 May 2008). "The autism rights movement". New York. Archived from the original on 27 May 2008. Retrieved 27 May 2008.
External links
- Asperger's Syndrome at Curlie
| Classification | |
|---|---|
| External resources |