Food allergy
| Food allergy | |
|---|---|
 | |
| Hives on the back are a common allergy symptom. | |
| Specialty | Emergency medicine |
| Symptoms | Itchiness, swelling of the tongue, vomiting, diarrhea, hives, trouble breathing, low blood pressure[1] |
| Usual onset | Minutes to several hours of exposure[1] |
| Duration | Long term, some may resolve[2] |
| Causes | Immune response to food[1] |
| Risk factors | Family history, vitamin D deficiency, obesity, high levels of cleanliness[1][2] |
| Diagnostic method | Based on a medical history, elimination diet, skin prick test, oral food challenge[1][2] |
| Differential diagnosis | Food intolerance, celiac disease, food poisoning[1] |
| Prevention | Early exposure to potential allergens[2][3] |
| Treatment | Avoiding the food in question, having a plan if exposure occurs, medical alert jewelry[1][2] |
| Medication | Adrenaline (epinephrine)[1] |
| Frequency | ~6% (developed world)[1][2] |
A food allergy is an abnormal immune response to food.[1] The symptoms of the allergic reaction may range from mild to severe.[1] They may include itchiness, swelling of the tongue, vomiting, diarrhea, hives, trouble breathing, or low blood pressure.[1] This typically occurs within minutes to several hours of exposure.[1] When the symptoms are severe, it is known as anaphylaxis.[1] A food intolerance and food poisoning are separate conditions, not due to an immune response.[1][4]
Common foods involved include cow's milk, peanuts, eggs, shellfish, fish, tree nuts, soy, wheat, rice, and fruit.[1][2][5] The common allergies vary depending on the country.[1] Risk factors include a family history of allergies, vitamin D deficiency, obesity, and high levels of cleanliness.[1][2] Allergies occur when immunoglobulin E (IgE), part of the body's immune system, binds to food molecules.[1] A protein in the food is usually the problem.[2] This triggers the release of inflammatory chemicals such as histamine.[1] Diagnosis is usually based on a medical history, elimination diet, skin prick test, blood tests for food-specific IgE antibodies, or oral food challenge.[1][2]
Early exposure to potential allergens may be protective.[2][3] Management primarily involves avoiding the food in question and having a plan if exposure occurs.[2] This plan may include giving adrenaline (epinephrine) and wearing medical alert jewelry.[1] The benefits of allergen immunotherapy for food allergies is unclear, thus is not recommended as of 2015.[6] Some types of food allergies among children resolve with age, including that to milk, eggs, and soy; while others such as to nuts and shellfish typically do not.[2]
In the developed world, about 4% to 8% of people have at least one food allergy.[1][2] They are more common in children than adults and appear to be increasing in frequency.[2] Male children appear to be more commonly affected than females.[2] Some allergies more commonly develop early in life, while others typically develop in later life.[1] In developed countries, a large proportion of people believe they have food allergies when they actually do not have them.[7][8][9] The declaration of the presence of trace amounts of allergens in foods is mandatory only in Brazil.[10][11][12]
Signs and symptoms
Food allergies usually have a fast onset (from seconds to one hour) and may include:[13]
- Rash
- Hives[13]
- Itching of mouth, lips, tongue, throat, eyes, skin, or other areas[13]
- Swelling (angioedema) of lips, tongue, eyelids, or the whole face[13]
- Difficulty swallowing[13]
- Runny or congested nose[13]
- Hoarse voice[13]
- Wheezing and/or shortness of breath[13]
- Diarrhea, abdominal pain, and/or stomach cramps[13]
- Lightheadedness[13]
- Fainting[13]
- Nausea[13]
- Vomiting[13]
In some cases, however, onset of symptoms may be delayed for hours.[13]
Symptoms can vary. The amount of food needed to trigger a reaction also varies.[14]
Serious danger regarding allergies can begin when the respiratory tract or blood circulation is affected. The former can be indicated through wheezing and cyanosis. Poor blood circulation leads to a weak pulse, pale skin and fainting.[15]
A severe case of an allergic reaction, caused by symptoms affecting the respiratory tract and blood circulation, is called anaphylaxis. When symptoms are related to a drop in blood pressure, the person is said to be in anaphylactic shock. Anaphylaxis occurs when IgE antibodies are involved, and areas of the body that are not in direct contact with the food become affected and show symptoms.[16] Those with asthma or an allergy to peanuts, tree nuts, or seafood are at greater risk for anaphylaxis.[17]
Cause
Although sensitivity levels vary by country, the most common food allergies are allergies to milk, eggs, peanuts, tree nuts, fish, shellfish, soy, and wheat.[18] These are often referred to as "the big eight".[19] Allergies to seeds — especially sesame — seem to be increasing in many countries.[20] An example an allergy more common to a particular region is that to rice in East Asia where it forms a large part of the diet.[21]
One of the most common food allergies is a sensitivity to peanuts, a member of the bean family. Peanut allergies may be severe, but children with peanut allergies sometimes outgrow them.[22] Tree nuts, including almonds, brazil nuts, cashews, coconuts, hazelnuts, macadamia nuts, pecans, pistachios, pine nuts, and walnuts, are also common allergens. Sufferers may be sensitive to one particular tree nut or to many different ones.[23] Also, seeds, including sesame seeds and poppy seeds, contain oils where protein is present, which may elicit an allergic reaction.[23]
Egg allergies affect about one in 50 children but are frequently outgrown by children when they reach age five.[24] Typically, the sensitivity is to proteins in the white, rather than the yolk.[23]
Milk from cows, goats, or sheep is another common food allergen, and many sufferers are also unable to tolerate dairy products such as cheese. A small portion of children with a milk allergy, roughly 10%, have a reaction to beef. Beef contains a small amount of protein that is also present in cow's milk.[25]
Seafood is one of the most common sources of food allergens; people may be allergic to proteins found in fish, crustaceans, or mollusks.[26]
Other foods containing allergenic proteins include soy, wheat, fruits, vegetables, maize, spices, synthetic and natural colors, and chemical additives.
Balsam of Peru, which is in various foods, is in the "top five" allergens most commonly causing patch test reactions in people referred to dermatology clinics.[27][28][29]
Sensitization
Sensitization can occur through the gastrointestinal tract, respiratory tract and possibly the skin.[30] Damage to the skin in conditions such as eczema has been proposed as a risk factor for sensitization.[31] An Institute of Medicine report says that food proteins contained in vaccines, such as gelatin, milk, or egg can cause sensitization (development of allergy) in vaccine recipients, to those food items.[32]
Atopy
Food allergies develop more easily in people with the atopic syndrome, a very common combination of diseases: allergic rhinitis and conjunctivitis, eczema, and asthma.[33] The syndrome has a strong inherited component; a family history of allergic diseases can be indicative of the atopic syndrome.
Cross-reactivity
Some children who are allergic to cow's milk protein also show a cross-sensitivity to soy-based products.[34] Some infant formulas have their milk and soy proteins hydrolyzed, so when taken by infants, their immune systems do not recognize the allergen and they can safely consume the product. Hypoallergenic infant formulas can be based on proteins partially predigested to a less antigenic form. Other formulas, based on free amino acids, are the least antigenic and provide complete nutritional support in severe forms of milk allergy.
Crustaceans (shrimp, crab, lobster, etc.) and molluscs (mussel, oyster, scallop, squid, octopus, snail, etc.) are different invertebrate classes, but the allergenic protein tropomyosin is present and responsible for cross-reactivity.[35]
People with latex allergy often also develop allergies to bananas, kiwifruit, avocados, and some other foods.[36]
Pathophysiology

Conditions caused by food allergies are classified into three groups according to the mechanism of the allergic response:[37]
- IgE-mediated (classic) – the most common type, occurs shortly after eating and may involve anaphylaxis.
- Non-IgE mediated – characterized by an immune response not involving immunoglobulin E; may occur some hours after eating, complicating diagnosis
- IgE and/or non-IgE-mediated – a hybrid of the above two types
Allergic reactions are hyperactive responses of the immune system to generally innocuous substances. When immune cells encounter the allergenic protein, IgE antibodies are produced; this is similar to the immune system's reaction to foreign pathogens. The IgE antibodies identify the allergenic proteins as harmful and initiate the allergic reaction. The harmful proteins are those that do not break down due to the strong bonds of the protein. IgE antibodies bind to a receptor on the surface of the protein, creating a tag, just as a virus or parasite becomes tagged. Why some proteins do not denature and subsequently trigger allergic reactions and hypersensitivity while others do is not entirely clear.[38]
Hypersensitivities are categorized according to the parts of the immune system that are attacked and the amount of time it takes for the response to occur. The four types of hypersensitivity reaction are: type 1, immediate IgE-mediated; type 2, cytotoxic; type 3, immune complex-mediated; and type 4, delayed cell-mediated.[39] The pathophysiology of allergic responses can be divided into two phases. The first is an acute response that occurs immediately after exposure to an allergen. This phase can either subside or progress into a "late-phase reaction" which can substantially prolong the symptoms of a response, and result in tissue damage.
Many food allergies are caused by hypersensitivities to particular proteins in different foods. Proteins have unique properties that allow them to become allergens, such as stabilizing forces in their tertiary and quaternary structures which prevent degradation during digestion. Many theoretically allergenic proteins cannot survive the destructive environment of the digestive tract, thus do not trigger hypersensitive reactions.[40]
Acute response
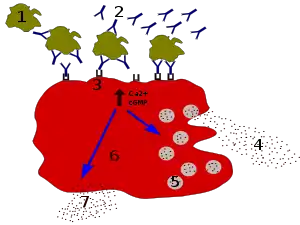
1 — antigen
2 — IgE antibody
3 — FcεRI receptor
4 — preformed mediators (histamine, proteases, chemokines, heparin)
5 — granules
6 — mast cell
7 — newly formed mediators (prostaglandins, leukotrienes, thromboxanes, PAF)
In the early stages of allergy, a type I hypersensitivity reaction against an allergen, encountered for the first time, causes a response in a type of immune cell called a TH2 lymphocyte, which belongs to a subset of T cells that produce a cytokine called interleukin-4 (IL-4). These TH2 cells interact with other lymphocytes called B cells, whose role is the production of antibodies. Coupled with signals provided by IL-4, this interaction stimulates the B cell to begin production of a large amount of a particular type of antibody known as IgE. Secreted IgE circulates in the blood and binds to an IgE-specific receptor (a kind of Fc receptor called FcεRI) on the surface of other kinds of immune cells called mast cells and basophils, which are both involved in the acute inflammatory response. The IgE-coated cells, at this stage, are sensitized to the allergen.[41]
If later exposure to the same allergen occurs, the allergen can bind to the IgE molecules held on the surface of the mast cells or basophils. Cross-linking of the IgE and Fc receptors occurs when more than one IgE-receptor complex interacts with the same allergenic molecule, and activates the sensitized cell. Activated mast cells and basophils undergo a process called degranulation, during which they release histamine and other inflammatory chemical mediators (cytokines, interleukins, leukotrienes, and prostaglandins) from their granules into the surrounding tissue causing several systemic effects, such as vasodilation, mucous secretion, nerve stimulation, and smooth-muscle contraction. This results in rhinorrhea, itchiness, dyspnea, and anaphylaxis. Depending on the individual, the allergen, and the mode of introduction, the symptoms can be system-wide (classical anaphylaxis), or localized to particular body systems.[41]
Late-phase response
After the chemical mediators of the acute response subside, late-phase responses can often occur due to the migration of other leukocytes such as neutrophils, lymphocytes, eosinophils, and macrophages to the initial site. The reaction is usually seen 2–24 hours after the original reaction.[42] Cytokines from mast cells may also play a role in the persistence of long-term effects.[43]
Diagnosis


Diagnosis is usually based on a medical history, elimination diet, skin prick test, blood tests for food-specific IgE antibodies, or oral food challenge.[1][2]
- For skin-prick tests, a tiny board with protruding needles is used. The allergens are placed either on the board or directly on the skin. The board is then placed on the skin, to puncture the skin and for the allergens to enter the body. If a hive appears, the person is considered positive for the allergy. This test only works for IgE antibodies. Allergic reactions caused by other antibodies cannot be detected through skin-prick tests.[44]
Skin-prick testing is easy to do and results are available in minutes. Different allergists may use different devices for testing. Some use a "bifurcated needle", which looks like a fork with two prongs. Others use a "multitest", which may look like a small board with several pins sticking out of it. In these tests, a tiny amount of the suspected allergen is put onto the skin or into a testing device, and the device is placed on the skin to prick, or break through, the top layer of skin. This puts a small amount of the allergen under the skin. A hive will form at any spot where the person is allergic. This test generally yields a positive or negative result. It is good for quickly learning if a person is allergic to a particular food or not, because it detects IgE. Skin tests cannot predict if a reaction would occur or what kind of reaction might occur if a person ingests that particular allergen. They can, however, confirm an allergy in light of a patient's history of reactions to a particular food. Non-IgE-mediated allergies cannot be detected by this method.
- Patch testing is used to determine if a specific substance causes allergic inflammation of the skin. It tests for delayed food reactions.[45][46][47]
- Blood testing is another way to test for allergies; however, it poses the same disadvantage and only detects IgE allergens and does not work for every possible allergen. Radioallergosorbent testing (RAST) is used to detect IgE antibodies present to a certain allergen. The score taken from the RAST is compared to predictive values, taken from a specific type of RAST. If the score is higher than the predictive values, a great chance the allergy is present in the person exists. One advantage of this test is that it can test many allergens at one time.[48]
A CAP-RAST has greater specificity than RAST; it can show the amount of IgE present to each allergen.[49] Researchers have been able to determine "predictive values" for certain foods, which can be compared to the RAST results. If a person's RAST score is higher than the predictive value for that food, over a 95% chance exists that patients will have an allergic reaction (limited to rash and anaphylaxis reactions) if they ingest that food. Currently, predictive values are available for milk, egg, peanut, fish, soy, and wheat.[50][51][52] Blood tests allow for hundreds of allergens to be screened from a single sample, and cover food allergies as well as inhalants. However, non-IgE-mediated allergies cannot be detected by this method. Other widely promoted tests such as the antigen leukocyte cellular antibody test and the food allergy profile are considered unproven methods, the use of which is not advised.[53]
- Food challenges test for allergens other than those caused by IgE allergens. The allergen is given to the person in the form of a pill, so the person can ingest the allergen directly. The person is watched for signs and symptoms. The problem with food challenges is that they must be performed in the hospital under careful watch, due to the possibility of anaphylaxis.[54]
Food challenges, especially double-blind, placebo-controlled food challenges, are the gold standard for diagnosis of food allergies, including most non-IgE-mediated reactions, but is rarely done.[55] Blind food challenges involve packaging the suspected allergen into a capsule, giving it to the patient, and observing the patient for signs or symptoms of an allergic reaction.
The recommended method for diagnosing food allergy is to be assessed by an allergist. The allergist will review the patient's history and the symptoms or reactions that have been noted after food ingestion. If the allergist feels the symptoms or reactions are consistent with food allergy, he/she will perform allergy tests. Additional diagnostic tools for evaluation of eosinophilic or non-IgE mediated reactions include endoscopy, colonoscopy, and biopsy.
Differential diagnosis
Important differential diagnoses are:
- Lactose intolerance generally develops later in life, but can present in young patients in severe cases. It is due to an enzyme deficiency (lactase) and not allergy, and occurs in many non-Western people.
- Celiac disease. While it is caused by a permanent intolerance to gluten (present in wheat, rye, barley and oats), is not an allergy nor simply an intolerance, but a chronic, multiple-organ autoimmune disorder primarily affecting the small intestine.[56][57][58]
- Irritable bowel syndrome
- C1 Esterase inhibitor deficiency (hereditary angioedema), a rare disease, generally causes attacks of angioedema, but can present solely with abdominal pain and occasional diarrhea.
Prevention
Breastfeeding for more than four months may prevent atopic dermatitis, cow's milk allergy, and wheezing in early childhood.[59] Early exposure to potential allergens may be protective.[2] Specifically, early exposure to eggs and peanuts reduces the risk of allergies to these.[3] Guidelines suggest introducing peanuts as early as 4–6 months and include precautionary measures for high-risk infants.[60] The former guidelines, advising delaying the introduction of peanuts, are now thought to have contributed to the increase in peanut allergy seen recently.[61]
To avoid an allergic reaction, a strict diet can be followed. It is difficult to determine the amount of allergenic food required to elicit a reaction, so complete avoidance should be attempted. In some cases, hypersensitive reactions can be triggered by exposures to allergens through skin contact, inhalation, kissing, participation in sports, blood transfusions, cosmetics, and alcohol.[62]
Inhalation exposure
Allergic reactions to airborne particles or vapors of known food allergens have been reported as an occupational consequence of people working in the food industry, but can also take place in home situations, restaurants, or confined spaces such as airplanes. According to two reviews, respiratory symptoms are common, but in some cases there has been progression to anaphylaxis.[63][64] The most frequent reported cases of reactions by inhalation of allergenic foods were due to peanut, seafood, legumes, tree nut, and cow's milk.[63] Steam rising from cooking of lentils, green beans, chickpeas and fish has been well documented as triggering reactions, including anaphylactic reactions.[63][65] One review mentioned case study examples of allergic responses to inhalation of other foods, including examples in which oral consumption of the food is tolerated.[63]
Treatment
The mainstay of treatment for food allergy is total avoidance of the foods identified as allergens. An allergen can enter the body by consuming a food containing the allergen, and can also be ingested by touching any surfaces that may have come into contact with the allergen, then touching the eyes or nose. For people who are extremely sensitive, avoidance includes avoiding touching or inhaling the problematic food. Total avoidance is complicated because the declaration of the presence of trace amounts of allergens in foods is not mandatory (see regulation of labelling).
If the food is accidentally ingested and a systemic reaction (anaphylaxis) occurs, then epinephrine should be used. A second dose of epinephrine may be required for severe reactions. The person should then be transported to the emergency room, where additional treatment can be given. Other treatments include antihistamines and steroids.[66]
Epinephrine

Epinephrine (adrenaline) is the first-line treatment for severe allergic reactions (anaphylaxis). If administered in a timely manner, epinephrine can reverse its effects. Epinephrine relieves airway swelling and obstruction, and improves blood circulation; blood vessels are tightened and heart rate is increased, improving circulation to body organs. Epinephrine is available by prescription in an autoinjector.[67]
Antihistamines
Antihistamines can alleviate some of the milder symptoms of an allergic reaction, but do not treat all symptoms of anaphylaxis.[68] Antihistamines block the action of histamine, which causes blood vessels to dilate and become leaky to plasma proteins. Histamine also causes itchiness by acting on sensory nerve terminals. The most common antihistamine given for food allergies is diphenhydramine.
Steroids
Glucocorticoid steroids are used to calm down the immune system cells that are attacked by the chemicals released during an allergic reaction. This treatment in the form of a nasal spray should not be used to treat anaphylaxis, for it only relieves symptoms in the area in which the steroid is in contact. Another reason steroids should not be used is the delay in reducing inflammation. Steroids can also be taken orally or through injection, by which every part of the body can be reached and treated, but a long time is usually needed for these to take effect.[69]
Epidemiology
The most common food allergens account for about 90% of all allergic reactions;[70] in adults they include shellfish, peanuts, tree nuts, fish, and egg.[71] In children, they include milk, eggs, peanuts, and tree nuts.[71] Six to 8% of children under the age of three have food allergies and nearly 4% of adults have food allergies.[71]
For reasons not entirely understood, the diagnosis of food allergies has apparently become more common in Western nations recently.[72] One possible explanation for this is the "old friends" hypothesis which suggests that non disease causing organisms, such as helminths, could protect against allergy. Therefore, reduced exposure to these organisms, particularly in developed countries, could have contributed towards the increase.[73]
In the United States, food allergy affects as many as 5% of infants less than three years of age[74] and 3% to 4% of adults.[75] A similar prevalence is found in Canada.[76]
About 75% of children who have allergies to milk protein are able to tolerate baked-in milk products, i.e., muffins, cookies, cake, and hydrolyzed formulas.[77]
About 50% of children with allergies to milk, egg, soy, peanuts, tree nuts, and wheat will outgrow their allergy by the age of 6. Those who are still allergic by the age of 12 or so have less than an 8% chance of outgrowing the allergy.[78]
Peanut and tree nut allergies are less likely to be outgrown, although evidence now shows[79] that about 20% of those with peanut allergies and 9% of those with tree nut allergies will outgrow them.[80]
In Japan, allergy to buckwheat flour, used for soba noodles, is more common than peanuts, tree nuts or foods made from soy beans.[81]
United States
In the United States, an estimated 12 million people have food allergies. Food allergy affects as many as 5% of infants less than three years of age[74] and 3% to 4% of adults.[75][82] The prevalence of food allergies is rising.[72][83][84] Food allergies cause roughly 30,000 emergency room visits and 150 deaths per year.[85]
Society and culture
Whether rates of food allergy are increasing or not, food allergy awareness has definitely increased, with impacts on the quality of life for children, their parents and their caregivers.[86][87][88][89] In the United States, the Food Allergen Labeling and Consumer Protection Act of 2004 causes people to be reminded of allergy problems every time they handle a food package, and restaurants have added allergen warnings to menus. The Culinary Institute of America, a premier school for chef training, has courses in allergen-free cooking and a separate teaching kitchen.[90] School systems have protocols about what foods can be brought into the school. Despite all these precautions, people with serious allergies are aware that accidental exposure can easily occur at other peoples' houses, at school or in restaurants.[91] Food fear has a significant impact on quality of life.[88][89] For children with allergies, their quality of life is also affected by actions of their peers. There is an increased occurrence of bullying, which can include threats or acts of deliberately being touched with foods they need to avoid, also having their allergen-free food deliberately contaminated.[92] In the 2018 animated/live action movie Peter Rabbit, rabbits used blackberries to deliberately induce an anaphylactic allergy response in a farmer who is trying to protect his garden. After many public protests, Sony Pictures and the director apologized for making light of food allergies.[93]
Regulation of labelling

In response to the risk that certain foods pose to those with food allergies, some countries have responded by instituting labeling laws that require food products to clearly inform consumers if their products contain priority allergens or byproducts of major allergens among the ingredients intentionally added to foods.
The priority allergens vary by country.
| Food | US | Canada | UK | Australia | EU |
|---|---|---|---|---|---|
| peanuts | Yes[94] | Yes[95] | Yes[96] | Yes[97] | Yes[98] |
| tree nuts | Yes[94] | Yes[95] | Yes[96] | Yes[97] | Yes[98] |
| milk | Yes[94] | Yes[95] | Yes[96] | Yes[97] | Yes[98] |
| eggs | Yes[94] | Yes[95] | Yes[96] | Yes[97] | Yes[98] |
| fish | Yes[94] | Yes[95] | Yes[96] | Yes[97] | Yes[98] |
| shellfish | Crustaceans only[94] | Crustaceans and molluscs[95] | Crustaceans and molluscs[96] | Yes[97] | Crustaceans and molluscs[98] |
| soy | Yes[94] | Yes[95] | Yes[96] | Yes[97] | Yes[98] |
| wheat | Yes[94] | Includes triticale[95] | Included under gluten[96] | Yes[97] | Included under gluten[98] |
| sesame seeds | No | Yes[95] | Yes[96] | Yes[97] | Yes[98] |
| mustard | No | Yes[95] | Yes[96] | No | Yes[98] |
| sulphites (not a true allergy) | No | Yes[95] | Yes[96] | No | Yes, >10 mg/kg[98] |
| gluten (not a true allergy) | No | Yes[95] | Yes[96] | No | Yes[98] |
| celery | No | No | Yes[96] | No | Yes[98] |
| lupin | No | No | Yes[96] | Yes[97] | Yes[98] |
There are no labeling laws mandating declaration of the presence of trace amounts in the final product as a consequence of cross-contamination, except in Brazil.[12][99][100][101][102][103][10][11]
Ingredients intentionally added
In the United States, the Food Allergen Labeling and Consumer Protection Act of 2004 (FALCPA) requires companies to disclose on the label whether a packaged food product contains any of these eight major food allergens, added intentionally: cow's milk, peanuts, eggs, shellfish, fish, tree nuts, soy and wheat.[99] (In October 2018 the US FDA issued a request for information for the consideration of labeling for sesame to help protect people who have sesame allergies.)[104] The eight-ingredient is list originated in 1999 from the World Health Organisation Codex Alimentarius Commission.[10] To meet FALCPA labeling requirements, if an ingredient is derived from one of the required-label allergens, then it must either have its "food sourced name" in parentheses, for example "Casein (milk)," or as an alternative, there must be a statement separate but adjacent to the ingredients list: "Contains milk" (and any other of the allergens with mandatory labeling).[99][101] The European Union requires listing for those eight major allergens plus molluscs, celery, mustard, lupin, sesame and sulfites.[100]
FALCPA applies to packaged foods regulated by the FDA, which does not include poultry, most meats, certain egg products, and most alcoholic beverages.[11] However, some meat, poultry, and egg processed products may contain allergenic ingredients. These products are regulated by the Food Safety and Inspection Service (FSIS), which requires that any ingredient be declared in the labeling only by its common or usual name. Neither the identification of the source of a specific ingredient in a parenthetical statement nor the use of statements to alert for the presence of specific ingredients, like "Contains: milk", are mandatory according to FSIS.[102][103] FALCPA also does not apply to food prepared in restaurants.[105][106] The EU Food Information for Consumers Regulation 1169/2011 – requires food businesses to provide allergy information on food sold unpackaged, for example, in catering outlets, deli counters, bakeries and sandwich bars.[107]
In the United States, there is no federal mandate to address the presence of allergens in drug products. FALCPA does not apply to medicines nor to cosmetics.[108]
Trace amounts as a result of cross-contamination
The value of allergen labeling other than for intentional ingredients is controversial. This concerns labeling for ingredients present unintentionally as a consequence of cross-contact or cross-contamination at any point along the food chain (during raw material transportation, storage or handling, due to shared equipment for processing and packaging, etc.).[10][11] Experts in this field propose that if allergen labeling is to be useful to consumers, and healthcare professionals who advise and treat those consumers, ideally there should be agreement on which foods require labeling, threshold quantities below which labeling may be of no purpose, and validation of allergen detection methods to test and potentially recall foods that were deliberately or inadvertently contaminated.[109][110]
Labeling regulations have been modified to provide for mandatory labeling of ingredients plus voluntary labeling, termed precautionary allergen labeling (PAL), also known as “may contain” statements, for possible, inadvertent, trace amount, cross-contamination during production.[10][111] PAL labeling can be confusing to consumers, especially as there can be many variations on the wording of the warning.[111][112] PAL is optional in the United States.[113] As of 2014, PAL is regulated only in Switzerland, Japan, Argentina, and South Africa. Argentina decided to prohibit precautionary allergen labeling since 2010, and instead puts the onus on the manufacturer to control the manufacturing process and label only those allergenic ingredients known to be in the products. South Africa does not permit the use of PAL, except when manufacturers demonstrate the potential presence of allergen due to cross-contamination through a documented risk assessment and despite adherence to Good Manufacturing Practice.[10] In Australia and New Zealand there is a recommendation that PAL be replaced by guidance from VITAL 2.0 (Vital Incidental Trace Allergen Labeling). A review identified "the eliciting dose for an allergic reaction in 1% of the population" as ED01. This threshold reference dose for foods (such as cow's milk, egg, peanut and other proteins) will provide food manufacturers with guidance for developing precautionary labeling and give consumers a better idea of might be accidentally in a food product beyond "may contain."[114][115] VITAL 2.0 was developed by the Allergen Bureau, a food industry sponsored, non-government organization.[116] The European Union has initiated a process to create labeling regulations for unintentional contamination but is not expected to publish such before 2024.[117]
In Brazil, since April 2016, the declaration of the possibility of cross-contamination is mandatory when the product does not intentionally add any allergenic food or its derivatives, but the Good Manufacturing Practices and allergen control measures adopted are not sufficient to prevent the presence of accidental trace amounts. These allergens include wheat, rye, barley, oats and their hybrids, crustaceans, eggs, fish, peanuts, soybean, milk of all species of mammalians, almonds, hazelnuts, cashew nuts, Brazil nuts, macadamia nuts, walnuts, pecan nuts, pistachios, pine nuts, and chestnuts.[12]
Genetically modified food
There are concerns that genetically modified foods, also described as foods sourced from genetically modified organisms (GMO), could be responsible for allergic reactions, and that the widespread acceptance of GMO foods may be responsible for what is a real or perceived increase in the percentage of people with allergies.[118][119][120] There is a scientific consensus that available food derived from GM crops poses no greater risk to human health than conventional food.[121][122][123] A 2016 U.S. National Academy of Sciences report concluded that there is no relationship between consumption of GM foods and the increase in prevalence of food allergies.[119]
One concern is that genetic engineering could make an allergy-provoking food more allergic, meaning that smaller portions would suffice to set off a reaction.[120] Of the food currently in widespread GMO use, only soybeans are identified as a common allergen. However, for the soybean proteins known to trigger allergic reactions, there is more variation from strain to strain than between those and the GMO varieties.[119] Another concern is that genes transferred from one species to another could introduce an allergen in a food not thought of as particularly allergenic. Research on an attempt to enhance the quality of soybean protein by adding genes from Brazil nuts was terminated when human volunteers known to have tree nut allergy reacted to the modified soybeans.[118]
Prior to a new GMO food receiving government approval, certain criteria need to be met. These include: Is the donor species known to be allergenic? Does the amino acid sequence of the transferred proteins resemble the sequence of known allergenic proteins? Are the transferred proteins resistant to digestion - a trait shared by many allergenic proteins?[119] Genes approved for animal use can be restricted from human consumption due to potential for allergic reactions. In 1998 Starlink brand corn restricted to animals was detected in the human food supply, leading to first a voluntary and then a FDA mandated recall.[124] There are requirements in some countries and recommendations in others that all foods containing GMO ingredients be so labeled, and that there be a post-launch monitoring system to report adverse effects (much there exists in some countries for drug and dietary supplement reporting).[118]
Restaurants
In the US, the FDA Food Code states that the person in charge in restaurants should have knowledge about major food allergens, cross-contacts, and symptoms of food allergy reactions. Restaurant staff, including wait staff and kitchen staff, may not be adequately informed about allergenic ingredients, or the risk of cross-contact when kitchen utensils used to prepare food may have been in previous contact with an allergenic food. The problem may be compounded when customers have a hard time describing their food allergies or when wait staff have a hard time understanding those with food allergies when taking an order.[125]
Diagnosing issues
There exists both over-reporting and under-reporting of the prevalence of food allergies. Self-diagnosed perceptions of food allergy are greater than the rates of true food allergy because people confuse non-allergic intolerance with allergy, and also attribute non-allergy symptoms to an allergic response. Conversely, healthcare professionals treating allergic reactions on an out-patient or even hospitalized basis may not report all cases. Recent increases in reported cases may reflect a real change in incidence or an increased awareness on the part of healthcare professionals.[126]
Research
A number of desensitization techniques are being studied.[127] Areas of research include anti-IgE antibody (omalizumab), specific oral tolerance induction (SOTI, also known as OIT for oral immunotherapy), and sublingual immunotherapy (SLIT). The benefits of allergen immunotherapy for food allergies is unclear, thus is not recommended as of 2015.[6]
There is research on the effects of increasing intake of polyunsaturated fatty acids (PUFAs) during pregnancy, lactation, via infant formula and in early childhood on the subsequent risk of developing food allergies during infancy and childhood. From two reviews, maternal intake of omega-3, long-chain fatty acids during pregnancy appeared to reduce the risks of medically diagnosed IgE-mediated allergy, eczema and food allergy per parental reporting in the first 12 months of life,[128][129] but the effects were not all sustained past 12 months.[129] The reviews characterized the literature's evidence as inconsistent and limited.[128][129] Results when breastfeeding mothers were consuming a diet high in PUFAs were inconclusive.[130] For infants, supplementing their diet with oils high in PUFAs did not affect the risks of food allergies, eczema or asthma either as infants or into childhood.[131]
There is research on probiotics, prebiotics and the combination of the two (synbiotics) as a means of treating or preventing infant and child allergies. From reviews, there appears to be a treatment benefit for eczema,[132][133][134] but not asthma, wheezing or rhinoconjunctivitis.[135] The evidence was not consistent for preventing food allergies and this approach cannot yet be recommended.[133][134][136][137]
The Food Standards Agency, in the United Kingdom, are in charge of funding research into food allergies and intolerance.[126] Since their founding in 1994 they have funded over 45 studies.[126] In 2005 Europe created EuroPrevall, a multi-country project dedicated to research involving allergies.[126]
See also
- List of allergens (food and non-food)
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 National Institute of Allergy and Infectious Diseases (July 2012). "Food Allergy An Overview" (PDF). Archived from the original (PDF) on 5 March 2016.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 Sicherer SH, Sampson HA (February 2014). "Food allergy: Epidemiology, pathogenesis, diagnosis, and treatment". J Allergy Clin Immunol. 133 (2): 291–307, quiz 308. doi:10.1016/j.jaci.2013.11.020. PMID 24388012.
- 1 2 3 Ierodiakonou D, Garcia-Larsen V, Logan A, et al. (20 September 2016). "Timing of Allergenic Food Introduction to the Infant Diet and Risk of Allergic or Autoimmune Disease: A Systematic Review and Meta-analysis" (PDF). JAMA. 316 (11): 1181–1192. doi:10.1001/jama.2016.12623. PMID 27654604. Archived (PDF) from the original on 23 July 2018. Retrieved 22 July 2020.
- ↑ Boyce JA, Assa'ad A, Burks AW, et al. (December 2010). "Guidelines for the Diagnosis and Management of Food Allergy in the United States: Summary of the NIAID-Sponsored Expert Panel Report". Journal of Allergy and Clinical Immunology. 126 (6): 1105–1118. doi:10.1016/j.jaci.2010.10.008. PMC 4241958. PMID 21134568. Archived from the original on 31 March 2020. Retrieved 22 July 2020 – via Elsevier.
- ↑ Nowak-Węgrzyn, A; Katz, Y; Mehr, SS; Koletzko, S (May 2015). "Non-IgE-mediated gastrointestinal food allergy". The Journal of Allergy and Clinical Immunology. 135 (5): 1114–24. doi:10.1016/j.jaci.2015.03.025. PMID 25956013.
- 1 2 "Allergen Immunotherapy". 22 April 2015. Archived from the original on 17 June 2015. Retrieved 15 June 2015.
- ↑ "Making sense of allergies" (PDF). Sense About Science. p. 1. Archived from the original (PDF) on 18 June 2015. Retrieved 7 June 2015.
- ↑ Coon ER, Quinonez RA, Moyer VA, et al. (November 2014). "Overdiagnosis: how our compulsion for diagnosis may be harming children". Pediatrics. 134 (5): 1013–23. doi:10.1542/peds.2014-1778. PMID 25287462.
- ↑ Ferreira CT, Seidman E (2007). "Food allergy: a practical update from the gastroenterological viewpoint". J Pediatr (Rio J). 83 (1): 7–20. doi:10.2223/JPED.1587. PMID 17279290.
- 1 2 3 4 5 6 Allen KJ, Turner PJ, Pawankar R, et al. (2014). "Precautionary labelling of foods for allergen content: are we ready for a global framework?". World Allergy Organ J. 7 (1): 1–14. doi:10.1186/1939-4551-7-10. PMC 4005619. PMID 24791183.
- 1 2 3 4 FDA (18 December 2017). "Food Allergies: What You Need to Know". Archived from the original on 25 January 2018. Retrieved 12 January 2018.
- 1 2 3 "Agência Nacional de Vigilância Sanitária Guia sobre Programa de Controle de Alergênicos" (in Portuguese). Agência Nacional de Vigilância Sanitária (ANVISA). 2016. Archived from the original on 29 April 2018. Retrieved 7 April 2018.
{{cite web}}: CS1 maint: unrecognized language (link) - 1 2 3 4 5 6 7 8 9 10 11 12 13 14 MedlinePlus Encyclopedia: Food allergy
- ↑ Simons FE, Ardusso LR, Bilò MB, et al. (23 February 2011). "World allergy organization guidelines for the assessment and management of anaphylaxis". World Allergy Organ J. 4 (2): 13–37. doi:10.1097/WOX.0b013e318211496c. ISSN 1939-4551. PMC 3500036. PMID 23268454.
- ↑ van Ree 1
- ↑ Sicherer 2006, p. 12
- ↑ Food Allergies Archived 2008-09-14 at the Wayback Machine. Food Allergy Initiative. 2009. Accessed 27 Mar 2010.
- ↑ "Food Allergy Facts & Figures". Asthma and Allergy Foundation of America. 28 March 2007. Archived from the original on 7 December 2006. Retrieved 15 March 2007.
- ↑ "Food allergy and intolerance". Allergy & Intolerance. Food Additives and Ingredients Association. Archived from the original on 13 February 2011. Retrieved 8 June 2010.
- ↑ "About Food Allergies". Food Allergy Initiative. 2008. Archived from the original on 12 December 2008. Retrieved 8 December 2008.
- ↑ "Rice Allergy". HealthCentersOnline. 2006. p. 2. Archived from the original on 23 May 2006. Retrieved 26 October 2006.
- ↑ Sicherer 2006, p. 62
- 1 2 3 Sicherer 2006, p. 63
- ↑ Savage JH, Matsui EC, Skripak JM, et al. (December 2007). "The natural history of egg allergy". J Allergy Clin Immunol. 120 (6): 1413–7. doi:10.1016/j.jaci.2007.09.040. PMID 18073126.
- ↑ Sicherer 2006, p. 64
- ↑ "Seafood (Fish, Crustaceans and Shellfish) - Priority food allergens". Health Canada, Health Products and Food Branch, Food Directorate, Bureau of Chemical Safety, Food Research Division. 2012. Archived from the original on 20 November 2016. Retrieved 19 November 2016.
- ↑ Gottfried Schmalz; Dorthe Arenholt Bindslev (2008). Biocompatibility of Dental Materials. Springer. ISBN 9783540777823. Archived from the original on 18 May 2016. Retrieved 5 March 2014.
- ↑ Thomas P. Habif (2009). Clinical Dermatology. Elsevier Health Sciences. ISBN 978-0323080378. Archived from the original on 8 September 2017. Retrieved 6 March 2014.
- ↑ Edward T. Bope; Rick D. Kellerman (2013). Conn's Current Therapy 2014: Expert Consult. Elsevier Health Sciences. ISBN 9780323225724. Archived from the original on 5 May 2016. Retrieved 6 March 2014.
- ↑ Valenta, R; Hochwallner, H; Linhart, B; Pahr, S (2015). "Food Allergies: The Basics". Gastroenterology. 148 (6): 1120–1131.e4. doi:10.1053/j.gastro.2015.02.006. ISSN 1528-0012. PMC 4414527. PMID 25680669. Archived from the original on 28 August 2021. Retrieved 22 July 2020.
- ↑ Flohr C, Perkin M, Logan K, et al. (2013). "Atopic Dermatitis and Disease Severity Are the Main Risk Factors for Food Sensitization in Exclusively Breastfed Infants". Journal of Investigative Dermatology. 134 (2): 345–350. doi:10.1038/jid.2013.298. PMC 3912359. PMID 23867897. Archived from the original on 28 August 2021. Retrieved 22 July 2020.
- ↑ Clayton, E (2012). Adverse Effects of Vaccines: Evidence and Causality. Institute of Medicine. p. 65. ISBN 978-0-309-21435-3. Archived from the original on 10 September 2015. Retrieved 22 July 2020.
- ↑ "Other atopic dermatitis and related conditions". ICD9. Archived from the original on 30 September 2007.
- ↑ "Policy Statement: Hypoallergenic Infant Formulas". American Academy of Pediatrics. 2 August 2000. Archived from the original on 16 January 2008. Retrieved 26 January 2008.
- ↑ Lopata AL, Kleine-Tebbe J, Kamath SD (2016). "Allergens and molecular diagnostics of shellfish allergy: Part 22 of the Series Molecular Allergology". Allergo J Int. 25 (7): 210–218. doi:10.1007/s40629-016-0124-2. PMC 5306157. PMID 28239537.
- ↑ "Other Common Allergens". Food Allergy Research & Education. Archived from the original on 16 June 2014.
- ↑ "Food allergy". NHS Choices. 16 May 2016. Archived from the original on 20 July 2017. Retrieved 31 January 2017.
A food allergy is when the body's immune system reacts unusually to specific foods
- ↑ Food Reactions. Allergies Archived 2010-04-16 at the Wayback Machine. Foodreactions.org. Kent, England. 2005. Accessed 27 Apr 2010.
- ↑ Nester 2009, p. 414
- ↑ Mayo Clinic. Causes of Food Allergies. Archived 2010-02-27 at the Wayback Machine April 2010.
- 1 2 Janeway, Charles; Paul Travers; Mark Walport; Mark Shlomchik (2001). Immunobiology; Fifth Edition. New York and London: Garland Science. pp. e–book. ISBN 978-0-8153-4101-7. Archived from the original on 28 June 2009.
- ↑ Grimbaldeston MA, Metz M, Yu M, et al. (2006). "Effector and potential immunoregulatory roles of mast cells in IgE-associated acquired immune responses". Curr. Opin. Immunol. 18 (6): 751–60. doi:10.1016/j.coi.2006.09.011. PMID 17011762.
- ↑ Holt PG, Sly PD (2007). "Th2 cytokines in the asthma late-phase response". Lancet. 370 (9596): 1396–8. doi:10.1016/S0140-6736(07)61587-6. PMID 17950849.
- ↑ Sicherer 2006, p. 185
- ↑ "Allergies and EGIDs | American Partnership For Eosinophilic Disorders". Apfed.org. Archived from the original on 4 May 2015. Retrieved 31 March 2014.
- ↑ "Patch test in the diagnosis of food allergy". 22 March 2014. Archived from the original on 10 March 2014. Retrieved 31 March 2014.
- ↑ Rokaite R, Labanauskas L, Vaideliene L (24 January 2014). "Role of the skin patch test in diagnosing food allergy in children with atopic dermatitis". Medicina (Kaunas). 40 (11): 1081–7. PMID 15547309.
- ↑ Sicherer 2006, pp. 187–8
- ↑ "What is a RAST test ? What is a CAP-RAST test?". kidswithfoodallergies.org. Archived from the original on 11 May 2013.
- ↑ Sampson, HA; Ho DG (October 1997). "Relationship between food-specific IgE concentrations and the risk of positive food challenges in children and adolescents". J Allergy Clin Immunol. 100 (4): 444–51. doi:10.1016/S0091-6749(97)70133-7. PMID 9338535.
- ↑ Sampson, HA (May 2001). "Utility of food-specific IgE concentrations in predicting symptomatic food allergy". J Allergy Clin Immunol. 107 (5): 891–6. doi:10.1067/mai.2001.114708. PMID 11344358.
- ↑ García-Ara C, Boyano-Martínez T, Díaz-Pena JM, et al. (January 2001). "Specific IgE levels in the diagnosis of immediate hypersensitivity to cows' milk protein in the infant". Allergy Clin Immunol. 107 (1): 185–90. doi:10.1067/mai.2001.111592. PMID 11150010.
- ↑ Wüthrich B (2005). "Unproven techniques in allergy diagnosis". J Investig Allergol Clin Immunol. 15 (2): 86–90. PMID 16047707.
- ↑ Sicherer 2006, p. 189
- ↑ Turnbull JL, Adams HN, Gorard DA (2015). "Review article: the diagnosis and management of food allergy and food intolerances". Aliment Pharmacol Ther (Review). 41 (1): 3–25. doi:10.1111/apt.12984. PMID 25316115.

- ↑ "Celiac Disease". NIDDKD. June 2015. Archived from the original on 13 March 2016. Retrieved 17 March 2016.
- ↑ "Celiac disease". World Gastroenterology Organisation Global Guidelines. July 2016. Archived from the original on 17 March 2017. Retrieved 23 April 2017.
- ↑ Tommasini A, Not T, Ventura A (2011). "Ages of celiac disease: from changing environment to improved diagnostics". World J Gastroenterol (Review). 17 (32): 3665–71. doi:10.3748/wjg.v17.i32.3665. PMC 3181451. PMID 21990947.
- ↑ Greer FR, Sicherer SH, Burks AW (January 2008). "Effects of early nutritional interventions on the development of atopic disease in infants and children: the role of maternal dietary restriction, breastfeeding, timing of introduction of complementary foods, and hydrolyzed formulas". Pediatrics. 121 (1): 183–91. doi:10.1542/peds.2007-3022. PMID 18166574.
- ↑ Chan ES, Abrams EM, Hildebrand KJ, et al. (12 September 2018). "Early introduction of foods to prevent food allergy". Allergy, Asthma & Clinical Immunology. 14 (2): 57. doi:10.1186/s13223-018-0286-1. ISSN 1710-1492. PMC 6157280. PMID 30275847.
- ↑ Du Toit G, Roberts G, Sayre PH, et al. (February 2015). "Randomized trial of peanut consumption in infants at risk for peanut allergy". N. Engl. J. Med. 372 (9): 803–13. doi:10.1056/NEJMoa1414850. PMC 4416404. PMID 25705822.
- ↑ Sicherer 2006, pp. 151–8
- 1 2 3 4 Leonardi S, Pecoraro R, Filippelli M, et al. (2014). "Allergic reactions to foods by inhalation in children". Allergy Asthma Proc. 35 (4): 288–294. doi:10.2500/aap.2014.35.3755. PMID 24992548.
- ↑ James JM, Crespo JF (2007). "Allergic reactions to foods by inhalation". Curr Allergy Asthma Rep. 7 (3): 167–174. doi:10.1007/s11882-007-0017-z. PMID 17448326.
- ↑ Vitaliti G, Pavone P, Spataro G, et al. (2015). "Legumes steam allergy in childhood: Update of the reported cases". Allergol Immunopathol (Madr). 43 (2): 196–202. doi:10.1016/j.aller.2013.09.009. PMID 24411097.
- ↑ "European Food Allergy and Anaphalaxis Public Declaration". the European Academy of Allergy and Clinical Immunology (EAACI). Archived from the original on 15 December 2013. Retrieved 10 December 2013.
- ↑ Sicherer 2006, p. 133
- ↑ Sicherer 2006, p. 131
- ↑ Sicherer 2006, p. 134
- ↑ "About Food Allergies Allergens". Food Allergy Initiative. Archived from the original on 9 December 2013. Retrieved 11 December 2013.
- 1 2 3 National Institute of Allergy and Infectious Diseases (July 2004). "Food Allergy: An Overview" (PDF). National Institutes of Health. p. 35. Archived from the original (PDF) on 5 March 2016.
- 1 2 Kagan RS (February 2003). "Food allergy: an overview". Environ Health Perspect. 111 (2): 223–5. doi:10.1289/ehp.5702. PMC 1241355. PMID 12573910.
- ↑ Rook GA, Adams V, Hunt J, et al. (August 2003). "Mycobacteria and other environmental organisms as immunomodulators for immunoregulatory disorders". Springer Seminars in Immunopathology. 25 (3–4): 237–255. doi:10.1007/s00281-003-0148-9. PMID 15007629.
- 1 2 Sampson H (2004). "Update on food allergy". J Allergy Clin Immunol. 113 (5): 805–819. doi:10.1016/j.jaci.2004.03.014. PMID 15131561.
- 1 2 Sicherer S, Sampson H (2006). "9. Food allergy". J Allergy Clin Immunol. 117 (2 Suppl Mini–Primer): S470–5. doi:10.1016/j.jaci.2005.05.048. PMID 16455349.
- ↑ "Food Allergies and Intolerance". Health Canada. 6 December 2007. Archived from the original on 14 June 2007.
- ↑ Lucendo AJ, Arias A, Gonzalez-Cervera J, Mota-Huertas T, Yague-Compadre JL. Tolerance of a cow's milk-based hydrolyzed formula in patients with eosinophilic esophagitis triggered by milk. Allergy; 68:1065–72. Link Archived 2016-11-28 at the Wayback Machine
- ↑ "What Are Food Allergies? Food Allergy Summary". Asthma and Allergy Foundation of America. 28 March 2007. Archived from the original on 27 October 2007. Retrieved 6 April 2007.
- ↑ "Outgrowing food allergies". Children's Memorial Hospital. Archived from the original on 20 October 2007.
- ↑ Fleischer DM, Conover-Walker MK, Matsui EC, et al. (November 2005). "The natural history of tree nut allergy". J Allergy Clin Immunol. 116 (5): 1087–93. doi:10.1016/j.jaci.2005.09.002. PMID 16275381.
- ↑ Urisu A, Ebisawa M, Ito K, et al. (2014). "Japanese Guideline for Food Allergy 2014". Allergol Int. 63 (3): 399–419. doi:10.2332/allergolint.14-RAI-0770. PMID 25178179.
- ↑ "Food Allergy Media Q&A" (PDF). Food Allergy & Anaphylaxis Network. 26 May 2010. Archived from the original (PDF) on 30 December 2010. Retrieved 25 March 2011.
- ↑ Branum AM, Lukacs SL (2008). "Food allergy among U.S. children: trends in prevalence and hospitalizations". NCHS Data Brief (10): 1–8. PMID 19389315.
- ↑ Ben-Shoshan M, Turnbull E, Clarke A (2012). "Food allergy: temporal trends and determinants". Curr Allergy Asthma Rep. 12 (4): 346–72. doi:10.1007/s11882-012-0274-3. PMID 22723032.
- ↑ Question 6: How serious are food allergies? Archived 12 November 2020 at the Wayback Machine Food Allergen Labeling And Consumer Protection Act of 2004 Questions and Answers, U.S. Food and Drug Administration (2006).
- ↑ Ravid NL, Annunziato RA, Ambrose MA, et al. (2015). "Mental health and quality-of-life concerns related to the burden of food allergy". Psychiatr. Clin. North Am. 38 (1): 77–89. doi:10.1016/j.psc.2014.11.004. PMID 25725570.
- ↑ Morou Z, Tatsioni A, Dimoliatis ID, et al. (2014). "Health-related quality of life in children with food allergy and their parents: a systematic review of the literature". J Investig Allergol Clin Immunol. 24 (6): 382–95. PMID 25668890.
- 1 2 Lange L (2014). "Quality of life in the setting of anaphylaxis and food allergy". Allergo J Int. 23 (7): 252–260. doi:10.1007/s40629-014-0029-x. PMC 4479473. PMID 26120535.
- 1 2 van der Velde JL, Dubois AE, Flokstra-de Blok BM (2013). "Food allergy and quality of life: what have we learned?". Curr Allergy Asthma Rep. 13 (6): 651–61. doi:10.1007/s11882-013-0391-7. PMID 24122150.
- ↑ Culinary Institute of America Archived 10 November 2017 at the Wayback Machine Allergen-free dining oasis comes to the CIA (2017)
- ↑ Shah E, Pongracic J (2008). "Food-induced anaphylaxis: who, what, why, and where?". Pediatr Ann. 37 (8): 536–41. doi:10.3928/00904481-20080801-06. PMID 18751571.
- ↑ Fong AT, Katelaris CH, Wainstein B (2017). "Bullying and quality of life in children and adolescents with food allergy". J Paediatr Child Health. 53 (7): 630–635. doi:10.1111/jpc.13570. PMID 28608485.
- ↑ Sony Apologizes for ‘Peter Rabbit’ Movie’s Allergy Scene Archived 1 June 2020 at the Wayback Machine New York Times, Jacey Fortrin, Feb 12, 2018.
- 1 2 3 4 5 6 7 8 Center for Food Safety and Applied Nutrition (8 November 2018). "Guidance for Industry: Questions and Answers Regarding Food Allergens (Edition 4)". U.S. Food and Drug Administration. Archived from the original on 28 July 2020. Retrieved 8 September 2019.
- 1 2 3 4 5 6 7 8 9 10 11 12 "Common food allergens". Health Canada. 21 June 2005. Archived from the original on 20 July 2020. Retrieved 8 September 2019.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 "Allergen labelling for food manufacturers". Food Standards Agency. Archived from the original on 4 August 2020. Retrieved 8 September 2019.
- 1 2 3 4 5 6 7 8 9 10 "IFN 08-17 – Mandatory allergen labelling". Department of Agriculture, Government of Australia. Archived from the original on 24 August 2019. Retrieved 8 September 2019.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 "REGULATION (EU) No 1169/2011 OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL of 25 October 2011 on the provision of food information to consumers, amending Regulations (EC) No 1924/2006 and (EC) No 1925/2006 of the European Parliament and of the Council, and repealing Commission Directive 87/250/EEC, Council Directive 90/496/EEC, Commission Directive 1999/10/EC, Directive 2000/13/EC of the European Parliament and of the Council, Commission Directives 2002/67/EC and 2008/5/EC and Commission Regulation (EC) No 608/2004". 25 October 2011. Archived from the original on 25 July 2020. Retrieved 22 July 2020.
- 1 2 3 "Food Allergen Labeling and Consumer Protection Act of 2004". FDA. 2 August 2004. Archived from the original on 28 May 2009.
- 1 2 "Food allergen labelling and information requirements under the EU Food Information for Consumers Regulation No. 1169/2011: Technical Guidance" Archived 7 July 2017 at the Wayback Machine (April 2015).
- 1 2 FDA (14 December 2017). "Have Food Allergies? Read the Label". Archived from the original on 12 November 2020. Retrieved 14 January 2018.
- 1 2 "Food Ingredients of Public Health Concern" (PDF). United States Department of Agriculture. Food Safety and Inspection Service. 7 March 2017. Archived (PDF) from the original on 12 November 2020. Retrieved 16 February 2018.
- 1 2 "Allergies and Food Safety". United States Department of Agriculture. Food Safety and Inspection Service. 1 December 2016. Archived from the original on 13 November 2020. Retrieved 16 February 2018.
- ↑ "Statement from FDA Commissioner Scott Gottlieb, M.D., on the FDA's new consideration of labeling for sesame allergies". U.S. Food and Drug Administration. 29 October 2018. Archived from the original on 12 December 2019. Retrieved 8 December 2019.
- ↑ Roses JB (2011). "Food allergen law and the Food Allergen Labeling and Consumer Protection Act of 2004: falling short of true protection for food allergy sufferers". Food Drug Law J. 66 (2): 225–42, ii. PMID 24505841.
- ↑ FDA (18 July 2006). "Food Allergen Labeling And Consumer Protection Act of 2004 Questions and Answers". Archived from the original on 12 November 2020. Retrieved 12 March 2018.
- ↑ "Allergy and intolerance: guidance for businesses". Archived from the original on 8 December 2014. Retrieved 12 December 2014.
- ↑ Shah AV, Serajuddin AT, Mangione RA (2018). "Making All Medications Gluten Free". J Pharm Sci. 107 (5): 1263–1268. doi:10.1016/j.xphs.2017.12.021. PMID 29287928.
- ↑ Mills EN, Valovirta E, Madsen C, et al. (2004). "Information provision for allergic consumers--where are we going with food allergen labelling?". Allergy. 59 (12): 1262–1268. doi:10.1111/j.1398-9995.2004.00720.x. PMID 15507093.
- ↑ Taylor SL, Baumert JL (2015). Worldwide food allergy labeling and detection of allergens in processed foods. Chem Immunol Allergy. Chemical Immunology and Allergy. Vol. 101. pp. 227–234. doi:10.1159/000373910. ISBN 978-3-318-02340-4. PMID 26022883.
- 1 2 DunnGalvin A, Chan CH, Crevel R, et al. (2015). "Precautionary allergen labelling: perspectives from key stakeholder groups". Allergy. 70 (9): 1039–1051. doi:10.1111/all.12614. PMID 25808296.
- ↑ Zurzolo GA, de Courten M, Koplin J, et al. (2016). "Is advising food allergic patients to avoid food with precautionary allergen labelling out of date?". Curr Opin Allergy Clin Immunol. 16 (3): 272–277. doi:10.1097/ACI.0000000000000262. PMID 26981748.
- ↑ Athas, Eric (28 January 2019). "Which Allergens Are in Your Food? You Can't Always Tell From the Labels". The New York Times. ISSN 0362-4331. Archived from the original on 13 April 2020. Retrieved 9 December 2019.
- ↑ Allen KJ, Remington BC, Baumert JL, et al. (2014). "Allergen reference doses for precautionary labeling (VITAL 2.0): clinical implications". J. Allergy Clin. Immunol. 133 (1): 156–164. doi:10.1016/j.jaci.2013.06.042. PMID 23987796.
- ↑ Taylor SL, Baumert JL, Kruizinga AG, et al. (2014). "Establishment of Reference Doses for residues of allergenic foods: report of the VITAL Expert Panel". Food Chem. Toxicol. 63: 9–17. doi:10.1016/j.fct.2013.10.032. PMID 24184597.
- ↑ The VITAL Program Archived 29 November 2020 at the Wayback Machine Allergen Bureau, Australia and New Zealand.
- ↑ Popping B, Diaz-Amigo C (2018). "European Regulations for Labeling Requirements for Food Allergens and Substances Causing Intolerances: History and Future". J AOAC Int. 101 (1): 2–7. doi:10.5740/jaoacint.17-0381. PMID 29202901.
- 1 2 3 Lee TH, Ho HK, Leung TF (2017). "Genetically modified foods and allergy". Hong Kong Med J. 23 (3): 291–295. doi:10.12809/hkmj166189. PMID 28473652.
- 1 2 3 4 Dunn SE, Vicini JL, Glenn KC, et al. (2017). "The allergenicity of genetically modified foods from genetically engineered crops: A narrative and systematic review". Ann. Allergy Asthma Immunol. 119 (3): 214–222.e3. doi:10.1016/j.anai.2017.07.010. PMID 28890018.
- 1 2 Selb R, Wal JM, Moreno FJ, et al. (2017). "Assessment of endogenous allergenicity of genetically modified plants exemplified by soybean - Where do we stand?" (PDF). Food Chem. Toxicol. 101: 139–148. doi:10.1016/j.fct.2017.01.014. hdl:10261/150576. PMID 28111299. Archived (PDF) from the original on 25 July 2018. Retrieved 22 July 2020.
- ↑ Nicolia A, Manzo A, Veronesi F, et al. (March 2014). "An overview of the last 10 years of genetically engineered crop safety research" (PDF). Critical Reviews in Biotechnology. 34 (1): 77–88. doi:10.3109/07388551.2013.823595. PMID 24041244. Archived from the original (PDF) on 17 September 2016. Retrieved 2 January 2019.
- ↑ "State of Food and Agriculture 2003–2004. Agricultural Biotechnology: Meeting the Needs of the Poor. Health and environmental impacts of transgenic crops". Food and Agriculture Organization of the United Nations. Archived from the original on 9 January 2019. Retrieved 8 February 2016.
- ↑ National Academies Of Sciences, Engineering; Division on Earth Life Studies; Board on Agriculture Natural Resources; Committee on Genetically Engineered Crops: Past Experience Future Prospects (2016). Genetically Engineered Crops: Experiences and Prospects. The National Academies of Sciences, Engineering, and Medicine (US). p. 149. doi:10.17226/23395. ISBN 978-0-309-43738-7. PMID 28230933. Archived from the original on 25 August 2019. Retrieved 19 May 2016.
- ↑ Bucchini L, Goldman LR (2002). "Starlink corn: a risk analysis". Environ. Health Perspect. 110 (1): 5–13. doi:10.1289/ehp.021105. PMC 1240687. PMID 11781159.
- ↑ Wen H, Kwon J (2016). "Food Allergy Risk Communication in Restaurants" (PDF). Food Protection Trends. 35 (5): 372–383. Archived (PDF) from the original on 18 January 2021. Retrieved 22 July 2020.
- 1 2 3 4 Hadley, Caroline (November 2006). "Food allergies on the rise? Determining the prevalence of food allergies, and how quickly it is increasing, is the first step in tackling the problem". EMBO Reports. 7 (11): 1080–1083. doi:10.1038/sj.embor.7400846. ISSN 1469-221X. PMC 1679775. PMID 17077863.
- ↑ Nowak-Węgrzyn A, Sampson HA (March 2011). "Future therapies for food allergies". J. Allergy Clin. Immunol. 127 (3): 558–73, quiz 574–5. doi:10.1016/j.jaci.2010.12.1098. PMC 3066474. PMID 21277625.
- 1 2 Best KP, Gold M, Kennedy D, et al. (2016). "Omega-3 long-chain PUFA intake during pregnancy and allergic disease outcomes in the offspring: a systematic review and meta-analysis of observational studies and randomized controlled trials". Am. J. Clin. Nutr. 103 (1): 128–143. doi:10.3945/ajcn.115.111104. PMID 26675770.
- 1 2 3 Gunaratne AW, Makrides M, Collins CT (2015). "Maternal prenatal and/or postnatal n-3 long chain polyunsaturated fatty acids (LCPUFA) supplementation for preventing allergies in early childhood". Cochrane Database Syst Rev (7): CD010085. doi:10.1002/14651858.CD010085.pub2. PMID 26197477.
- ↑ Waidyatillake NT, Dharmage SC, Allen KJ, et al. (2018). "Association of breast milk fatty acids with allergic disease outcomes-A systematic review". Allergy. 73 (2): 295–312. doi:10.1111/all.13300. PMID 28869762.
- ↑ Schindler, Tim; Sinn, John Kh; Osborn, David A. (28 October 2016). "Polyunsaturated fatty acid supplementation in infancy for the prevention of allergy". The Cochrane Database of Systematic Reviews. 10: CD010112. doi:10.1002/14651858.CD010112.pub2. ISSN 1469-493X. PMC 6464137. PMID 27788565.
- ↑ Chang YS, Trivedi MK, Jha A, et al. (2016). "Synbiotics for Prevention and Treatment of Atopic Dermatitis: A Meta-analysis of Randomized Clinical Trials". JAMA Pediatr. 170 (3): 236–242. doi:10.1001/jamapediatrics.2015.3943. PMID 26810481.
- 1 2 Cuello-Garcia CA, Brożek JL, Fiocchi A, et al. (2015). "Probiotics for the prevention of allergy: A systematic review and meta-analysis of randomized controlled trials". J. Allergy Clin. Immunol. 136 (4): 952–961. doi:10.1016/j.jaci.2015.04.031. PMID 26044853.
- 1 2 Osborn DA, Sinn JK (2013). "Prebiotics in infants for prevention of allergy". Cochrane Database Syst Rev (3): CD006474. doi:10.1002/14651858.CD006474.pub3. PMID 23543544.
- ↑ Zuccotti G, Meneghin F, Aceti A, et al. (2015). "Probiotics for prevention of atopic diseases in infants: systematic review and meta-analysis". Allergy. 70 (11): 1356–1371. doi:10.1111/all.12700. PMID 26198702.
- ↑ Zhang GQ, Hu HJ, Liu CY, et al. (2016). "Probiotics for Prevention of Atopy and Food Hypersensitivity in Early Childhood: A PRISMA-Compliant Systematic Review and Meta-Analysis of Randomized Controlled Trials". Medicine (Baltimore). 95 (8): e2562. doi:10.1097/MD.0000000000002562. PMC 4778993. PMID 26937896.
- ↑ de Silva D, Geromi M, Panesar SS, et al. (2014). "Acute and long-term management of food allergy: systematic review". Allergy. 69 (2): 159–167. doi:10.1111/all.12314. PMID 24215577.
- Notes
- Nester, Eugene W.; Anderson, Denise G.; Roberts Jr, C. Evans; Nester, Martha T. (2009). "Immunologic Disorders". Microbiology: A Human Perspective (6th ed.). New York: McGraw-Hill. pp. 414–428.
- Sicherer, Scott H. (2006). Understanding and Managing Your Child's Food Allergy. Baltimore: Johns Hopkins University Press.
External links
| Classification | |
|---|---|
| External resources |
- Food Allergy Archived 31 March 2015 at the Wayback Machine, Merck Manual
- "Food Allergies and Intolerances Resource List for Consumers" (PDF). Food and Nutrition Information Center, National Agricultural Library. December 2010. Archived from the original (PDF) on 6 August 2011. Retrieved 15 August 2011. – a collection of resources on the topic of food allergies and intolerances
- "Food Allergy". MedlinePlus. U.S. National Library of Medicine. Archived from the original on 29 July 2020. Retrieved 22 July 2020.
Food science | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| General |
| ||||||||||
| Food industry |
| ||||||||||
| Food politics |
| ||||||||||
| Institutions |
| ||||||||||