Plantar fasciitis
| Plantar fasciitis | |
|---|---|
| Other names: Plantar fasciosis, plantar fasciopathy, jogger's heel, heel spur syndrome[1] | |
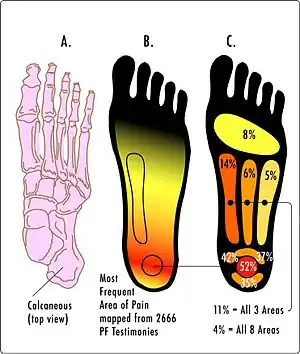 | |
| Most common areas of pain in plantar fasciitis | |
| Specialty | Orthopedics, sports medicine, podiatry |
| Symptoms | Pain in the heel and bottom of the foot[2] |
| Usual onset | Gradual[3] |
| Causes | Unclear[2] |
| Risk factors | Overuse (long periods of standing), obesity, inward rolling of the foot[2][4] |
| Diagnostic method | Based on symptoms, ultrasound[2] |
| Differential diagnosis | Osteoarthritis, ankylosing spondylitis, heel pad syndrome, reactive arthritis[5][6] |
| Treatment | Conservative management[4][7] |
| Frequency | ~4%[2][5] |
Plantar fasciitis is a disorder of the connective tissue which supports the arch of the foot.[2] It results in pain in the heel and bottom of the foot that is usually most severe with the first steps of the day or following a period of rest.[2][4] Pain is also frequently brought on by bending the foot and toes up towards the shin.[3][4] The pain typically comes on gradually, and it affects both feet in about one-third of cases.[2][3]
The cause of plantar fasciitis is not entirely clear.[2] Risk factors include overuse, such as from long periods of standing, an increase in exercise, and obesity.[2][4] It is also associated with inward rolling of the foot, a tight Achilles tendon, and a sedentary lifestyle.[2][4] It is unclear if heel spurs have a role in causing plantar fasciitis even though they are commonly present in people who have the condition.[2] Plantar fasciitis is a disorder of the insertion site of the ligament on the bone characterized by micro tears, breakdown of collagen, and scarring.[2] Since inflammation plays either a lesser or no role, a review proposed it be renamed plantar fasciosis.[2][8] The presentation of the symptoms is generally the basis for diagnosis; with ultrasound sometimes being useful if there is uncertainty.[2] Other conditions with similar symptoms include osteoarthritis, ankylosing spondylitis, heel pad syndrome, and reactive arthritis.[5][6]
Most cases of plantar fasciitis resolve with time and conservative methods of treatment.[4][7] For the first few weeks, those affected are usually advised to rest, change their activities, take pain medications, and stretch.[4] If this is not sufficient, physiotherapy, orthotics, splinting, or steroid injections may be options.[4] If these measures are not effective, additional measures may include extracorporeal shockwave therapy or surgery.[4]
Between 4% and 7% of the general population has heel pain at any given time: about 80% of these are due to plantar fasciitis.[2][5] Approximately 10% of people have the disorder at some point during their life.[9] It becomes more common with age.[2] It is unclear if one sex is more affected than the other.[2]
Signs and symptoms
When plantar fasciitis occurs, the pain is typically sharp[10] and usually unilateral (70% of cases).[7] Bearing weight on the heel after long periods of rest worsens heel pain in affected individuals.[11] Individuals with plantar fasciitis often report their symptoms are most intense during their first steps after getting out of bed or after prolonged periods of sitting.[4] Symptoms typically improve with continued walking.[4][6][10] Rare, but reported symptoms include numbness, tingling, swelling, or radiating pain.[12] Typically there are no fevers or night sweats.[3]
If the plantar fascia is overused in the setting of plantar fasciitis, the plantar fascia can rupture. Typical signs and symptoms of plantar fascia rupture include a clicking or snapping sound, significant local swelling, and acute pain in the bottom of the foot.[10]
Risk factors
Identified risk factors for plantar fasciitis include excessive running, standing on hard surfaces for prolonged periods, high arches of the feet, the presence of a leg length inequality, and flat feet. The tendency of flat feet to excessively roll inward during walking or running makes them more susceptible to plantar fasciitis.[4][11][13] Obesity is seen in 70% of individuals who present with plantar fasciitis and is an independent risk factor.[3]
Plantar fasciitis is commonly a result of some biomechanical imbalance that causes an increased amount of tension placed along the plantar fascia.[14]
Studies consistently find a strong association between increased body mass index and plantar fasciitis in the non-athletic population. This association between weight and plantar fasciitis is not present in the athletic population.[7] Achilles tendon tightness and inappropriate footwear have also been identified as significant risk factors.[15]
Pathophysiology
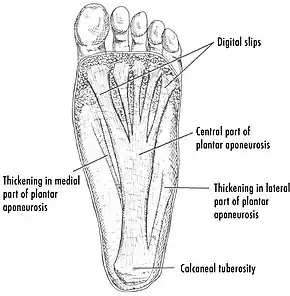
The cause of plantar fasciitis is poorly understood and appears to have several contributing factors.[15] The plantar fascia is a thick fibrous band of connective tissue that originates from the medial tubercle and anterior aspect of the heel bone. From there, the fascia extends along the sole of the foot before inserting at the base of the toes and supports the arch of the foot.[3][11][13]
Plantar fasciitis is a non-inflammatory condition of the plantar fascia. Within the last decade, studies have observed microscopic anatomical changes indicating that plantar fasciitis is due to a non-inflammatory structural breakdown of the plantar fascia rather than an inflammatory process.[7][15]
Many in the academic community have stated the condition should be renamed plantar fasciosis in light of these newer findings.[6] Repetitive microtrauma (small tears) appears to cause a structural breakdown of the plantar fascia.[12][13] Microscopic examination of the plantar fascia often shows myxomatous degeneration, connective tissue calcium deposits, and disorganized collagen fibers.[8]
Disruptions in the plantar fascia's normal mechanical movement during standing and walking (known as the Windlass mechanism) place excess strain on the calcaneal tuberosity and seem to contribute to the development of plantar fasciitis.[15] Other studies have also suggested that plantar fasciitis is not due to inflamed plantar fascia, but may be a tendon injury involving the flexor digitorum brevis muscle located immediately deep to the plantar fascia.[13]
Diagnosis
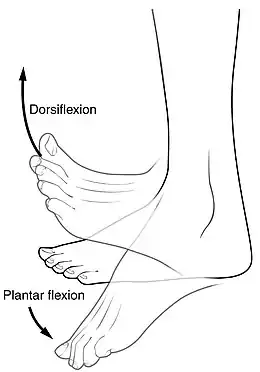
Plantar fasciitis is usually diagnosed by a health care provider after consideration of a person's presenting history, risk factors, and clinical examination.[4][16][17] Palpation along the inner aspect of the heel bone on the sole may elicit tenderness during the physical examination.[4][11] The foot may have limited dorsiflexion due to excessive tightness of the calf muscles or the Achilles tendon.[7] Dorsiflexion of the foot may elicit the pain due to stretching of the plantar fascia with this motion.[4][12] Diagnostic imaging studies are not usually needed to diagnose plantar fasciitis.[7] Occasionally, a physician may decide imaging studies (such as X-rays, diagnostic ultrasound, or MRI) are warranted to rule out serious causes of foot pain.
Other diagnoses that are typically considered include fractures, tumors, or systemic disease if plantar fasciitis pain fails to respond appropriately to conservative medical treatments.[4][11] Bilateral heel pain or heel pain in the context of a systemic illness may indicate a need for a more in-depth diagnostic investigation. Under these circumstances, diagnostic tests such as a CBC or serological markers of inflammation, infection, or autoimmune disease such as C-reactive protein, erythrocyte sedimentation rate, anti-nuclear antibodies, rheumatoid factor, HLA-B27, uric acid, or Lyme disease antibodies may also be obtained.[5] Neurological deficits may prompt an investigation with electromyography to check for damage to the nerves or muscles.[12]
An incidental finding associated with this condition is a heel spur, a small bony calcification on the calcaneus (heel bone), which can be found in up to 50% of those with plantar fasciitis.[6] In such cases, it is the underlying plantar fasciitis that produces the heel pain, and not the spur itself.[13] The condition is responsible for the creation of the spur though the clinical significance of heel spurs in plantar fasciitis remains unclear.[12]
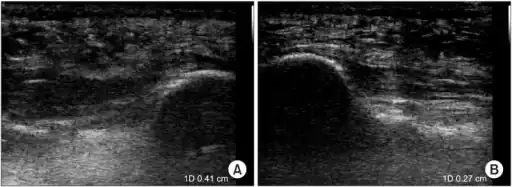 a)Ultrasonographic finding of plantar fasciitis b)normal sonographic finding
a)Ultrasonographic finding of plantar fasciitis b)normal sonographic finding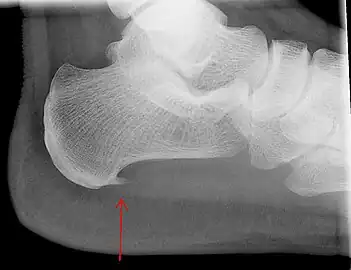 Heel bone with heel spur
Heel bone with heel spur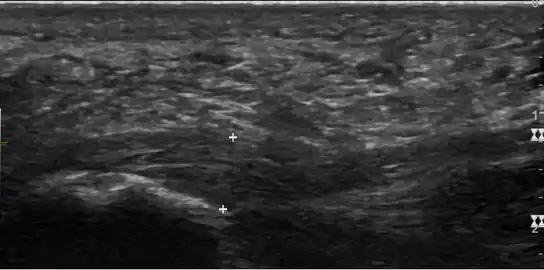 Thickened plantar fascia in ultrasound
Thickened plantar fascia in ultrasound
Imaging
Medical imaging is not routinely needed. It is expensive and does not typically change how plantar fasciitis is managed.[15] When the diagnosis is not clinically apparent, lateral view X-rays of the ankle are the recommended imaging modality to assess for other causes of heel pain, such as stress fractures or bone spur development.[7]
The plantar fascia has three fascicles-the central fascicle being the thickest at 4 mm, the lateral fascicle at 2 mm, and the medial less than a millimeter thick.[18] In theory, plantar fasciitis becomes more likely as the plantar fascia's thickness at the calcaneal insertion increases. A thickness of more than 4.5 mm ultrasound and 4 mm on MRI are useful for diagnosis.[19] Other imaging findings, such as thickening of the plantar aponeurosis, are nonspecific and have limited usefulness in diagnosing plantar fasciitis.[13]
3-phase bone scan is a sensitive modality to detect active plantar fasciitis. Furthermore, a 3-phase bone scan can be used to monitor response to therapy, as demonstrated by decreased uptake after corticosteroid injections.[20]
Differential diagnosis
The differential diagnosis for heel pain is extensive and includes pathological entities including, but not limited to, the following: calcaneal stress fracture, calcaneal bursitis, osteoarthritis, spinal stenosis involving the nerve roots of lumbar spinal nerve 5 (L5) or sacral spinal nerve 1 (S1), calcaneal fat pad syndrome, hypothyroidism, seronegative spondyloparthopathies such as reactive arthritis, ankylosing spondylitis, or rheumatoid arthritis (more likely if pain is present in both heels),[5] plantar fascia rupture, and compression neuropathies such as tarsal tunnel syndrome or impingement of the medial calcaneal nerve.[3][5][7]
A determination about a diagnosis of plantar fasciitis can usually be made based on a person's medical history and physical examination.[21] When a physician suspects a fracture, infection, or some other serious underlying condition, they may order an X-ray to investigate.[21] X-rays are unnecessary to screen for plantar fasciitis for people who stand or walk a lot at work unless imaging is otherwise indicated.[21]
Treatment
Non-surgical

About 90% of plantar fasciitis cases improve within six months with conservative treatment,[9] and within a year regardless of treatment.[4][7] Affected people use many treatments for plantar fasciitis. Most have little evidence to support their use and are not adequately studied.[4] First-line conservative approaches include rest, massage, heat, ice, and calf-strengthening exercises; techniques to stretch the calf muscles, Achilles tendon, and plantar fascia; weight reduction in the overweight or obese; and nonsteroidal anti-inflammatory drugs (NSAIDs) such as aspirin or ibuprofen.[6][11][23] The use of NSAIDs to treat plantar fasciitis is common, but their use fails to resolve the pain in 20% of people.[11]
If plantar fasciitis fails to respond to conservative treatment for at least three months, then extracorporeal shockwave therapy (ESWT) may be considered. Evidence from meta-analyses suggests significant pain relief lasts up to one year after the procedure.[9][24] However, debate about the therapy's efficacy has persisted.[8] ESWT is performed with or without anesthesia though studies suggest giving anesthesia diminishes the procedure's effectiveness.[25] Complications from ESWT are rare and typically benign when present.[25] Known complications of ESWT include the development of a mild hematoma or an ecchymosis, redness around the site of the procedure, or migraine.[25]
Corticosteroid injections are sometimes used for cases of plantar fasciitis refractory to more conservative measures. There is tentative evidence that injected corticosteroids are effective for short-term pain relief up to one month, but not after that.[26]
Orthotic devices and specific taping techniques may reduce pronation of the foot and therefore reduce load on the plantar fascia resulting in pain improvement.[13] The evidence to support the use of foot orthoses is mixed, with some suggesting short-term pain relief up to three months and others failing to confirm this benefit.[27][28] The long-term effectiveness of custom orthotics for plantar fasciitis pain reduction requires additional study.[29]
Another treatment technique is known as plantar iontophoresis. This technique involves applying anti-inflammatory substances such as dexamethasone or acetic acid topically to the foot and transmitting these substances through the skin with an electric current.[11] Some evidence supports the use of night splints for 1–3 months to relieve plantar fasciitis pain that has persisted for six months.[7] The night splints are designed to position and maintain the ankle in a neutral position, thereby passively stretching the calf and plantar fascia during sleep.[7]
Surgery
Plantar fasciotomy is a surgical treatment and the last resort for refractory plantar fasciitis pain. If plantar fasciitis does not resolve after six months of conservative treatment, then the procedure is considered as a last resort.[4][6] Minimally invasive and endoscopic approaches to plantar fasciotomy exist but require a specialist who is familiar with specific equipment. The availability of these surgical techniques is limited as of 2012.[5] A 2012 study found 76% of people who underwent endoscopic plantar fasciotomy had complete relief of their symptoms and had few complications (level IV evidence).[8] Heel spur removal during plantar fasciotomy does not appear to improve the surgical outcome.[30]
Plantar heel pain may occur for multiple reasons. In select cases, surgeons may perform a release of the lateral plantar nerve alongside the plantar fasciotomy.[5][30] Possible complications of plantar fasciotomy include nerve injury, instability of the medial longitudinal arch of the foot,[31] fracture of the calcaneus, prolonged recovery time, infection, rupture of the plantar fascia, and failure to improve the pain.[4] Coblation surgery has recently been proposed as an alternative surgical approach for the treatment of recalcitrant plantar fasciitis.[30]
Epidemiology
Plantar fasciitis is the most common type of plantar fascia injury[10] and is the most common reason for heel pain, responsible for 80% of cases. The condition tends to occur more often in women, military recruits, older athletes, dancers,[1] the obese, and young male athletes.[7][12][13]
Plantar fasciitis is estimated to affect 1 in 10 people at some point during their lifetime and most commonly affects people between 40–60 years of age.[3][8] In the United States alone, more than two million people receive treatment for plantar fasciitis.[3] The cost of treating plantar fasciitis in the United States is estimated to be $284 million each year.[3]
Research
Botulinum toxin A injections as well as similar techniques such as platelet-rich plasma injections and prolotherapy remain controversial.[7][8][11][32]
Dry needling is also being researched for treatment of plantar fasciitis.[33] A systematic review of available research found limited evidence of effectiveness for this technique.[34] The studies were reported to be inadequate in quality and too diverse in methodology to enable reaching a firm conclusion.[34]
References
- 1 2 Toronto Notes 2017: Comprehensive Medical Reference and Review for the Medical Council of Canada Qualifying Exam Part I and the United States Medical Licensing Exam Step 2. Toronto Notes for Medical Students Incorporated. 12 June 2019. ISBN 9781927363348. Archived from the original on 28 August 2021. Retrieved 12 June 2019 – via Google Books.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 Beeson P (September 2014). "Plantar fasciopathy: revisiting the risk factors" (PDF). Foot and Ankle Surgery. 20 (3): 160–5. doi:10.1016/j.fas.2014.03.003. PMID 25103701. Archived from the original (PDF) on 2018-07-06. Retrieved 2019-06-22.
- 1 2 3 4 5 6 7 8 9 10 Rosenbaum AJ, DiPreta JA, Misener D (March 2014). "Plantar heel pain". The Medical Clinics of North America. 98 (2): 339–52. doi:10.1016/j.mcna.2013.10.009. PMID 24559879.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 Goff JD, Crawford R (September 2011). "Diagnosis and treatment of plantar fasciitis". American Family Physician. 84 (6): 676–82. PMID 21916393. Archived from the original on 2013-12-30.
- 1 2 3 4 5 6 7 8 9 Cutts S, Obi N, Pasapula C, Chan W (November 2012). "Plantar fasciitis". Annals of the Royal College of Surgeons of England. 94 (8): 539–42. doi:10.1308/003588412X13171221592456. PMC 3954277. PMID 23131221.
- 1 2 3 4 5 6 7 Tu P, Bytomski JR (October 2011). "Diagnosis of heel pain". American Family Physician. 84 (8): 909–16. PMID 22010770. Archived from the original on 2013-12-30.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Tahririan MA, Motififard M, Tahmasebi MN, Siavashi B (August 2012). "Plantar fasciitis". Journal of Research in Medical Sciences. 17 (8): 799–804. PMC 3687890. PMID 23798950.
- 1 2 3 4 5 6 Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW (June 2014). "Plantar and medial heel pain: diagnosis and management". The Journal of the American Academy of Orthopaedic Surgeons. 22 (6): 372–80. doi:10.5435/JAAOS-22-06-372. PMID 24860133.
- 1 2 3 Zhiyun L, Tao J, Zengwu S (July 2013). "Meta-analysis of high-energy extracorporeal shock wave therapy in recalcitrant plantar fasciitis". Swiss Medical Weekly. 143: w13825. doi:10.4414/smw.2013.13825. PMID 23832373.
- 1 2 3 4 Jeswani T, Morlese J, McNally EG (September 2009). "Getting to the heel of the problem: plantar fascia lesions". Clinical Radiology. 64 (9): 931–9. doi:10.1016/j.crad.2009.02.020. PMID 19664484.
- 1 2 3 4 5 6 7 8 9 Molloy LA (November 2012). "Managing chronic plantar fasciitis: when conservative strategies fail". JAAPA. 25 (11): 48, 50, 52–3. doi:10.1097/01720610-201211000-00009. PMID 23620924.
- 1 2 3 4 5 6 Monto RR (December 2013). "Platelet-rich plasma and plantar fasciitis". Sports Medicine and Arthroscopy Review. 21 (4): 220–4. doi:10.1097/JSA.0b013e318297fa8d. PMID 24212370. Archived from the original on 2021-08-28. Retrieved 2020-01-11.
- 1 2 3 4 5 6 7 8 Orchard J (October 2012). "Plantar fasciitis". BMJ. 345: e6603. doi:10.1136/bmj.e6603. PMID 23054045. Archived from the original on 2021-08-28. Retrieved 2020-01-11.
- ↑ BARRETT, STEPHEN (April 15, 1999). "Plantar Fasciitis and Other Causes of Heel Pain". American Family Physician. 59 (8): 2200–2206. PMID 10221305. Archived from the original on 15 April 2019. Retrieved 15 April 2019.
- 1 2 3 4 5 Yin MC, Ye J, Yao M, Cui XJ, Xia Y, Shen QX, Tong ZY, Wu XQ, Ma JM, Mo W (August 2014). "Is extracorporeal shock wave therapy clinical efficacy for relief of chronic, recalcitrant plantar fasciitis? A systematic review and meta-analysis of randomized placebo or active-treatment controlled trials". Archives of Physical Medicine and Rehabilitation. 95 (8): 1585–93. doi:10.1016/j.apmr.2014.01.033. PMID 24662810.
- ↑ Buchbinder R (May 2004). "Clinical practice. Plantar fasciitis". The New England Journal of Medicine. 350 (21): 2159–66. doi:10.1056/NEJMcp032745. PMID 15152061.
- ↑ Cole C, Seto C, Gazewood J (December 2005). "Plantar fasciitis: evidence-based review of diagnosis and therapy". American Family Physician. 72 (11): 2237–42. PMID 16342847. Archived from the original on 2014-07-14.
- ↑ Ehrmann C, Maier M, Mengiardi B, Pfirrmann CW, Sutter R (September 2014). "Calcaneal attachment of the plantar fascia: MR findings in asymptomatic volunteers". Radiology. 272 (3): 807–14. doi:10.1148/radiol.14131410. PMID 24814176.
- ↑ League AC (March 2008). "Current concepts review: plantar fasciitis". Foot & Ankle International. 29 (3): 358–66. doi:10.3113/fai.2008.0358. PMID 18348838.
- ↑ Pelletier-Galarneau M, Martineau P, Gaudreault M, Pham X (2015). "Review of running injuries of the foot and ankle: clinical presentation and SPECT-CT imaging patterns". American Journal of Nuclear Medicine and Molecular Imaging. 5 (4): 305–16. PMC 4529586. PMID 26269770.
- 1 2 3 American College of Occupational and Environmental Medicine (February 2014), "Five Things Physicians and Patients Should Question", Choosing Wisely: an initiative of the ABIM Foundation, American College of Occupational and Environmental Medicine, archived from the original on 11 September 2014, retrieved 24 February 2014, which cites
- Haas N, Beecher P, Easly M, et al. (2011). "Ankle and foot disorders". In Hegmann KT (ed.). Occupational medicine practice guidelines : evaluation and management of common health problems and functional recovery in workers (3rd ed.). Elk Grove Village, IL: American College of Occupational and Environmental Medicine. p. 1182. ISBN 978-0615452272.
- ↑ Lim AT, How CH, Tan B (April 2016). "Management of plantar fasciitis in the outpatient setting". Singapore Medical Journal. 57 (4): 168–70, quiz 171. doi:10.11622/smedj.2016069. PMC 4853481. PMID 27075037.
- ↑ "Plantar Fasciitis and Bone Spurs". American Academy of Orthopaedic Surgeons. 2010. Archived from the original on 16 June 2014. Retrieved 24 June 2014.
- ↑ Aqil A, Siddiqui MR, Solan M, Redfern DJ, Gulati V, Cobb JP (November 2013). "Extracorporeal shock wave therapy is effective in treating chronic plantar fasciitis: a meta-analysis of RCTs". Clinical Orthopaedics and Related Research. 471 (11): 3645–52. doi:10.1007/s11999-013-3132-2. PMC 3792262. PMID 23813184.
- 1 2 3 Wang CJ (March 2012). "Extracorporeal shockwave therapy in musculoskeletal disorders". Journal of Orthopaedic Surgery and Research. 7 (1): 11. doi:10.1186/1749-799X-7-11. PMC 3342893. PMID 22433113.
- ↑ David JA, Sankarapandian V, Christopher PR, Chatterjee A, Macaden AS (June 2017). "Injected corticosteroids for treating plantar heel pain in adults". The Cochrane Database of Systematic Reviews. 6: CD009348. doi:10.1002/14651858.CD009348.pub2. PMC 6481652. PMID 28602048.
- ↑ Lee SY, McKeon P, Hertel J (February 2009). "Does the use of orthoses improve self-reported pain and function measures in patients with plantar fasciitis? A meta-analysis". Physical Therapy in Sport. 10 (1): 12–8. doi:10.1016/j.ptsp.2008.09.002. PMID 19218074.
- ↑ Hawke, F; Burns, J; Radford, JA; du Toit, V (16 July 2008). "Custom-made foot orthoses for the treatment of foot pain". The Cochrane Database of Systematic Reviews (3): CD006801. doi:10.1002/14651858.CD006801.pub2. PMID 18646168.
- ↑ Anderson J, Stanek J (May 2013). "Effect of foot orthoses as treatment for plantar fasciitis or heel pain". Journal of Sport Rehabilitation. 22 (2): 130–6. doi:10.1123/jsr.22.2.130. PMID 23037146.
- 1 2 3 Thomas JL, Christensen JC, Kravitz SR, Mendicino RW, Schuberth JM, Vanore JV, Weil LS, Zlotoff HJ, Bouché R, Baker J (May–June 2010). "The diagnosis and treatment of heel pain: a clinical practice guideline-revision 2010". The Journal of Foot and Ankle Surgery. 49 (3 Suppl): S1–19. doi:10.1053/j.jfas.2010.01.001. PMID 20439021.
- ↑ Tweed JL, Barnes MR, Allen MJ, Campbell JA (September–October 2009). "Biomechanical consequences of total plantar fasciotomy: a review of the literature". Journal of the American Podiatric Medical Association. 99 (5): 422–30. doi:10.7547/0990422. PMID 19767549.
- ↑ Monto RR (April 2014). "Platelet-rich plasma efficacy versus corticosteroid injection treatment for chronic severe plantar fasciitis". Foot & Ankle International. 35 (4): 313–8. doi:10.1177/1071100713519778. PMID 24419823.
- ↑ Cotchett MP, Landorf KB, Munteanu SE, Raspovic A (January 2011). "Effectiveness of trigger point dry needling for plantar heel pain: study protocol for a randomised controlled trial". Journal of Foot and Ankle Research. 4 (1): 5. doi:10.1186/1757-1146-4-5. PMC 3035595. PMID 21255460.
- 1 2 Cotchett MP, Landorf KB, Munteanu SE (September 2010). "Effectiveness of dry needling and injections of myofascial trigger points associated with plantar heel pain: a systematic review". Journal of Foot and Ankle Research. 3 (1): 18. doi:10.1186/1757-1146-3-18. PMC 2942821. PMID 20807448.
External links
| Classification | |
|---|---|
| External resources |
- "Plantar fasciitis and bone spurs". American Academy of Orthopedic Surgeons. Archived from the original on 2014-06-16. Retrieved 2014-05-20.