Septal myectomy
| Septal myectomy | |
|---|---|
 | |
| Hypertrophic cardiomyopathy | |
| Specialty | Cardiology |
| Indications | Hypertrophic cardiomyopathy[1] |
| Complications | Injury to the septum or nearby structures, heart block[1] |
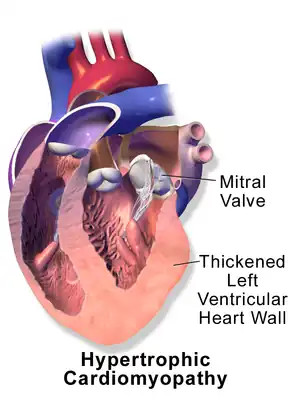
Septal myectomy is a heart surgery to treat hypertrophic cardiomyopathy (HCM).[1] It is performed via a median sternotomy, and entails removing a portion of the septum that is obstructing the flow of blood from the left ventricle to the aorta.[2]
It is typically considered when symptoms persist despite treatment with medication (usually beta, verapamil or disopyramide).[1] Non-surgical thinning of tissue with alcohol ablation is an alternative, particularly if there are other co-existing diseases or poor health that may render heart surgery unsafe.[1]
Complications include injury to the septum or nearby structures and heart block.[1]
The procedure is effective, with 80% to 90% having improved symptoms or no symptoms.[1] Long-term survival is equivalent to that of the general population, and superior to obstructive HCM without operation.[1]
Septal myectomy was established by Andrew G. Morrow in the 1960s.[3]
Technique
Following anaesthesia, a transthoracic echocardiogram is performed to take measurements of the heart and to assess the mitral valve and septum, before performing a median sternotomy.[1] Central aortic cannulation and a single, 2-stage venous return cannula is performed with normothermic cardiopulmonary bypass.[1]
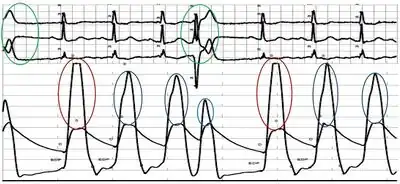
After the placement of the aortic inflow cannula, intracardiac pressure is measured using two 22 gauge needles; one placed in the aorta near the aortic cannula and another inserted through the right ventricular free wall and septum into the left ventricle (LV).[1] Both LV and aortic pressures are monitored at the same time.[1] The Brockenbrough-Braunwald-Morrow sign is recorded by eliciting a premature ventricular contraction.[1] A small dose of isoproterenol may be required to provoke a gradient.[1] Cardiopulmonary bypass is commenced after pressures are recorded, the aorta cross-clamped and the heart is arrested with cold-blood via the aortic needle.[1] Usually a proportion of the thickened septum is cut after being visualised through the aortic valve via a cut in the aorta.[1]
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Cui, Hao; Schaff, Hartzell V. (2020). "80. Hypertrophic cardiomyopathy". In Raja, Shahzad G. (ed.). Cardiac Surgery: A Complete Guide. Switzerland: Springer. pp. 735–748. ISBN 978-3-030-24176-6. Archived from the original on 2022-10-13. Retrieved 2022-10-13.
- ↑ Ralph-Edwards, Anthony; Vanderlaan, Rachel D.; Bajona, Pietro (July 2017). "Transaortic septal myectomy: techniques and pitfalls". Annals of Cardiothoracic Surgery. 6 (4): 410–415. doi:10.21037/acs.2017.07.08. ISSN 2225-319X. PMID 28944183. Archived from the original on 2022-10-13. Retrieved 2022-10-13.
- ↑ "History of Changes for Study: NCT04603521". clinicaltrials.gov. Archived from the original on 30 October 2022. Retrieved 30 October 2022.