Bacterial tracheitis
| Bacterial tracheitis | |
|---|---|
| Other names: Tracheitis, inflammation of the trachea, membranous laryngotracheobronchitis, exudative tracheitis[1][2] | |
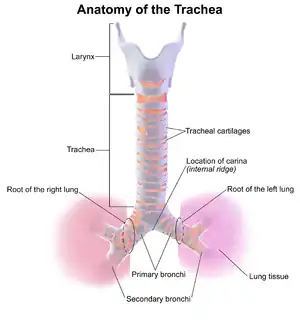 | |
| Anatomy of the trachea | |
| Specialty | Pediatrics, ENT surgery |
| Symptoms | Stridor, fever, productive cough, pain[2] |
| Complications | Airway obstruction, tracheal stenosis[2] |
| Risk factors | Following viral upper respiratory infections, endotracheal intubation, tracheostomy, poor immune function[2][3] |
| Diagnostic method | Based on symptoms[3] |
| Differential diagnosis | Epiglottitis, croup, candidiasis, diphtheria, retropharyngeal abscess, viral laryngitis[2] |
| Treatment | Antibiotics, endotracheal intubation[3] |
| Frequency | Rare[3] |
Bacterial tracheitis is a bacterial infection of the trachea.[1] Symptoms may include stridor, fever, productive cough, and pain.[2] Complications can include airway obstruction or tracheal stenosis.[2]
It may occur following croup or other viral upper respiratory infections.[2][3] Other risk factors include endotracheal intubation, tracheostomy, and poor immune function.[2][3] The bacterial most commonly involved include Staphylococcus aureus and streptococci.[3] Diagnosis is suspected based on symptoms and may be confirmed by bronchoscopy or X-rays.[3]
Treatment involves antibiotics and occasionally endotracheal intubation.[3] Antibiotics that may be used include ceftriaxone with vancomycin or amoxicillin/clavulanate.[2] Inhaled epinephrine is not useful.[2] While outcomes with treatment are generally good, people may still die as a result.[2]
Bacterial tracheitis is rare, affecting about 1 to 10 per million children per year.[3][2] It most commonly affects young children between the age of 3 and 8 years old.[2] Males may be more commonly affected than females.[2] It occurs more commonly in the fall and winter.[2] The condition was first described in the 1920s.[2]
Signs and symptoms
- Increasing deep or barking croup cough following a recent upper respiratory infection
- Crowing sound when inhaling (inspiratory stridor)
- 'Scratchy' feeling in the throat
- Chest pain
- Fever
- Ear ache
- Headache
- Dizziness (light headed)
- Labored breathing
Causes
Bacterial tracheitis is a bacterial infection of the trachea and is capable of producing airway obstruction.
One of the most common causes is Staphylococcus aureus and often follows a recent viral upper respiratory infection. Bacterial tracheitis is a rare complication of influenza infection.[4] It is the most serious in young children, possibly because of the relatively small size of the trachea that gets easily blocked by swelling. The most frequent sign is the rapid development of stridor. It is occasionally confused with croup. If it is inflamed, a condition known as tracheitis can occur. In this condition there can be inflammation of the linings of the trachea. A condition called tracheo-bronchitis can be caused, when the mucous membrane of the trachea and bronchi swell. A collapsed trachea is formed as a result of defect in the cartilage, that makes the cartilage unable to support the trachea and results in dry hacking cough. In this condition there can be inflammation of the linings of the trachea. If the connective nerve tissues in the trachea degenerate it causes tracheomalacia. Infections to the trachea can cause tracheomegaly.
Diagnosis

The diagnosis of tracheitis requires the direct vision of exudates or pseudomembranes on the trachea. X-ray findings may include subglottic narrowing. The priority is to secure the patient's airway, and to rule out croup and epiglottitis which may be fatal. Suspicion for tracheitis should be high in cases of onset of airway obstruction that do not respond to racemic epinephrine.
Although the trachea is considered part of the lower respiratory tract,[6] it is classified under "acute upper respiratory infections".[7]
Treatment
In more severe cases, it is treated by administering intravenous antibiotics and may require admission to an intensive care unit (ICU) for intubation and supportive ventilation if the airway swelling is severe. During an intensive care admission, various methods of invasive and non-invasive monitoring may be required, which may include ECG monitoring, oxygen saturation, capnography and arterial blood pressure monitoring.
References
- 1 2 "Bacterial Tracheitis". www.dynamed.com. Archived from the original on 22 November 2021. Retrieved 29 April 2022.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Burton, LV; Lofgren, DH; Silberman, M (January 2022). "Bacterial Tracheitis". PMID 29262085.
{{cite journal}}: Cite journal requires|journal=(help) - 1 2 3 4 5 6 7 8 9 10 "Bacterial Tracheitis - Children's Health Issues". MSD Manual Consumer Version. Archived from the original on 7 August 2021. Retrieved 29 April 2022.
- ↑ medicine, s cecil. Goldman (24th ed.). Philadelphia: Elsevier Saunders. p. 1326. ISBN 978-1-4377-2788-3.
- ↑ "Bacterial Tracheitis | Pediatric Radiology Reference Article | Pediatric Imaging | @pedsimaging". Pediatric Imaging. 20 June 2019. Archived from the original on 17 June 2021. Retrieved 29 April 2022.
- ↑ Patwa, Apeksh; Shah, Amit (September 2015). "Anatomy and physiology of respiratory system relevant to anaesthesia". Indian Journal of Anaesthesia. 59 (9): 533–541. doi:10.4103/0019-5049.165849. ISSN 0019-5049. PMC 4613399. PMID 26556911.
- ↑ "J04.1 Acute tracheitis". ICD-10 Version. 2014. Archived from the original on 2021-03-09. Retrieved 2020-08-08.
External links
| Classification | |
|---|---|
| External resources |