Peritonsillar abscess
| Peritonsillar abscess | |
|---|---|
| Other names: Quinsy, quinsey | |
 | |
| Right sided peritonsillar abscess | |
| Specialty | Otorhinolaryngology |
| Symptoms | Fever, throat pain, trouble opening the mouth, change to the voice[1] |
| Complications | Blockage of the airway, aspiration pneumonitis[1] |
| Causes | Multiple types of bacteria[1] |
| Risk factors | Streptococcal pharyngitis[1] |
| Diagnostic method | Based on the symptoms[1] |
| Differential diagnosis | Retropharyngeal abscess, infectious mononucleosis, epiglottitis, cancer[1] |
| Treatment | Antibiotics, remove pus, fluids, pain medication, steroids[1] |
| Frequency | ~3 per 10,000 per year (USA)[1] |
Peritonsillar abscess (PTA), also known as quinsy, is an accumulation of pus due to an infection behind the tonsil.[2] Symptoms include fever, throat pain, trouble opening the mouth, and a change to the voice.[1] Pain is usually worse on one side.[1] Complications may include blockage of the airway or aspiration pneumonitis.[1]
They are typically due to infection by a number of types of bacteria.[1] Often it follows streptococcal pharyngitis.[1] They do not typically occur in those who have had a tonsillectomy.[1] Diagnosis is usually based on the symptoms.[1] Medical imaging may be done to rule out complications.[1]
Treatment is by antibiotics, removing the pus, sufficient fluids, and pain medication.[1] Steroids may also be useful.[1] It may be reasonable to attempt treatment with medications alone initially.[3] Admission to hospital is generally not needed.[1] In the United States about 3 per 10,000 people per year are affected.[1] Young adults are most commonly affected.[1]
Signs and symptoms
Unlike tonsillitis, which is more common in the children, PTA has a more even age spread, from children to adults. Symptoms start appearing two to eight days before the formation of an abscess. A progressively severe sore throat on one side and pain during swallowing (odynophagia) usually are the earliest symptoms. As the abscess develops, persistent pain in the peritonsillar area, fever, a general sense of feeling unwell, headache and a distortion of vowels informally known as "hot potato voice" may appear. Neck pain associated with tender, swollen lymph nodes, referred ear pain and foul breath are also common. While these signs may be present in tonsillitis itself, a PTA should be specifically considered if there is limited ability to open the mouth (trismus).
Physical signs of a peritonsillar abscess include redness and swelling in the tonsillar area of the affected side and swelling of the jugulodigastric lymph nodes. The uvula may be displaced towards the unaffected side.
Complications
- Retropharyngeal abscess
- Extension of abscess in other deep neck spaces leading to airway compromise; see Ludwig's angina
- Sepsis
- Glomerulonephritis and rheumatic fever (strep throat chronic complications)
- Decreased oral intake and dehydration
Causes
PTA usually arises as a complication of an untreated or partially treated episode of acute tonsillitis. The infection, in these cases, spreads to the peritonsillar area (peritonsillitis). This region comprises loose connective tissue and is hence susceptible to formation of an abscess. PTA can also occur de novo. Both aerobic and anaerobic bacteria can be causative. Commonly involved aerobic pathogens include Streptococcus, Staphylococcus and Haemophilus. The most common anaerobic species include Fusobacterium necrophorum, Peptostreptococcus, Prevotella species, and Bacteroides.[4][5][6][7][8][9]
Diagnosis
Diagnosis is usually based on the symptoms.[1] Medical imaging may be done to rule out complications.[1] Medical imaging may include CT scan, MRI, or ultrasound is also useful in diagnosis.[1]
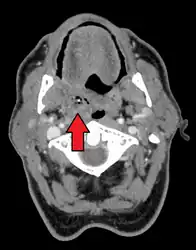 Peritonsillar abscess on the person's right as seen on CT imaging
Peritonsillar abscess on the person's right as seen on CT imaging.jpg.webp) Peritonsillar abscess
Peritonsillar abscess
Treatment
Treatment is by removing the pus, antibiotics, sufficient fluids, and pain medication.[1] Steroids, such as 10 mg dexamathasone, may also be useful.[1] Admission to hospital is generally not needed.[1]
Antibiotics
The infection is frequently penicillin resistant.[1] There are a number of antibiotics options including amoxicillin/clavulanate 875 mg by mouth twice per day or intravenous metronidazole 500 mg every 6 hours in combination with ceftriaxone 1 gram twice per day.[1] Piperacillin/tazobactam may also be used.[1]
Surgery
The pus can be removed by a number of methods including needle aspiration, incision and drainage, and tonsillectomy.[1] Incision and drainage may be associated with a lower chance of recurrence than needle aspiration but the evidence is very uncertain. Needle aspiration may be less painful but again the evidence is very uncertain.[10]
Treatment can also be given while a patient is under anesthesia, but this is usually reserved for children or anxious patients. Tonsillectomy can be indicated if a patient has recurring peritonsillar abscesses or a history of tonsillitis. For patients with their first peritonsillar abscess most ENT-surgeons prefer to "wait and observe" before recommending tonsillectomy.[11]
Epidemiology
It is a commonly encountered otorhinolaryngological (ENT) emergency.[11]
The number of new cases per year of peritonsillar abscess in the United States has been estimated approximately at 30 cases per 100,000 people.[12] In a study in Northern Ireland, the number of new cases was 10 cases per 100,000 people per year.[13] In Denmark, the number of new cases is higher and reaches 41 cases per 100,000 people per year.[14] Younger children who develop a peritonsillar abscess are often immunocompromised and in them, the infection can cause airway obstruction.[15]
Society and culture
Word orgin
The condition is often referred to as "quincy", "quinsy",[16] or "quinsey", anglicised versions of the French word esquinancie which was originally rendered as squinsey and subsequently quinsy.[17]
Notable cases
- Sultan Tekish of Kwarezm[18]
- Osceola[19]
- Michel de Montaigne[20]
- Pope Adrian IV
- George Washington was believed to have died of complications arising from quinsy, but is now thought to have died from epiglottitis.[21]
- James Gregory of the band The Ordinary Boys almost died from quinsy because it was left untreated for so long before emergency treatment was started.[22]
- Eiichiro Oda, author of the best-selling One Piece manga, was hospitalized due to complications.[23]
- Ian Maclaren died of complications from quinsy while on a lecture tour of the United States.[24]
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 Galioto NJ (April 2017). "Peritonsillar Abscess". American Family Physician. 95 (8): 501–506. PMID 28409615.
- ↑ "Tonsillar Cellulitis and Tonsillar Abscess - Ear, Nose, and Throat Disorders - Merck Manuals Consumer Version". Merck Manuals Consumer Version. Archived from the original on 25 October 2017. Retrieved 24 October 2017.
- ↑ Forner, D; Curry, DE; Hancock, K; MacKay, C; Taylor, SM; Corsten, M; Trites, JR; Rigby, MH (November 2020). "Medical Intervention Alone vs Surgical Drainage for Treatment of Peritonsillar Abscess: A Systematic Review and Meta-analysis". Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 163 (5): 915–922. doi:10.1177/0194599820927328. PMID 32482146.
- ↑ Brook I, Frazier EH, Thompson DH (March 1991). "Aerobic and anaerobic microbiology of peritonsillar abscess". The Laryngoscope. 101 (3): 289–92. doi:10.1288/00005537-199103000-00012. PMID 2000017.
- ↑ Sakae FA, Imamura R, Sennes LU, Araújo Filho BC, Tsuji DH (2006). "Microbiology of peritonsillar abscesses". Brazilian Journal of Otorhinolaryngology. 72 (2): 247–51. doi:10.1016/S1808-8694(15)30063-X. PMID 16951860. Archived from the original on 2014-07-14.
- ↑ Gavriel H, Lazarovitch T, Pomortsev A, Eviatar E (January 2009). "Variations in the microbiology of peritonsillar abscess". European Journal of Clinical Microbiology & Infectious Diseases. 28 (1): 27–31. doi:10.1007/s10096-008-0583-6. PMID 18612664.
- ↑ Sunnergren O, Swanberg J, Mölstad S (2008). "Incidence, microbiology and clinical history of peritonsillar abscesses". Scandinavian Journal of Infectious Diseases. 40 (9): 752–5. doi:10.1080/00365540802040562. PMID 19086341.
- ↑ Klug TE, Henriksen JJ, Fuursted K, Ovesen T (May 2011). "Significant pathogens in peritonsillar abscesses". European Journal of Clinical Microbiology & Infectious Diseases. 30 (5): 619–27. doi:10.1007/s10096-010-1130-9. PMID 21181222. Archived from the original on 2020-01-25. Retrieved 2019-01-22.
- ↑ Powell EL, Powell J, Samuel JR, Wilson JA (September 2013). "A review of the pathogenesis of adult peritonsillar abscess: time for a re-evaluation". The Journal of Antimicrobial Chemotherapy. 68 (9): 1941–50. CiteSeerX 10.1.1.1001.2391. doi:10.1093/jac/dkt128. PMID 23612569.
- ↑ Chang BA, Thamboo A, Burton MJ, Diamond C, Nunez DA, et al. (Cochrane ENT Group) (December 2016). "Needle aspiration versus incision and drainage for the treatment of peritonsillar abscess". The Cochrane Database of Systematic Reviews. 12: CD006287. doi:10.1002/14651858.CD006287.pub4. PMC 6463807. PMID 28009937.
- 1 2 Raut VV (2000). "Management of peritonsillitis/peritonsillar". Revue de Laryngologie - Otologie - Rhinologie. 121 (2): 107–10. PMID 10997070.
- ↑ Johnson RF, Stewart MG (June 2005). "The contemporary approach to diagnosis and management of peritonsillar abscess". Current Opinion in Otolaryngology & Head and Neck Surgery. 13 (3): 157–60. doi:10.1097/01.moo.0000162259.42115.38. PMID 15908813.
- ↑ Hanna BC, McMullan R, Gallagher G, Hedderwick S (April 2006). "The epidemiology of peritonsillar abscess disease in Northern Ireland". The Journal of Infection. 52 (4): 247–53. doi:10.1016/j.jinf.2005.07.002. PMID 16125782.
- ↑ Ehlers Klug T, Rusan M, Fuursted K, Ovesen T (November 2009). "Fusobacterium necrophorum: most prevalent pathogen in peritonsillar abscess in Denmark". Clinical Infectious Diseases. 49 (10): 1467–72. doi:10.1086/644616. PMID 19842975.
- ↑ Hardingham M (May 1987). "Peritonsillar infections". Otolaryngologic Clinics of North America. 20 (2): 273–8. PMID 3474580.
- ↑ "Peritonsillitis (Peritonsillar Cellulitis and Peritonsillar Abscess)". Marx: Rosen's Emergency Medicine (7th ed.). Mosby, An Imprint of Elsevier. 2009. Archived from the original on 4 October 2015. Retrieved 8 July 2013.
- ↑ Greene, Richard Gleason (1890). The International cyclopedia: a compendium of human knowledge, Volume 12. Mead Dodd. pp. 355–6. Archived from the original on 2016-09-25.
- ↑ Juvaini, Ala-ad-Din Ata-Malik (1997). History of the World Conqueror. Manchester U.K.: Manchester University Press. p. 314.
- ↑ Wickman, Patricia Riles (2006). Osceola's Legacy. University of Alabama Press. p. 144.
- ↑ de Montaigne, Michel (1877). "Essays of Michel de Montaigne". In William Carew Hazlitt (ed.). The Life of Montaigne. Vol. 1. Translated by Charles Cotton (Kindle ed.).
- ↑ Mount Vernon Plantation (2006). "Part 4. President and Back Home". Meet George Washington. Mount Vernon Ladies Association. Archived from the original on 19 January 2005.
- ↑ "Ordinary Boys reveal illness that caused V cancellation". 21 August 2006. Archived from the original on 22 July 2010. Retrieved 7 August 2010.
- ↑ "NEWS: One Piece on Break". Viz Media. Archived from the original on 2013-06-07. Retrieved 2013-05-21.
- ↑ Nicoll, W. Robertson (1908). 'Ian Maclaren': Life of the Rev. John Watson, D.D. London: Hodder and Stoughton. p. 379.
External links
| Classification | |
|---|---|
| External resources |