Depressant
Depressants, or central depressants, are drugs that lower neurotransmission levels, or depress or reduce arousal or stimulation in various areas of the brain.[1] Depressants are also colloquially referred to as "downers" as they lower the level of arousal when taken. Depressants do not change the mood or mental state of others. Stimulants, or "uppers," increase mental or physical function, hence the opposite drug class from depressants are stimulants, not antidepressants.
Depressants are widely used throughout the world as prescription medicines and illicit substances. Alcohol is a very prominent depressant. When depressants are used, effects often include ataxia, anxiolysis, pain relief, sedation or somnolence, cognitive or memory impairment, as well as, in some instances, euphoria, dissociation, muscle relaxation, lowered blood pressure or heart rate, respiratory depression, and anticonvulsant effects. Depressants also act to produce anesthesia. Cannabis may sometimes be considered a depressant due to one of its components, cannabidiol. The latter is known to treat insomnia, anxiety, and muscle spasms, similar to other depressive drugs. However, while tetrahydrocannabinol, another component, may slow brain function to a small degree while reducing reaction to stimuli, it is generally considered a stimulant and main psychoactive agent that can sometimes cause anxiety, panic, and psychosis instead. Other depressants can include drugs like Xanax (a benzodiazepine) and a number of opioids. Gabapentinoids like gabapentin and baclofen are depressants and have anticonvulsant, and anxiolytic effects. Most anticonvulsants like Lamotrigine and Phenytoin are depressants. Carbamates are depressants that are similar to barbiturates.
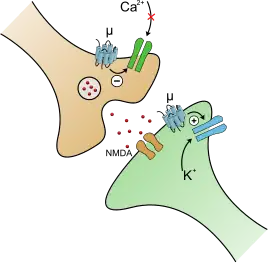
Depressants exert their effects through a number of different pharmacological mechanisms, the most prominent of which include facilitation of GABA and inhibition of glutamatergic or monoaminergic activity. Other examples are chemicals that modify the electrical signaling inside the body, the most prominent of which are bromides and channel blockers.
Indications
Depressants are used medicinally to relieve the following symptoms:
Types

Alcohol
An alcoholic beverage is a drink that contains alcohol (known formally as ethanol), an anesthetic that has been used as a psychoactive drug for several millennia. Ethanol is the oldest recreational drug still used by humans. Ethanol can cause alcohol intoxication when consumed. Alcoholic beverages are divided into three general classes for taxation and regulation of production: beers, wines, and spirits (distilled beverages). They are legally consumed in most countries around the world. More than 100 countries have laws regulating their production, sale, and consumption.[2]
The most common way to measure intoxication for legal or medical purposes is through blood alcohol content (also called blood alcohol concentration or blood alcohol level). It is usually expressed as a percentage of alcohol in the blood in units of mass of alcohol per volume of blood, or mass of alcohol per mass of blood, depending on the country. For instance, in North America a blood alcohol content of 0.10 g/dL means that there are 0.10 g of alcohol for every dL of blood (i.e., mass per volume is used there).[3]
Barbiturates
Barbiturates are effective in relieving the conditions that they are designed to address (insomnia, seizures). They are also commonly used for unapproved purposes, are physically addictive, and have serious potential for overdose. By the late 1950s, concerns over the mounting social costs associated with barbiturates, which were beginning to overshadow their perceived medical benefits, prompted a concerted effort to find alternative medications. Most people still using barbiturates today do so in the prevention of seizures or in mild form for relief from the symptoms of migraines.

Benzodiazepines
A benzodiazepine (sometimes colloquially "benzo"; often abbreviated "BZD") is a drug whose core chemical structure is the fusion of a benzene ring and a diazepine ring. The first such drug, chlordiazepoxide (Librium), was discovered accidentally by Leo Sternbach in 1955 and made available in 1960 by Hoffmann–La Roche, who has also marketed the benzodiazepine diazepam (Valium) since 1963.
Benzodiazepines enhance the effect of the neurotransmitter gamma-aminobutyric acid (GABA) at the GABAA receptor, resulting in sedative, hypnotic (sleep-inducing), anxiolytic (anti-anxiety), anticonvulsant, and muscle relaxant properties; also seen in the applied pharmacology of high doses of many shorter-acting benzodiazepines are amnesic-dissociative actions. These properties make benzodiazepines useful in treating anxiety, insomnia, agitation, seizures, muscle spasms, alcohol withdrawal, and as a premedication for medical or dental procedures. Benzodiazepines are categorized as either short-, intermediate-, or long-acting. Short- and intermediate-acting benzodiazepines are preferred for the treatment of insomnia; longer-acting benzodiazepines are recommended for the treatment of anxiety.
In general, benzodiazepines are safe and effective in the short term, although cognitive impairments and paradoxical effects such as aggression or behavioral disinhibition occasionally occur. A minority react reverse and contrary to what would normally be expected. For example, a state of panic may worsen considerably following intake of a benzodiazepine. Long-term use is controversial due to adverse psychological and physical effects, decreasing effectiveness, physical dependence, and benzodiazepine withdrawal syndrome, following withdrawal after long-term use. Due to adverse effects associated with the long-term use of benzodiazepines, withdrawal from benzodiazepines generally leads to improved physical and mental health. The elderly are at an increased risk of experiencing both short- and long-term adverse effects.
There is controversy concerning the safety of benzodiazepines in pregnancy. While they are not major teratogens, uncertainty remains as to whether they cause cleft palate in a small number of babies and whether neurobehavioral effects occur as a result of prenatal exposure; they are known to cause withdrawal symptoms in the newborn. Benzodiazepines can be taken in overdoses and can cause dangerous deep unconsciousness. However, they are much less toxic than their predecessors, barbiturates, and death rarely results when a benzodiazepine is the only drug taken; however, when combined with other central nervous system depressants such as alcohol and opiates, the potential for toxicity and fatal overdose increases. Benzodiazepines are commonly misused and taken in combination with other addictive drugs. In addition, all benzodiazepines are listed in Beers List, which is significant in clinical practice.
Cannabis
Cannabis is often considered either in its own unique category or as a mild psychedelic.[4][5] The chemical compound tetrahydrocannabinol (THC), which is found in cannabis, has many depressant effects such as muscle relaxation, sedation, decreased alertness, and tiredness.[6] Contrary to the previous statement, activation of the CB1 receptor by cannabinoids causes an inhibition of GABA, the exact opposite of what central nervous system depressants do.

Carbamates
Carbamates are a class of depressants or "tranquilizers" that are synthesized from urea.[7] Carbamates have anxiolytic,[8] muscle relaxant,[8] anticonvulsant,[9] hypnotic,[8] antihypertensive,[10] and analgesic effects. They have other uses like muscle tremors, agitation, and alcohol withdrawal. Their muscle relaxant effects are useful for strains, sprains, and muscle injuries combined with rest, physical therapy, and other measures.[8] The effects, synthesis, and mechanism of action of Carbamates are very similar to barbiturates.[11] There are many different types of Carbamates: some only produce anxiolytic and hypnotic effects while some only have anticonvulsant effects.
Side effects of Carbamates include drowsiness, dizziness, headache, diarrhea, nausea, flatulence, liver failure, poor coordination, nystagmus, abuse, dizziness, weakness, nervousness, euphoria, overstimulation, and dependence. Uncommon but potentially severe adverse reactions include hyper sensitivity reactions such as Stevens Johnson syndrome, embryo-fetal toxicity, stupor, and coma. Carbamates are fatal in overdose, which is why many have been replaced with benzodiazepines. It is not recommended to use most Carbamates like Carisoprodol for a long time as physical and psychological dependence does occur.[12]
Meprobamate, which metabolizes to Carisoprodol, was launched in 1955. It quickly become the first blockbuster psychotropic drug in America, becoming popular in Hollywood and gaining fame for its seemingly miraculous effects. It has since been marketed under more than 100 trade names, including Amepromat, Quivet, and Zirpon. Carisoprodol, which is still used mainly for its muscle relaxant effects, can potentially abuse. Its mechanism of action is very similar to barbiturates, alcohol, methaqualone, and benzodiazepines. Carisoprodol allosterically modulates and directly activates the human α1β2γ2 GABAAR (GABAA) in the central nervous system, similar to barbiturates. This causes chloride channels to open, allowing chloride to flood into the neuron. This slows down communication between neurons and the nervous system.[13] Unlike benzodiazepines, which increase the frequency of the chloride channel opening, Carisoprodol increases the duration of channel opening when GABA is bound.[14][15] GABA is the main inhibitory neurotransmitter in the nervous system, which causes its depressant effects.
Carbamates are fatal in overdose. Symptoms are similar to a barbiturate overdose and typically include difficulty thinking, poor coordination, decreased level of consciousness, and a decreased effort to breathe (respiratory depression). An overdose is more likely to be fatal when mixed with another depressant that suppresses breathing.
Physical and psychological dependence does happen with long term use of Carbamates; particularly Carisoprodol. Today Carisoprodol is only used in the short-term for muscle pain, particularly back pain. Discontinuation after long-term use could be very intense and even possibly fatal. Withdrawal can resemble barbiturate, alcohol, or benzodiazepine withdrawal, as they all have a similar mechanism of action. Discontinuation symptoms include confusion, disorientation, delirium, hallucinations (auditory & visual), insomnia, decreased appetite, anxiety, psychomotor agitation, pressured speech, tremor, tachycardia, and seizures, which could be fatal.[16]
Carbamates gained widespread use in the 1950s, alongside barbiturates. While their popularity has gradually waned due to concerns over overdose and dependence potential, newer derivatives of carbamates continue to be developed. Among these is Felbamate, an anticonvulsant that was approved in 1993 and is commonly used today. It is a GABAA positive allosteric modulator and blocks the NR2B subunit of the NMDA receptor. Other carbamates block sodium channels. Phenprobamate was used as an anxiolytic and is still sometimes used in Europe for general anesthesia and for treating muscle cramps and spasticity. Methocarbamol is a popular drug that is commonly known as Robaxin and is over-the-counter in some countries. It is a carbamate with muscle relaxant effects. Tetrabamate is a controversial drug that is a combination of febarbamate, difebarbamate, and phenobarbital. It is marketed in Europe and has been largely but not completely discontinued. On April 4, 1997, after over 30 years of use due to reports of hepatitis and acute liver failure, the use of the drug was restricted. Carisoprodol, known as "Soma", is still commonly used today for its muscle relaxant effects. It is also very commonly abused around the world. It is a Schedule IV substance in the United States. Famous martial artist and actor Bruce Lee died due to an allergic reaction to meprobamate.
Approved
- Carisoprodol/Meprobamate/Tybamate (Soma/Miltown, Solacen) (muscle relaxant, anxiolytic, tranquilizer)
- Difebarbamate (Atrium, Sevrium) (tranquilizer)
- Emylcamate (Striatran) (anxiolytic and muscle relaxant)
- Ethinamate (Valamin, Valmid) (sedative-hypnotic)
- Febarbamate/Phenobamate (Solium, Tymium) (anxiolytic and tranquilizer)
- Felbamate (Felbatol) (anticonvulsant)
- Hexapropymate (Merinax) (hypnotic-sedative)
- Mebutamate (Capla, Dormate) (anxiolytic, sedative, antihypertensive)
- Phenprobamate (Gamaquil, Isotonil) (muscle relaxant, sedative, anxiolytic, anticonvulsant, anesthesia)
- Procymate (Equipax) (sedative, anxiolytic)
- Styramate (Sinaxamol) (muscle relaxant, anticonvulsant)
- Tetrabamate (febarbamate, difebarbamate, phenobarbital) (Atrium, G Tril, Sevrium) (anxiety, alcohol withdrawal, muscle tremors, agitation, depression)
Although a drug may be approved, that does not necessarily mean it is still being used today.
Not approved
- Carisbamate (anticonvulsant)
- Clocental (hypnotic)
- Cyclarbamate (muscle relaxant and tranquilizer)
- Lorbamate (muscle relaxant and tranquilizer)
- Nisobamate (tranquilizer)
- Pentabamate (tranquilizer)
Gabapentinoids
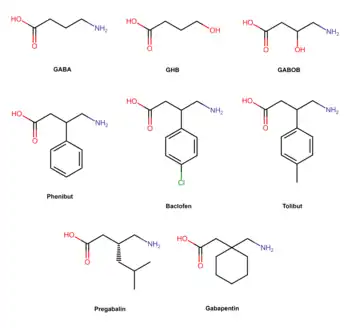
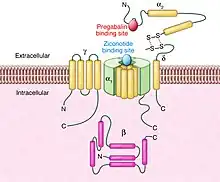

Gabapentinoids are a unique and relatively novel class of depressants that selectively bind to the auxiliary α2δ subunit (CACNA2D1 and CACNA2D2) site of certain VDCCs, and thereby act as inhibitors of α2δ subunit-containing Voltage-gated calcium channels. α2δ is nicknamed the "Gabapentin receptor". At physiologic or resting membrane potential, VDCCs are normally closed. They are activated (opened) at depolarized membrane potentials, which is the source of the "voltage-gated" epithet. Gabapentinoids bind to the α1 and α2 sites of the α2δ subunit family. Gabapentin is the prototypical gabapentinoid. The α2δ is found on L-type calcium channels, N-type calcium channels, P/Q-type calcium channels, and R-type calcium channels throughout the central and peripheral nervous systems. α2δ is located on presynaptic neurons and affects calcium channel trafficking and kinetics, initiates extracellular signaling cascades, gene expression, and promotes excitatory synaptogenesis through thrombospondin 1 .[17] Gabapentinoids are not direct channel blockers; rather, they disrupt the regulatory function of α2δ and its interactions with other proteins. Most of the effects of gabapentinoids are mediated by the high voltage activated N and P/Q-type calcium channels. P/Q-type calcium channels are mainly found in the cerebellum (Purkinje neurons) which may be responsible for the ataxic adverse effect of gabapentinoids, while N-type calcium channels are located throughout the central and peripheral nervous systems. N-type calcium channels are mainly responsible for the analgesic effects of gabapentinoids. Ziconotide, a non-gabapentinoid ω-conotoxin peptide, binds to the N-type calcium channels and has analgesic effects 1000 times stronger than morphine. Gabapentinoids are selective for the α2δ site, but non-selective when they bind to the calcium channels complex. They act on the α2δ site to lower the release of many excitatory and pro-nociceptive neurochemicals including glutamate, substance P, calcitonin gene-related peptide (CGRP), and more.[18][19][20]
Gabapentinoids are absorbed from the intestines mainly by the Large neutral amino acid transporter 1 (LAT1, SLC7A5) and the Excitatory amino acid transporter 3 (EAAT3). They are one of the few drugs that use these amino acid transporters. Gabapentinoids are structurally similar to the Branched-chained amino acids L-leucine and L-isoleucine, both of which also bind to the α2δ site. Branched-chained amino acids like l-leucine, l-isoleucine, and l-valine have many functions in the central nervous system. They modify large neutral amino acid (LNAA) transport at the blood–brain barrier and reduce the synthesis neurotransmitter of neurotransmitters derived from aromatic-amino acids, notably serotonin from tryptophan and catecholamines from tyrosine and phenylalanine.[21] This may be relevant to the pharmacology of gabapentinoids.
Gabapentin was designed by researchers at Parke-Davis to be an analogue of the neurotransmitter GABA that could more easily cross the blood–brain barrier and was first described in 1975 by Satzinger and Hartenstein.[22][23] Gabapentin was first approved for epilepsy, mainly as an add-on treatment to partial seizures. Gabapentinoids are GABA analogues,[24] but they do not bind to the GABA receptors, convert into GABA or another GABA receptor agonist in vivo, or directly modulate GABA transport or metabolism.[25][26] Phenibut and baclofen, two structurally related compounds, are exceptions, as they mainly act on the GABA B receptor.[27][28] Gabapentin, but not pregabalin, has been found to activate voltage-gated potassium channel (KCNQ), which might potentiate its depressant qualities. Despite this, gabapentinoids mimic GABA activity by inhibiting neurotransmission.[29] Gabapentinoids prevent delivery of the calcium channels to the cell membrane and disrupt interactions of α2δ with NMDA receptors, AMPA receptors, neurexins, and thrombospondins. Some calcium channel blockers of the dihydropyridine class are used for hypertension weakly block α2δ.[30]
Gabapentinoids have anxiolytic, anticonvulsant, antiallodynic, antinociceptive and possibly muscle relaxant properties.[19][31][32] Pregabalin and gabapentin are used in epilepsy, mainly partial seizures (focal). Gabapentinoids are not effective for generalized seizures. They are also used for postherpetic neuralgia, neuropathic pain associated with diabetic neuropathy, fibromyalgia, generalized anxiety disorder, and restless legs syndrome.[33][34][35][36][37][38] Pregabalin and gabapentin have many off-label uses including insomnia,[39] alcohol and opioid withdrawal,[40] smoking cessation,[41] social anxiety disorder,[42] bipolar disorder,[43][44] attention deficit hyperactivity disorder,[45] chronic pain, hot flashes,[46] tinnutus, migraines, and more. Baclofen is primarily used for the treatment of spastic movement disorders, especially in instances of spinal cord injury, cerebral palsy, and multiple sclerosis.[47] Phenibut is used in Russia, Ukraine, Belarus and Latvia to treat anxiety and to improve sleep, as in the treatment of insomnia.[48] It is also used for various other indications, including the treatment of asthenia, depression, alcoholism, alcohol withdrawal syndrome, post-traumatic stress disorder, stuttering, tics, vestibular disorders, Ménière's disease, dizziness, for the prevention of motion sickness, and for the prevention of anxiety before or after surgical procedures or painful diagnostic tests.[48] Phenibut, like other GABA B agonists, is also sometimes used by body builders to increase the human growth hormone.
Reuters reported on 25 March 2010 that "Pfizer Inc violated a United States racketeering law by improperly promoting the epilepsy drug Neurontin (gabapentin). Under the Racketeer Influenced and Corrupt Organizations Act, the penalty is automatically tripled, so the finding will cost Pfizer $141 million." The case stems from a claim from Kaiser Foundation Health Plan Inc. that "it was misled into believing Neurontin was effective for off-label treatment of migraines, bipolar disorder and other conditions. Pfizer argued that Kaiser physicians "still recommend the drug for those uses", and that "the insurer's website also still lists Neurontin as a drug for neuropathic pain."
In some cases, gabapentinoids are abused and provide similar effects to alcohol, benzodiazepines and gamma-hydroxybutyric acid (GHB).[49][50][51] The FDA placed a black box warning on Neurontin (gabapentin), and Lyrica (pregabalin), for serious breathing problems.[52] Mixing gabapentinoids with opioids, benzodiazepines, barbiturates, GHB, alcohol, or any other depressant is potentially deadly.[53][54][55][56]
Common side effects of gabapentinoids include drowsiness, dizziness, weakness, increased appetite, urinary retention, shortness of breath, involuntary eye movements (nystagmus), memory issues, uncontrollable jerking motions, auditory hallucinations, erectile dysfunction, and myoclonic seizures.[57][58]
An overdose of gabapentinoids usually consists of severe drowsiness, severe ataxia, blurred vision, slurred speech, severe uncontrollable jerking motions, and anxiety.[59][60] Like most anticonvulsants, pregabalin and gabapentin have an increased risk of suicidal thoughts and behaviors.[61][62] Gabapentinoids, like all calcium channel blockers, are known to cause angioedema.[63] Taking them with an ACE inhibitor can increase the toxic effects of gabapentinoids.[64] They may also enhance the fluid-retaining effect of certain anti-diabetic agents (thiazolidinediones). It is not known if they cause gingival enlargement like other calcium channel blockers. Gabapentinoids are excreted by the kidney mostly in their original form. Gabapentinoids can build up in the body when someone has renal failure. This usually presents itself as myoclonus and an altered mental state. It is unclear if it is safe to use gabapentinoids during pregnancy, with some studies showing potential harm.[65]
Physical or physiological dependence does occur during long-term use of gabapentinoids.[66] Following abrupt or rapid discontinuation of pregabalin and gabapentin people report withdrawal symptoms like insomnia, headache, nausea, diarrhea, flu-like symptoms, anxiety, depression, pain, hyperhidrosis, seizures, psychomotor agitation, confusion, disorientation, and gastrointestinal complaints.[67][68] Acute withdrawal from baclofen and phenibut may also cause auditory and visual hallucinations, as well as acute psychosis.[69][70] Baclofen withdrawal can be more intense if it is administered intrathecally or for long periods of time. If baclofen or phenibut is used for long periods of time it can resemble intense benzodiazepine, GHB or alcohol withdrawal. To minimize withdrawal symptoms, baclofen or phenibut should be tapered down slowly. Abrupt withdrawal from phenibut or baclofen could possibly be life-threatening because of its mechanism of action. Abrupt withdrawal can cause rebound seizures and severe agitation.[71][70]
- Gabapentin (Neurontin)
- Gabapentin Enacarbil (Horizant, Regnite)
- Gabapentin Extended-Release (Gralise)
- Pregabalin (Lyrica)
- Phenibut (Anvifen, Fenibut, Noofen)
- Baclofen (Lioresal)
- Mirogabalin (Tarlige) (Japan Only)
Not approved:
- Imagabalin
- Tolibut
- 4-Flurophenibut
- HSK16149
- Trans-4 and cis-4-[18F] fluorogabapentin (α2δ PET Imaging)
- 4-Methylpregabalin
- PD-217,014
- Atagabalin
- Arbaclofen
- Saclofen
Endogenous (not Gabapentinoids), endogenous BCAA amino acids that bind to α2δ):
- Phenylalanine
- NP-118809
- Gababutin
- Ziconotide (Approved for pain)
- Ethanol
- Dextrothyroxine (Agonist of α2δ instead of inhibiting it)[74]
- Ethioninie
- Suloctidil
- Terodiline
- Bepridil
Gamma-Hydroxybutyric acid

Gamma-Hydroxybutyric acid or "GHB" is a GABA analogue that is a natural occurring neurotransmitter and depressant drug.[75][76][77] It is also naturally found in small amounts some alcoholic beverages alongside ethanol.[78] GHB is the prototypical substance among a couple of GHB receptor modulators.[79]
GHB has been used as a general anesthetic[80][81] and as a treatment for cataplexy,[82][83] narcolepsy,[82][84] and alcoholism.[85][86][87][88] The sodium salt of GHB, sodium oxybate, is commonly used today for narcolepsy,[89] sudden muscle weakness,[90] and excessive daytime sleepiness. It is sold under the brand name Xyrem.[91][92][89]
As a depressant, GHB would worsen narcolepsy and muscle weakness. But in low doses GHB mainly affects the GHB receptor,[93][94] an excitatory receptor that releases dopamine and glutamate[95] giving GHB stimulant effects, the opposite of a depressant. But in large doses GHB activates the GABAB receptor, an inhibitory receptor in the central nervous system, which overpowers the excitatory effects, thus causing central nervous system depression.[96][97] Some antipsychotics are agonists of the GHB receptor.[98][99][100]
GHB can usually be found in either as sodium, potassium, magnesium, or calcium salts.[101][102] Xywav is a medication that is a mixture of all GHB salts[103] and is used to treat the same conditions as Xyrem. Both Xywav and Xyrem are Schedule III[104][105] and have a black box warning[106] for central nervous system depressant effects (hypoventilation & bradycardia) and for their very high potential for abuse.[107][79] Overdose on GHB is fatal with or without mixing other CNS depressants.[108][109][110][111] Death from GHB overdose is usually caused by respiratory depression, seizures, or coma.[96][112][113]
GHB is used illegally as an intoxicant, an aphrodisiac,[75][114] and as an athletic-performance enhancer.[79] It is a popular club drug in some parts of the world due to its powerful aphrodisiac and euphoric effects. Similarly to phenibut and baclofen, it is used by body-builders to increase the human growth hormone due to GABAB activation.[115][116] It has also been reportedly used as a date-rape drug.[117][118] This caused it to be a Schedule I substance in the United States and Canada and other countries. Xyrem, which is GHB in its sodium form, is Schedule III in the United States, Canada and other countries.[91][104]
In low doses, GHB mainly binds to the GHB receptor and weakly binds to the GABAB receptor.[94][93][119] The GHB receptor is an excitatory G protein-coupled receptor (GPCR).[94][93] Its endogenous ligand is GHB, since GHB is also a neurotransmitter.[76] It is also a transporter for vitamin B2. The existence of a specific GHB receptor was predicted by observing the action of GHB and related compounds that primarily act on the GABAB receptor, but also exhibit a range of effects which were found not to be produced by GABAB activity, and so were suspected of being produced by a novel and at the time unidentified receptor target. At higher doses seizures are very common.[112] This is thought to be mediated through increased Na+/K+ current and increased release of dopamine and glutamate.[95] GHB can also causes absence seizures;[112][120][121] the mechanism is currently not known but it is believed to be due to interactions with the GABAB receptor.[120] It is being investigated if endogenous GHB is responsible for non-convulsive seizures in humans.[112][122]
GHB withdrawal is very intense.[123] Physical dependence develops quickly. It is also highly psychologically addictive. It shares some similarities with the withdrawal of gabapentinoids phenibut and baclofen due to the activation of the GABAB receptor. It features a typical depressant withdrawal syndrome that mimics alcohol withdrawal.[124] Symptoms include delirium, tremor, anxiety, tachycardia, insomnia, hypertension, confusion, sweating, severe agitation which may require restraint,[125] auditory and visual hallucinations and possibly death from tonic-clonic seizures.[126][124][127][128][129]
Baclofen and phenibut are very effective for withdrawal and are preferred by patients over benzodiazepines for treatment of withdrawal.[127]
GHB receptor modulators:
GHB receptor agonists:
- Gamma-Hydroxybutyric acid (GHB) (Xyrem)
- Calcium Oxybate, Magnesium Oxybate, Sodium Oxybate (Xyrem), Potassium Oxybate. Xywav is a mixture of all these salts.
- 3-hydroxycyclopent-1-enecarboxylic acid (HOCPCA)
- γ-hydroxycrotonic acid, trans-4-Hydroxycrotonic acid (GHC, T-HCA)
- Amisulpride, Levosulpiride, Sulpiride, Sultopride Antipsychotic GHB receptor ligands
- 3-Chloropropanoic acid (UMB66)
- 3-phenylpropyloxybutyric acid (UMB72)
- 4-benzyloxybutyric acid (UMB73)
- 4-hydroxy-4-napthylbutanoic acid (UMB86)
- 5-Hydroxypentanoate (UMB58)
- gamma-(4-methoxybenzyl)-gamma-hydroxybutyric acid (NCS-435)
- 4-(4-chlorophenyl)-4-hydroxy-2-butanoic acid (NCS-356)
- 3-hydroxyphenylacetic acid (3-HPA)
- Catechin, Monastrol Positive allosteric modulators
Prodrugs that metabolize into GHB:
- γ-Hydroxyvaleric acid (GHV)
- gamma-Valerolactone, γ-Valerolactone (GVL) prodrug to GHV
- 1,4-Butanediol (1,4-BD)
- 1,4-Butanediol acetate (DABD)
- Ethyl acetoxy butanoate (EAB)
- Aceburic acid (GHB acetate)
- gamma-Butyrolactone, γ-Butyrolactone (GBL)
- 2-Furanone, γ-crotonolactone (GCL)
- Gamma-Hydroxybutyraldehyde, γ-Hydroxybutyraldehyde (GHBAL)
- Gamma-Hydroxyvaleric acid, γ-Hydroxyvaleric acid (GHV)
GHB receptor antagonists:
Some GHB receptors modulators only bind to the GHB receptor, while others bind to both the GHB and GABAB receptors
Nonbenzodiazepines

Nonbenzodiazepines, sometimes referred to as Z-drugs, are a class of hypnotic depressants that are mainly used to treat insomnia and sometimes anxiety.[130] They are structurally related do benzodiazepines. They positively modulate the benzodiazepine site of the GABAA receptor, the chief inhibitory receptor of the central nervous system just like benzodiazepines, but a molecular level, they are structurally unrelated.
Nonbenzodiazepines bind to the benzodiazepine of the GABAA receptor site to keep the chloride channel open.[131] This causes chloride in the intercellular area to flood into the neuron.[132] Since chloride has a negative charge it causes the neuron to rest and cease firing. This results in a relaxing and depressant effect in the central nervous system.
Common nonbenzodiazepines like Zolpidem and Zopiclone are extremely effective for insomnia but carry many risks and side effects. Sleeping pills, including zopiclone, have been associated with an increased risk of death.
Adverse reactions as follows: "taste disturbance (some report a metallic like taste); less commonly nausea, vomiting, dizziness, drowsiness, dry mouth, headache; rarely amnesia, confusion, depression, hallucinations, nightmares; very rarely light headedness, incoordination, paradoxical effects, and sleep-walking also reported". Some users of nonbenzodiazepines have sleep-walked and committed murders or have been involved in motor vehicle accidents. Unlike benzodiazepines, nonbenzodiazepines have a risk of hallucinations and sleep-walking. Like benzodiazepines, they can cause anterograde amnesia.
Nonbenzodiazepines should not be discontinued abruptly if taken for more than a few weeks due to the risk of rebound withdrawal effects and acute withdrawal reactions, which may resemble those seen during benzodiazepine withdrawal. Treatment usually entails gradually reducing the dosage over a period of weeks or several months depending on the individual, dosage, and length of time the drug has been taken. If this approach fails, a crossover to a benzodiazepine equivalent dose of a long-acting benzodiazepine (such as chlordiazepoxide or more preferably diazepam) can be tried followed by a gradual reduction in dosage. In extreme cases and, in particular, where severe addiction and/or abuse is manifested, an inpatient detoxification may be required, with flumazenil as a possible detoxification tool.
Opioids/Opiates


Opioids are substances that act on opioid receptors to reduce pain.[133] Medically they are primarily used for pain relief, including anesthesia. Opioids also cause euphoria and are highly abused.
Opioids and Opiates are not the same. Opiates refer to natural opioids such as morphine and codeine. Opioids refer to all natural, semisynthetic, and synthetic opioids, like heroin and oxycodone.
Contrary to popular misconception, opioids are not depressants in the classical sense.[4] They do produce central nervous system depression, but they also excite certain areas of the central nervous system. To remain true to the term 'depressant' – opioids cannot be classified as such. For opioid agonists and opium derivatives, these are classified differently. analgesic or narcotic correctly identifies these drugs. However, they do have depressant actions nonetheless.
There are three principal classes of opioid receptors, μ, κ, δ (mu, kappa, and delta),[134] although up to seventeen have been reported, and include the ε, ι, λ, and ζ (Epsilon, Iota, Lambda and Zeta) receptors. Conversely, σ (Sigma) receptors are no longer considered to be opioid receptors because their activation is not reversed by the opioid inverse-agonist naloxone.The nociception opioid peptide receptor (NOP) (ORL1) is an opioid receptor which is involved in pain responses, anxiety, movement, reward, hunger, memory, and much more. It plays a major role in the development of tolerance to μ-opioid agonists.[135]
When "pain" occurs, a signal gets sent from the site of possible injury. This signal goes up the spinal cord into the brain where it is perceived as a negative emotion known as nociception or "hurt". In the central nervous system, the spine is connected to the brain by a structure called the brain stem.[136] The brain stem is the first part of the brain that develops in a mammal out of the neural crest. It is also the oldest part of the brain and controls many automatic functions such as consciousness, breathing, heart rate, digestion, and many more. Opioid receptors are specialized pain blocking receptors. They bind a wide range of hormones, peptides, and much more. Although they are found everywhere in the central nervous system, they are highly concentrated in the brain stem. Depending on the receptor, activation of them has the ability to stop pain from making its way to the brain and being perceived as pain. Hence opioids do not actually "stop" pain; they simply stop you from knowing you are in pain. Pain and the ability to modify it based on an organism's environment is an evolutionary advantage, and it has been shown that it can help an organism escape and survive certain situations where they may otherwise be immobilized due to pain and injury. The midbrain nuclei of the brain stem, with structures like the periaqueductal gray, reticular formation, and rostromedial tegmental nucleus, are responsible for the majority of the physical and psychological effects of endogenous and exogenous opioids.
The μ-opioid receptor is the responsible for the analgesic, euphoric, and adverse effects of opioids. The μ-opioid receptor is a G-protein coupled receptor. When the μ-opioid receptor is activated, it causes pain relief, euphoria, constipation, constricted pupils, itching, and nausea. The μ-opioid is located in the gastrointestinal tract, which controls peristalsis. This causes constipation, which can be extremely problematic and distressing. Activation of this receptor also causes relaxation of voluntary and involuntary muscles which can cause side effects like trouble urinating and swallowing. The μ-opioid receptor can also reduce androgens, thus decreasing libido and sexual function. The receptor is also known to cause "musical anhedonia".[137]
The receptor plays a critical role in feeding. The palatability of food is determined by opioid receptor-related processes in the nucleus accumbens and ventral pallidum. The opioid processes involve mu opioid receptors and are present in the rostromedial shell of the nucleus accumbens on its spiny neurons. This area has been called the "opioid eating site".
The μ-opioid receptor has many endogenous ligands including endorphin.[138]
Common and short term
Other
- Cognitive effects
- Opioid dependence
- Dizziness
- Loss of appetite
- Delayed gastric emptying
- Decreased sex drive
- Impaired sexual function
- Decreased testosterone levels
- Depression
- Immunodeficiency
- Increased pain sensitivity
- Irregular menstruation
- Increased risk of falls
- Slowed breathing
- Coma
The Kappa receptor (KOR) is a G protein-coupled receptor located in the central nervous system. KOR is also a G-protein coupled receptor.[140] Humans and some other primates have a higher density of kappa receptors than most other animals. KOR is responsible for nociception, consciousness, motor control, and mood. Dysregulation of this receptor system has been implicated in alcohol and drug addiction. The endogenous ligand for KOR is dynorphin. Activation of KOR usually causes dysphoria; hence the name dynorphin. The intoxicating plant, Salvia divinorum contains salvinorin A, an alkaloid that is a potent and selective κ-opioid (kappa-opioid) receptor agonist. This causes powerful hallucinations. Antagonizing the κ-opioid (kappa-opioid) receptor may be able to treat depression, anxiety, stress, addiction and alcoholism.[141]
The third receptor is the δ-opioid receptor (DOR). The delta receptor is the least studied out of the 3 main opioid receptors. It is a G-protein coupled receptor, and its endogenous ligand is deltorphin. Activation of δ-opioid receptor (DOR) may have antidepressant effects. δ-opioid agonists can produce respiratory depression at very high doses; at lower doses, they have the opposite effect. High doses of an δ-opioid agonist can cause seizures, although not all delta agonists produce this effect.[142] Activation of the delta receptor is usually stimulating instead of sedating like most opioids.
The nociception receptor is involved in the regulation of numerous brain activities, particularly instinctive emotional behaviors and pain.[143] (NOP) is a G-protein coupled receptor. The nociception receptor controls a wide range of biological functions including nociception, food intake, memory processes, cardiovascular and renal functions, spontaneous locomotor activity, gastrointestinal motility, anxiety, and the control of neurotransmitter release at peripheral and central sites.[144]
An opioid overdose is fatal. A person overdosing on opioids/opiates is presented with respiratory depression, a lethal condition that can cause hypoxia from slow and shallow breathing. Mixing opioids with another depressant such as benzodiazepines or alcohol increases the chance of an overdose and respiratory depression. Opioid overdose causes a decreased level of consciousness, pinpoint pupils and respiratory depression. Other symptoms include seizures and muscle spasms. Opioids activate μ-opioid receptors in specific regions of the central nervous system associated with respiratory regulation. They activate μ-opioid receptors in the medulla and pons. They are located in the brain stem connecting to the spine. This area has a high density of μ-opioid receptors as they block pain going up from spine into the brain. These areas are the oldest and most primitive parts of the brain. They control automatic functions such as breathing and digestion. Opioids stop this process and cause respiratory depression and constipation. The brain stem no longer detects carbon dioxide in the blood, so it does not initiate the inhalation reflex, usually resulting in hypoxia. Some overdose victims, however, die from cardiovascular failure, or asphyxiation from choking on their vomit.
Naloxone is a μ-opioid receptor antagonist,[145] meaning instead of activating the μ-opioid receptor it disrupts the functioning of the receptor.[145] Since Naloxone is powerful and highly selective for the μ-opioid receptor it can knock off powerful opioids like fentanyl off the receptor and block another ligand from binding to the receptor, thus stopping an overdose.[146] A person dependent on opioids may go into precipitated withdrawal when Naloxone is used.[147] Since naloxone blocks any endogenous or exogenous opioids from binding to the μ-opioid receptor.[147] This may cause a person to immediately go into withdrawal after naloxone is used.[148] This can cause withdrawal symptoms like cold sweats and diarrhea.
Opioids activate μ-opioid receptors in the rostromedial tegmental nucleus (RMTg). The Rostromedial tegmental nucleus is a GABAergic nucleus which functions as a "master brake" for the midbrain dopamine system.[149][150] The RMTg possesses robust functional and structural links to the dopamine pathways.[149][150] Opioids decrease the release of GABA, thus disinhibiting the GABAergic brake on dopamine networks.[149] GABA is an inhibitory neurotransmitter, meaning it either blocks or decreases the potential of a neuron firing.[151] This causes large amounts of dopamine to be released, as it is no longer blocked by GABA.[149] Disinhibition of GABA may be responsible for causing seizures, an uncommon adverse effect of opioids. The GABAergic disinhibition is also why Opioids are not considered true "depressants". This exciting of dopaminergic pathways causes the euphoria of opioids. This causes major positive reinforcing effects in the brain, instructing it to do it again. The RMTg is also responsible for development of tolerance and addiction. Psychostimulants also excite this pathway.[149][150]
Fentanyl is very commonly cut into other substances sold on the street. Fentanyl is used to increase the potency of substances, thus making the user spend more money on the laced substance.[152][153] Codeine is a weaker natural opiate that is usually used for bronchitis, diarrhea, and post-operative pain. It is very easy to overdose on these substances, especially if you have no tolerance. It is recommended to get your drugs tested, and to carry Naloxone.
Natural Opiates (Papaver somniferum, Opium)
- Morphine (MS Contin)
- Codeine (Tylenol No. 3)
- Papaverine (Pavabid)
- Noscapine (Narcotine)
- Thebaine
- Oripavine
- Narceine
Semi-synthetic Morphinan Opioids:
- Oxycodone (OxyContin)
- Heroin (Diamorphine)
- Hydrocodone (Vicodin)
- Oxymorphone (Opana)
- Hydromorphone (Dilaudid)
- Buprenorphine (Suboxone)
- Naloxone (Narcan)
Semi-synthetic Opioids are derived from the natural alkaloid thebaine.
Fully synthetic Opioids:
- Fentanyl (Duragesic)
- Tramadol (Ultram)
- Methadone (Dolophine)
- Pethidine (Demerol)
- Ketobemidone (Ketogan)
- Pentazocine (Talwin)
- Carfentanil (Wildnil)
- Loperamide (Imodium)
- Dextropropoxyphene (Darvocet)
- Tapentadol (Nucynta)
- Dextropropoxyphene (Darvocet)
Others:
Mitragyna speciosa (Kratom) Indole alkaloid
Piperidinediones
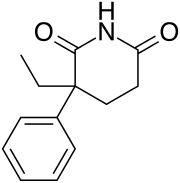
Piperidinediones are a class of depressants that are not used anymore. There are Piperidinediones that are used for other purposes like breast cancer. . The Piperidinedione class is very structurally similar to barbiturates. Some Piperidinediones include Glutethimide, Methyprylon, Pyrithyldione, Glutarimide, and Aminoglutethimide. The first 3 (Glutethimide, Methyprylon, and Pyrithyldione) are central nervous depressants. The Piperidinedione depressants, specifically Glutethimide, are positive modulators of the GABAA anion channel. The drug increases inhibitory GABAergic tone and causes neuro-inhibition of the cortical and limbic systems, observed clinically as a sedative-hypnotic effect. Glutethimide is also a potent inhibitor of the CYP 2D6 enzyme in the liver. This enzyme is responsible for converting many drugs from beta blockers to antidepressants to opioids and opiates. Due to its effects on the conversion of opioids, it was highly abused and mixed with opioids like codeine. Codeine must be metabolized to morphine in the liver to have its psychoactive and analgesic effects. Mixing codeine with the Piperidinedione Glutethimide allowed more codeine to be converted into morphine in the body; thus increasing its effect. These were known as "hits", "cibas and codeine", and "dors and 4s". Glutethimide was believed to be safer than barbiturates, but many people died from the drug. Demand was high in the United States at one point. Production of glutethimide was discontinued in the US in 1993 and in several eastern European countries, most notably Hungary, in 2006.
Glutethimide withdrawal is intense and resembles barbiturate withdrawal. It features hallucinations and delirium typical of a depressant withdrawal. In the 1970s, there were reports of neonatal withdrawal from glutethimide. Infants born to mothers addicted to glutethimide responded well initially, then had recurrence of symptoms about 5 days later, including overactivity, restlessness, tremors, hyperreflexia, hypotonus, vasomotor instability, incessant crying, and general irritability.
Glutethimide withdrawal featured severe agitation, tremor, and seizures which could be fatal.
Overdose causes stupor or coma and respiratory depression.
- Methyprylon (Dimerin, Methyprylone, Noctan, Noludar)
- Pyrithyldione (Presidon, Pyridion, Pyridione, Pyrithyldion, Pyrithyldione)
- Piperidione (Ascron, Dihyprylon, Dihyprylone, Sedulon, Tusseval) (Withdrawan before approval)
- Glutethimide (Doriden)
Quinazolinone
Quinazolinones are a class of depressants that are rarely used anymore. Quinazolinones have powerful sedative, hypnotic, and anxiolytic effects. Quinazolinone's structure is very similar to some antibiotics. Quinazolinone's main mechanism of action is binding to the GABAA receptor.[154] It does not bind to the ethanol, barbiturate, neurosteroid, or benzodiazepine site.[154] Instead, it binds on a site directly between the GABRB2 (β2) and (α1) GABRA1 proteins on the GABAA receptor.[154] The anesthetic etomidate and Anticonvulsant loreclezole may also bind to this site.[154]
Overdosing on quinazolinone sometimes causes effects that are the opposite of quinazolinone-like sedation. The overdose consists of hyperreflexia, vomiting, kidney failure, delirium, hypertonia, coma, myoclonic twitches, somnolence, euphoria, muscular hyperactivity, agitated delirium, tachycardia, and tonic-clonic seizures. In 1982, 2,764 people visited US emergency rooms from overdosing on quinazolinones, specifically Methaqualone.[155] Mixing quinazolines with another depressant is possibly fatal. Death from a quinazolinone overdose is usually caused by death through cardiac or respiratory arrest. Overdose resembles barbiturate/carbamate overdose.
Quinazolinone withdrawal occurs when someone who has become dependent on a quinazolinone ceases usage. Quinazolinone withdrawal resembles ethanol, barbiturate, benzodiazepine, and carbamate withdrawal. It usually consists of restlessness, nausea and vomiting, decreased appetite, tachycardia, insomnia, tremor, hallucinations, delirium, confusion, and seizures; and, which are possibly fatal: EEG photoparoxysmal response, myoclonic twitches, fever, muscle spasms, and irritability.[156]
Methaqualone hydrochloride, quinazolinone anxiolytics and hypnotics are referred to as "quaaludes", "ludes", and "disco biscuits". Methaqualone was very commonly abused in the western world during the 1960s and 1970s. Methaqualone was mainly prescribed for insomnia, as it was thought to be safer than barbiturates and carbamates. Methaqualone became highly abused by many, including celebrities, after its introduction in 1965.[155] Methaqualone was first synthesized in India in 1951 by Indra Kishore Kacker and Syed Husain Zaheer, who were conducting research on finding new antimalarial medications.[157][158] The drug name "Quaalude" (Methaqualone) is a portmanteau, combining the words "quiet interlude". Methaqualone was discontinued in the United States in 1985, mainly due to its psychological addictiveness, widespread abuse, and illegal recreational use. Nonbenzodiazepines, and benzodiazepines are now used to treat insomnia instead. Methaqualone is now a Schedule I substance. Some quinazolinone analogues are still sold online. They come with the risk of seizure.
Large doses of Methaqualone can cause euphoria, disinhibition, increased sexuality, sociability, muscle relaxation, anxiolysis, and sedation. Today, Methaqualone is widely abused in South Africa. Many celebrities have used quinazolinone, most notably Methaqualone. Bill Cosby admitted to casual sex involving recreational use of Methaqualone (Quaaludes).[159][160][161] 18 year old actor Anissa Jones died at 18 from an overdose of cocaine, PCP, Methaqualone, and the barbiturate Seconal. Billy Murcia, a drummer for the rock band New York Dolls, died at 21 when he drowned in a bathtub while overdosing on heroin and Methaqualone.[162]
Cloroqualone was a quinazolinone that bound to the GABAA and sigma-1 receptor. It had useful cough suppressant effects and weaker sedative effects than Methaqualone, but was ultimately withdrawn due to its potential for abuse and overdose.[163]
Diproqualone is a quinazolinone that is still used today. Diproqualone has sedative, anxiolytic, antihistamine and analgesic properties, resulting from its agonist activity at the β subtype of the GABAa receptor, antagonist activity at all histamine receptors, inhibition of the cyclooxygenase-1 enzyme, and possibly its agonist activity at both the Sigma-1 receptor and Sigma-2 receptor. Diproqualone is used primarily for the treatment of inflammatory pain associated with osteoarthritis and rheumatoid arthritis; it is used more rarely for treating insomnia, anxiety and neuralgia. Diproqualone is the only analogue of methaqualone that is still in widespread clinical use due to its useful anti-inflammatory and analgesic effects along with the sedative and anxiolytic actions common to other drugs of this class. There are still some concerns about the potential of diproqualone for abuse and overdose; it is sold not as a pure drug but as the camphosulfonate salt in combination mixtures with other medicines such as ethenzamide.
Etaqualone is a quinazolinone-class depressant. It has sedative, hypnotic, muscle relaxant and central nervous system depressant properties. It was highly abused, and had high risk for overdose. Users would snort or smoke the free base Etaqualone hydrochloride salt.
Methylmethaqualone is an analogue of Methaqualone with similar hypnotic and sedative effects. Methylmethaqualone differs from methaqualone by 4-methylation on the phenyl ring. It produces convulsions at only slightly above the effective sedative dose. It would appear that this compound was sold on the black market in Germany as a designer drug analogue of methaqualone.[164]
Nitromethaqualone is a quinazolinone depressant with ten times more hypnotic and sedative effects than Methaqualone.[165]
Quinazolinones:
- Alfoqualone (Arofuto)
- Cloroqualone
- Diproqualone
- Etaqualone (Aolan, Athinazone, Ethinazone)
- Mebroqualone (MBQ)
- Mecloqualone (Nubarene, Casfen)
- Methaqualone (Quaalude, Sopor, Mandrax)
- Methylmethaqualone
- Nitromethaqualone
- SL-164 (Dicloqualone, DCQ)
Miscellaneous
- Alpha and beta blockers (carvedilol, propranolol, atenolol, etc.)
- Anticholinergics (atropine, hyoscyamine, scopolamine, etc.)
- Anticonvulsants (topiramate, carbamazepine, lamotrigine, etc.)
- Antihistamines (diphenhydramine, doxylamine, promethazine, etc.)
- Antipsychotics (haloperidol, chlorpromazine, clozapine, etc.)
- Hypnotics (zolpidem, zopiclone, chloral hydrate, eszopiclone, etc.)
- Muscle relaxants (baclofen, phenibut, carisoprodol, cyclobenzaprine, etc.)
- Sedatives (gamma-hydroxybutyrate, etc.)
Methods of intake
Combining multiple depressants can be very dangerous because the central nervous system's depressive properties have been proposed to increase exponentially instead of linearly.[166] This characteristic makes depressants a common choice for deliberate overdoses in the case of suicide. The use of alcohol or benzodiazepines along with the usual dose of heroin is often the cause of overdose deaths in opiate addicts.
References
- "Depressant – Definition". Princeton WordNet. Retrieved 28 December 2013.
- "Minimum Legal Age Limits". IARD.org. International Alliance for Responsible Drinking. Archived from the original on 4 May 2016. Retrieved 23 June 2016.
- Ethanol Level at eMedicine
- World Health Organization (August 31, 2009). Clinical Guidelines for Withdrawal Management and Treatment of Drug Dependence in Closed Settings (PDF). World Health Organization, Western Pacific Region. p. 3. ISBN 978-92-9061-430-2. Archived from the original (PDF) on March 12, 2014.
Cannabis is a depressant drug, but it also has hallucinogenic effects.
- Amsterdam, Jan; Nutt, David; Brink, Wim (January 23, 2013). "Generic legislation of new psychoactive drugs" (PDF). J Psychopharmacol. 27 (3): 317–324. doi:10.1177/0269881112474525. PMID 23343598. S2CID 12288500.
Figure 1
- Burgess, Lana (2019-07-30). "Is marijuana a depressant? Everything you need to know". www.medicalnewstoday.com. Retrieved 2023-08-19.
They may reduce anxiety and muscle tension and make a person feel sleepy.
- Jordan, Allan M.; Khan, Tariq H.; Malkin, Hugh; Osborn, Helen M. I. (August 2002). "Synthesis and analysis of urea and carbamate prodrugs as candidates for melanocyte-directed enzyme prodrug therapy (MDEPT)". Bioorganic & Medicinal Chemistry. 10 (8): 2625–2633. doi:10.1016/s0968-0896(02)00097-4. ISSN 0968-0896. PMID 12057651.
- Conermann, Till; Christian, Desirae (2022), "Carisoprodol", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 31971718, retrieved 2022-11-30
- Kulig, Katarzyna; Malawska, Barbara (October 2007). "Carisbamate, a new carbamate for the treatment of epilepsy". IDrugs: The Investigational Drugs Journal. 10 (10): 720–727. ISSN 1369-7056. PMID 17899491.
- Kavelman, D. A.; Lewis, J. A. (1963-11-09). "Clinical Evaluation of a New Antihypertensive Agent: W583 (Mebutamate)". Canadian Medical Association Journal. 89 (19): 993–995. ISSN 0008-4409. PMC 1921904. PMID 14076168.
- Rho, J. M.; Donevan, S. D.; Rogawski, M. A. (March 1997). "Barbiturate-like actions of the propanediol dicarbamates felbamate and meprobamate". The Journal of Pharmacology and Experimental Therapeutics. 280 (3): 1383–1391. ISSN 0022-3565. PMID 9067327.
- "Meprobamate", LiverTox: Clinical and Research Information on Drug-Induced Liver Injury, Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases, 2012, PMID 31644030, retrieved 2022-11-30
- Gonzalez, Lorie A.; Gatch, Michael B.; Taylor, Cynthia M.; Bell-Horner, Cathy L.; Forster, Michael J.; Dillon, Glenn H. (May 2009). "Carisoprodol-Mediated Modulation of GABAA Receptors: In Vitro and in Vivo Studies". The Journal of Pharmacology and Experimental Therapeutics. 329 (2): 827–837. doi:10.1124/jpet.109.151142. ISSN 0022-3565. PMC 2672873. PMID 19244096.
- Twyman, Roy E.; Rogers, Carl J.; Macdonald, Robert L. (March 1989). "Differential regulation of ?-aminobutyric acid receptor channels by diazepam and phenobarbital". Annals of Neurology. 25 (3): 213–220. doi:10.1002/ana.410250302. hdl:2027.42/50330. ISSN 0364-5134. PMID 2471436. S2CID 72023197.
- Twyman, R.; Rogers, C. J.; Macdonald, R. (1989). "Differential regulation of γ‐aminobutyric acid receptor channels by diazepam and phenobarbital". Annals of Neurology. 25 (3): 213–220. doi:10.1002/ANA.410250302. hdl:2027.42/50330. PMID 2471436. S2CID 72023197.
- Ni, Karen; Cary, Margaret; Zarkowski, Paul (October 2007). "Carisoprodol withdrawal induced delirium: A case study". Neuropsychiatric Disease and Treatment. 3 (5): 679–682. ISSN 1176-6328. PMC 2656305. PMID 19300598.
- Spencer, Sade; Brown, Robyn M.; Quintero, Gabriel C.; Kupchik, Yonatan M.; Thomas, Charles A.; Reissner, Kathryn J.; Kalivas, Peter W. (2014-06-18). "α2δ-1 signaling in nucleus accumbens is necessary for cocaine-induced relapse". The Journal of Neuroscience. 34 (25): 8605–8611. doi:10.1523/JNEUROSCI.1204-13.2014. ISSN 1529-2401. PMC 4061396. PMID 24948814.
- Dooley DJ, Taylor CP, Donevan S, Feltner D (2007). "Ca2+ channel alpha2delta ligands: novel modulators of neurotransmission". Trends Pharmacol. Sci. 28 (2): 75–82. doi:10.1016/j.tips.2006.12.006. PMID 17222465.
- Elaine Wyllie; Gregory D. Cascino; Barry E. Gidal; Howard P. Goodkin (17 February 2012). Wyllie's Treatment of Epilepsy: Principles and Practice. Lippincott Williams & Wilkins. p. 423. ISBN 978-1-4511-5348-4.
- Honorio Benzon; James P. Rathmell; Christopher L. Wu; Dennis C. Turk; Charles E. Argoff; Robert W Hurley (11 September 2013). Practical Management of Pain. Elsevier Health Sciences. p. 1006. ISBN 978-0-323-17080-2.
- Fernstrom, John D. (June 2005). "Branched-chain amino acids and brain function". The Journal of Nutrition. 135 (6 Suppl): 1539S–46S. doi:10.1093/jn/135.6.1539S. ISSN 0022-3166. PMID 15930466.
- Sneader, Walter (2005-10-31). Drug Discovery: A History. John Wiley & Sons. ISBN 978-0-470-01552-0.
- Levandovskiy, Igor A; Sharapa, Dmitry I; Shamota, Tatyana V; Rodionov, Vladimir N; Shubina, Tatyana E (2011-02-01). "Conformationally restricted GABA analogs: from rigid carbocycles to cage hydrocarbons". Future Medicinal Chemistry. 3 (2): 223–241. doi:10.4155/fmc.10.287. ISSN 1756-8919. PMID 21428817.
- Bryans, Justin S.; Wustrow, David J. (1999). "3-Substituted GABA analogs with central nervous system activity: A review". Medicinal Research Reviews. 19 (2): 149–77. doi:10.1002/(SICI)1098-1128(199903)19:2<149::AID-MED3>3.0.CO;2-B. PMID 10189176. S2CID 38496241.
- Uchitel, O. D; Di Guilmi, M. N.; Urbano, F. J.; Gonzalez-Inchauspe, C. (2010). "Acute modulation of calcium currents and synaptic transmission by gabapentinoids". Channels (Austin). 4 (6): 490–496. doi:10.4161/chan.4.6.12864. PMID 21150315.
- Sills, G. J. (2006). "The mechanisms of action of gabapentin and pregabalin". Current Opinion in Pharmacology. 6 (1): 108–13. doi:10.1016/j.coph.2005.11.003. PMID 16376147.
- Lapin, I. (2001). "Phenibut (beta-phenyl-GABA): a tranquilizer and nootropic drug". CNS Drug Reviews. 7 (4): 471–481. doi:10.1111/j.1527-3458.2001.tb00211.x. ISSN 1080-563X. PMC 6494145. PMID 11830761.
- Abramets, I. I.; Komissarov, I. V. (June 1985). "[Effect of fenibut on the GABA B receptors of the spinal motor neurons]". Biulleten' Eksperimental'noi Biologii I Meditsiny. 99 (6): 698–700. ISSN 0365-9615. PMID 2861865.
- "Gabapentin – an overview | ScienceDirect Topics". www.sciencedirect.com. Retrieved 2022-04-26.
- "Target Information | Therapeutic Target Database". db.idrblab.net. Retrieved 2022-05-23.
- Douglas Kirsch (10 October 2013). Sleep Medicine in Neurology. John Wiley & Sons. p. 241. ISBN 978-1-118-76417-6.
- Frye, Mark; Moore, Katherine (2009). "Gabapentin and Pregabalin". In Schatzberg, Alan F.; Nemeroff, Charles B. (eds.). The American Psychiatric Publishing Textbook of Psychopharmacology. pp. 767–77. doi:10.1176/appi.books.9781585623860.as38. ISBN 978-1-58562-309-9.
- Garcia-Borreguero, D.; Larrosa, O.; de la Llave, Y.; Verger, K.; Masramon, X.; Hernandez, G. (2002-11-26). "Treatment of restless legs syndrome with gabapentin: a double-blind, cross-over study". Neurology. 59 (10): 1573–1579. doi:10.1212/wnl.59.10.1573. ISSN 0028-3878. PMID 12451200. S2CID 45436475.
- Derry, Sheena; Bell, Rae Frances; Straube, Sebastian; Wiffen, Philip J.; Aldington, Dominic; Moore, R. Andrew (2019-01-23). "Pregabalin for neuropathic pain in adults". The Cochrane Database of Systematic Reviews. 1 (1): CD007076. doi:10.1002/14651858.CD007076.pub3. ISSN 1469-493X. PMC 6353204. PMID 30673120.
- Ryvlin, Philippe; Perucca, Emilio; Rheims, Sylvain (December 2008). "Pregabalin for the management of partial epilepsy". Neuropsychiatric Disease and Treatment. 4 (6): 1211–1224. doi:10.2147/ndt.s4716. ISSN 1176-6328. PMC 2646650. PMID 19337461.
- Derry, Sheena; Cording, Malene; Wiffen, Philip J.; Law, Simon; Phillips, Tudor; Moore, R. Andrew (2016-09-29). "Pregabalin for pain in fibromyalgia in adults". The Cochrane Database of Systematic Reviews. 9 (5): CD011790. doi:10.1002/14651858.CD011790.pub2. ISSN 1469-493X. PMC 6457745. PMID 27684492.
- Baldwin, David S; Ajel, Khalil; Masdrakis, Vasilios G; Nowak, Magda; Rafiq, Rizwan (2013). "Pregabalin for the treatment of generalized anxiety disorder: an update". Neuropsychiatric Disease and Treatment. 9: 883–892. doi:10.2147/NDT.S36453. ISSN 1176-6328. PMC 3699256. PMID 23836974.
- Cappuzzo, Kimberly A (2009). "Treatment of postherpetic neuralgia: focus on pregabalin". Clinical Interventions in Aging. 4: 17–23. ISSN 1176-9092. PMC 2685221. PMID 19503762.
- Lo, Hsiao-Sui; Yang, Chien-Ming; Lo, Helen G.; Lee, Chien-Ying; Ting, Hua; Tzang, Bor-Show (March 2010). "Treatment effects of gabapentin for primary insomnia". Clinical Neuropharmacology. 33 (2): 84–90. doi:10.1097/WNF.0b013e3181cda242. ISSN 1537-162X. PMID 20124884. S2CID 4046961.
- Freynhagen, Rainer; Backonja, Miroslav; Schug, Stephan; Lyndon, Gavin; Parsons, Bruce; Watt, Stephen; Behar, Regina (2016). "Pregabalin for the Treatment of Drug and Alcohol Withdrawal Symptoms: A Comprehensive Review". CNS Drugs. 30 (12): 1191–1200. doi:10.1007/s40263-016-0390-z. ISSN 1172-7047. PMC 5124051. PMID 27848217.
- Sood, Amit; Ebbert, Jon O.; Wyatt, Kirk D.; Croghan, Ivana T.; Schroeder, Darrell R.; Sood, Richa; Hays, J. Taylor (March 2010). "Gabapentin for smoking cessation". Nicotine & Tobacco Research. 12 (3): 300–304. doi:10.1093/ntr/ntp195. ISSN 1462-2203. PMC 2825098. PMID 20081039.
- Kawalec, Paweł; Cierniak, Agnieszka; Pilc, Andrzej; Nowak, Gabriel (April 2015). "Pregabalin for the treatment of social anxiety disorder". Expert Opinion on Investigational Drugs. 24 (4): 585–594. doi:10.1517/13543784.2014.979283. ISSN 1744-7658. PMID 25361817. S2CID 207477337.
- Sokolski, K. N.; Green, C.; Maris, D. E.; DeMet, E. M. (December 1999). "Gabapentin as an adjunct to standard mood stabilizers in outpatients with mixed bipolar symptomatology". Annals of Clinical Psychiatry. 11 (4): 217–222. doi:10.1023/a:1022361412956. ISSN 1040-1237. PMID 10596736. S2CID 8468706.
- Conesa, María‐Llanos; Rojo, Luis‐Miguel; Plumed, Javier; Livianos, Lorenzo (2012-01-16). "Pregabalin in the Treatment of Refractory Bipolar Disorders". CNS Neuroscience & Therapeutics. 18 (3): 269–270. doi:10.1111/j.1755-5949.2011.00289.x. ISSN 1755-5930. PMC 6493626. PMID 22449111.
- Hamrin, V.; Bailey, K. (2001). "Gabapentin and methylphenidate treatment of a preadolescent with attention deficit hyperactivity disorder and bipolar disorder". Journal of Child and Adolescent Psychopharmacology. 11 (3): 301–309. doi:10.1089/10445460152595630. ISSN 1044-5463. PMID 11642481.
- Pandya, K J; Morrow, G R; Roscoe, J A; Hickok, J T; Zhao, H; Pajon, E; Sweeney, T J; Banerjee, T K; Flynn, P J (2005-09-03). "Gabapentin for hot flashes in 420 women with breast cancer: a randomised double-blind placebo-controlled trial". Lancet. 366 (9488): 818–824. doi:10.1016/S0140-6736(05)67215-7. ISSN 0140-6736. PMC 1627210. PMID 16139656.
- "Baclofen". The American Society of Health-System Pharmacists. Retrieved 2011-12-06.
- Lapin I (2001). "Phenibut (beta-phenyl-GABA): a tranquilizer and nootropic drug". CNS Drug Reviews. 7 (4): 471–81. doi:10.1111/j.1527-3458.2001.tb00211.x. PMC 6494145. PMID 11830761.
- Hägg, Staffan; Jönsson, Anna K.; Ahlner, Johan (2020). "Current Evidence on Abuse and Misuse of Gabapentinoids". Drug Safety. 43 (12): 1235–1254. doi:10.1007/s40264-020-00985-6. ISSN 0114-5916. PMC 7686181. PMID 32857333.
- Smith, Blair H; Higgins, Cassie; Baldacchino, Alex; Kidd, Brian; Bannister, Jonathan (August 2012). "Substance misuse of gabapentin". The British Journal of General Practice. 62 (601): 406–407. doi:10.3399/bjgp12X653516. ISSN 0960-1643. PMC 3404313. PMID 22867659.
- Althobaiti, Yusuf S.; Alghorabi, Amal; Alshehri, Fahad S.; Baothman, Bandar; Almalki, Atiah H.; Alsaab, Hashem O.; Alsanie, Walaa; Gaber, Ahmed; Almalki, Hussam; Alghamdi, Abdulrahman S.; Basfer, Ahmad (2020-06-26). "Gabapentin-induced drug-seeking-like behavior: a potential role for the dopaminergic system". Scientific Reports. 10 (1): 10445. Bibcode:2020NatSR..1010445A. doi:10.1038/s41598-020-67318-6. ISSN 2045-2322. PMC 7320158. PMID 32591630.
- "FDA warns about serious breathing problems with seizure and nerve pain medicines gabapentin (Neurontin, Gralise, Horizant) and pregabalin (Lyrica, Lyrica CR)". U.S. Food and Drug Administration (FDA). 19 December 2019. Archived from the original on 22 December 2019. Retrieved 21 December 2019.
 This article incorporates text from this source, which is in the public domain.
This article incorporates text from this source, which is in the public domain. - Gomes, Tara; Juurlink, David N.; Antoniou, Tony; Mamdani, Muhammad M.; Paterson, J. Michael; van den Brink, Wim (2017-10-03). "Gabapentin, opioids, and the risk of opioid-related death: A population-based nested case–control study". PLOS Medicine. 14 (10): e1002396. doi:10.1371/journal.pmed.1002396. ISSN 1549-1277. PMC 5626029. PMID 28972983.
- Kriikku, Pirkko; Ojanperä, Ilkka (July 2021). "Pregabalin and gabapentin in non-opioid poisoning deaths". Forensic Science International. 324: 110830. doi:10.1016/j.forsciint.2021.110830. ISSN 1872-6283. PMID 34000615. S2CID 234770186.
- Elliott, Simon P.; Burke, Timothy; Smith, Christopher (January 2017). "Determining the Toxicological Significance of Pregabalin in Fatalities". Journal of Forensic Sciences. 62 (1): 169–173. doi:10.1111/1556-4029.13263. ISSN 1556-4029. PMID 27864947. S2CID 39480384.
- Kalk, Nicola J.; Chiu, Ching-Ting; Sadoughi, Rasa; Baho, Heli; Williams, Bryn D.; Taylor, David; Copeland, Caroline S. (2022-04-18). "Fatalities associated with gabapentinoids in England (2004–2020)". British Journal of Clinical Pharmacology. 88 (8): 3911–3917. doi:10.1111/bcp.15352. ISSN 1365-2125. PMC 9543893. PMID 35435281. S2CID 248228229.
- Gabapentin for Adults with Neuropathic Pain: A Review of the Clinical Efficacy and Safety. CADTH Rapid Response Reports. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health. 2015. PMID 26180879.
- Toth, Cory (February 2014). "Pregabalin: latest safety evidence and clinical implications for the management of neuropathic pain". Therapeutic Advances in Drug Safety. 5 (1): 38–56. doi:10.1177/2042098613505614. ISSN 2042-0986. PMC 4110876. PMID 25083261.
- Desai, Aaron; Kherallah, Yazan; Szabo, Cheryl; Marawar, Rohit (March 2019). "Gabapentin or pregabalin induced myoclonus: A case series and literature review". Journal of Clinical Neuroscience. 61: 225–234. doi:10.1016/j.jocn.2018.09.019. ISSN 1532-2653. PMID 30381161. S2CID 53165515.
- Isoardi, Katherine Z.; Polkinghorne, Gregory; Harris, Keith; Isbister, Geoffrey K. (December 2020). "Pregabalin poisoning and rising recreational use: a retrospective observational series". British Journal of Clinical Pharmacology. 86 (12): 2435–2440. doi:10.1111/bcp.14348. ISSN 1365-2125. PMC 7688538. PMID 32374500.
- Gibbons, Robert D.; Hur, Kwan; Brown, C. Hendricks; Mann, J. John (December 2010). "Gabapentin and Suicide Attempts". Pharmacoepidemiology and Drug Safety. 19 (12): 1241–1247. doi:10.1002/pds.2036. ISSN 1053-8569. PMC 2992093. PMID 20922708.
- Cross, Aaron L.; Viswanath, Omar; Sherman, Andrew l (2022), "Pregabalin", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 29261857, retrieved 2022-05-21
- Read, Stephanie H.; Giannakeas, Vasily; Pop, Paula; Bronskill, Susan E.; Herrmann, Nathan; Chen, Simon; Luke, Miles J.; Wu, Wei; McCarthy, Lisa M.; Austin, Peter C.; Normand, Sharon-Lise (October 2021). "Evidence of a gabapentinoid and diuretic prescribing cascade among older adults with lower back pain". Journal of the American Geriatrics Society. 69 (10): 2842–2850. doi:10.1111/jgs.17312. ISSN 1532-5415. PMID 34118076. S2CID 235412378.
- Quintero, Gabriel C (2017-02-09). "Review about gabapentin misuse, interactions, contraindications and side effects". Journal of Experimental Pharmacology. 9: 13–21. doi:10.2147/JEP.S124391. ISSN 1179-1454. PMC 5308580. PMID 28223849.
- "Pregabalin Use During Pregnancy". Drugs.com. Retrieved 2022-06-11.
- Schifano, Fabrizio (2014-06-01). "Misuse and Abuse of Pregabalin and Gabapentin: Cause for Concern?". CNS Drugs. 28 (6): 491–496. doi:10.1007/s40263-014-0164-4. ISSN 1179-1934. PMID 24760436. S2CID 4508086.
- Ishikawa, Hayahito; Takeshima, Masahiro; Ishikawa, Hiroyasu; Ayabe, Naoko; Ohta, Hidenobu; Mishima, Kazuo (September 2021). "Pregabalin withdrawal in patients without psychiatric disorders taking a regular dose of pregabalin: A case series and literature review". Neuropsychopharmacology Reports. 41 (3): 434–439. doi:10.1002/npr2.12195. ISSN 2574-173X. PMC 8411313. PMID 34382380.
- Hellwig, Thaddaus R.; Hammerquist, Rhonda; Termaat, Jill (2010-06-01). "Withdrawal symptoms after gabapentin discontinuation". American Journal of Health-System Pharmacy. 67 (11): 910–912. doi:10.2146/ajhp090313. ISSN 1535-2900. PMID 20484214.
- Alvis, Bret D.; Sobey, Christopher M. (January 2017). "Oral Baclofen Withdrawal Resulting in Progressive Weakness and Sedation Requiring Intensive Care Admission". The Neurohospitalist. 7 (1): 39–40. doi:10.1177/1941874416637404. ISSN 1941-8744. PMC 5167087. PMID 28042369.
- Hardman, Matthew I.; Sprung, Juraj; Weingarten, Toby N. (May 2019). "Acute phenibut withdrawal: A comprehensive literature review and illustrative case report". Bosnian Journal of Basic Medical Sciences. 19 (2): 125–129. doi:10.17305/bjbms.2018.4008. ISSN 1512-8601. PMC 6535394. PMID 30501608.
- Mohammed, Imran; Hussain, Asif (2004-08-09). "Intrathecal baclofen withdrawal syndrome- a life-threatening complication of baclofen pump: A case report". BMC Clinical Pharmacology. 4: 6. doi:10.1186/1472-6904-4-6. ISSN 1472-6904. PMC 514562. PMID 15301690.
- "SwissTargetPrediction". www.swisstargetprediction.ch. Retrieved 2022-12-21.
- "Target Report Card". www.ebi.ac.uk. Retrieved 2022-12-21.
- genophore. "DEXTROTHYROXINE". genophore.com. Retrieved 2022-12-21.
- O'connell, Ted; Kaye, Lily; Plosay, John J. III (2000-12-01). "Gamma-Hydroxybutyrate (GHB): A Newer Drug of Abuse". American Family Physician. 62 (11): 2478–2482. PMID 11130233.
- Cash, Christopher D. (1994-06-01). "Gammahydroxybutyrate: An overview of the pros and cons for it being a neurotransmitter and/or a useful therapeutic agent". Neuroscience & Biobehavioral Reviews. 18 (2): 291–304. doi:10.1016/0149-7634(94)90031-0. ISSN 0149-7634. PMID 7914688. S2CID 42104511.
- Fait, Aaron; Yellin, Ayelet; Fromm, Hillel (2006). "GABA and GHB Neurotransmitters in Plants and Animals". In Baluška, František; Mancuso, Stefano; Volkmann, Dieter (eds.). Communication in Plants. pp. 171–185. doi:10.1007/978-3-540-28516-8_12. ISBN 978-3-540-28516-8.
{{cite book}}:|work=ignored (help) - Elliott, Simon; Burgess, Victoria (2005-07-16). "The presence of gamma-hydroxybutyric acid (GHB) and gamma-butyrolactone (GBL) in alcoholic and non-alcoholic beverages". Forensic Science International. 151 (2): 289–292. doi:10.1016/j.forsciint.2005.02.014. ISSN 0379-0738. PMID 15939164.
- Nicholson, Katherine L.; Balster, Robert L. (2001-06-01). "GHB: a new and novel drug of abuse". Drug and Alcohol Dependence. 63 (1): 1–22. doi:10.1016/S0376-8716(00)00191-5. ISSN 0376-8716. PMID 11297827.
- Wedin, Gregory P.; Hornfeldt, Carl S.; Ylitalo, Lisa M. (2006-01-01). "The Clinical Development of γ-Hydroxybutyrate (GHB)". Current Drug Safety. 1 (1): 99–106. doi:10.2174/157488606775252647. PMID 18690919.
- Tunnicliff, Godfrey (1997-01-01). "Sites of Action of Gamma-Hydroxybutyrate (GHB)–A Neuroactive Drug with Abuse Potential". Journal of Toxicology: Clinical Toxicology. 35 (6): 581–590. doi:10.3109/15563659709001236. ISSN 0731-3810. PMID 9365423.
- Boscolo-Berto, Rafael; Viel, Guido; Montagnese, Sara; Raduazzo, Daniella I.; Ferrara, Santo D.; Dauvilliers, Yves (2012-10-01). "Narcolepsy and effectiveness of gamma-hydroxybutyrate (GHB): A systematic review and meta-analysis of randomized controlled trials". Sleep Medicine Reviews. 16 (5): 431–443. doi:10.1016/j.smrv.2011.09.001. ISSN 1087-0792. PMID 22055895.
- Xu, Xiao-Min; Wei, You-Dong; Liu, Yang; Li, Zuo-Xiao (2019-12-01). "Gamma-hydroxybutyrate (GHB) for narcolepsy in adults: an updated systematic review and meta-analysis". Sleep Medicine. 64: 62–70. doi:10.1016/j.sleep.2019.06.017. ISSN 1389-9457. PMID 31671326. S2CID 198286153.
- "Pharmacokinetics of Gammahydroxybutyrate (GHB) in Narcoleptic Patients". academic.oup.com. Retrieved 2023-03-28.
- "The role of gamma-hydroxybutyric acid in the treatment of alcoholism: from animal to clinical studies". academic.oup.com. Retrieved 2023-03-28.
- "Does Gamma-Hydroxybutyrate (GHB) Have a Role in the Treatment of Alcoholism?". academic.oup.com. Retrieved 2023-03-28.
- Maremmani, Angelo Giovanni Icro; Pani, Pier Paolo; Rovai, Luca; Pacini, Matteo; Dell’Osso, Liliana; Maremmani, Icro (July 2011). "Long-Term γ-Hydroxybutyric Acid (GHB) and Disulfiram Combination Therapy in GHB Treatment-Resistant Chronic Alcoholics". International Journal of Environmental Research and Public Health. 8 (7): 2816–2827. doi:10.3390/ijerph8072816. ISSN 1660-4601. PMC 3155331. PMID 21845160.
- Caputo, Fabio; Vignoli, Teo; Maremmani, Icro; Bernardi, Mauro; Zoli, Giorgio (June 2009). "Gamma Hydroxybutyric Acid (GHB) for the Treatment of Alcohol Dependence: A Review". International Journal of Environmental Research and Public Health. 6 (6): 1917–1929. doi:10.3390/ijerph6061917. ISSN 1660-4601. PMC 2705225. PMID 19578468.
- Alshaikh, Mashael K.; Gacuan, Divine; George, Smitha; Sharif, Munir; BaHammam, Ahmed S. (January 2011). "Long-Term Follow-Up of Patients With Narcolepsy-Cataplexy Treated With Sodium Oxybate (Xyrem)". Clinical Neuropharmacology. 34 (1): 1–4. doi:10.1097/WNF.0b013e318203d415. ISSN 0362-5664. PMID 21206362. S2CID 206127007.
- U. S. Xyrem Multicenter Study Group (2004-03-01). "Sodium oxybate demonstrates long-term efficacy for the treatment of cataplexy in patients with narcolepsy". Sleep Medicine. 5 (2): 119–123. doi:10.1016/j.sleep.2003.11.002. ISSN 1389-9457. PMID 15033130.
- Carter, Lawrence P.; Pardi, Daniel; Gorsline, Jane; Griffiths, Roland R. (2009-09-01). "Illicit gamma-hydroxybutyrate (GHB) and pharmaceutical sodium oxybate (Xyrem®): Differences in characteristics and misuse". Drug and Alcohol Dependence. 104 (1): 1–10. doi:10.1016/j.drugalcdep.2009.04.012. ISSN 0376-8716. PMC 2713368. PMID 19493637.
- Wang, Y. Grace; Swick, Todd J.; Carter, Lawrence P.; Thorpy, Michael J.; Benowitz, Neal L. (2009-08-15). "Safety Overview of Postmarketing and Clinical Experience of Sodium Oxybate (Xyrem): Abuse, Misuse, Dependence, and Diversion". Journal of Clinical Sleep Medicine. 05 (4): 365–371. doi:10.5664/jcsm.27549. ISSN 1550-9389.
- Bay, Tina; Eghorn, Laura F.; Klein, Anders B.; Wellendorph, Petrine (2014-01-15). "GHB receptor targets in the CNS: Focus on high-affinity binding sites". Biochemical Pharmacology. 87 (2): 220–228. doi:10.1016/j.bcp.2013.10.028. ISSN 0006-2952. PMID 24269284.
- Carter, Lawrence P.; Koek, Wouter; France, Charles P. (2009-01-01). "Behavioral analyses of GHB: Receptor mechanisms". Pharmacology & Therapeutics. 121 (1): 100–114. doi:10.1016/j.pharmthera.2008.10.003. ISSN 0163-7258. PMC 2631377. PMID 19010351.
- Kamal, Rama M.; Noorden, Martijn S. van; Franzek, Ernst; Dijkstra, Boukje A. G.; Loonen, Anton J. M.; Jong, Cornelius A. J. De (2016). "The Neurobiological Mechanisms of Gamma-Hydroxybutyrate Dependence and Withdrawal and Their Clinical Relevance: A Review". Neuropsychobiology. 73 (2): 65–80. doi:10.1159/000443173. ISSN 0302-282X. PMID 27003176. S2CID 33389634.
- Ingels, Marianne; Rangan, Cyrus; Bellezzo, Joseph; Clark, Richard F (2000-07-01). "Coma and respiratory depression following the ingestion of GHB and its precursors: Three cases11Selected Topics: Toxicology is coordinated by Kenneth Kulig, MD, of Denver, Colorado". The Journal of Emergency Medicine. 19 (1): 47–50. doi:10.1016/S0736-4679(00)00188-8. ISSN 0736-4679. PMID 10863118.
- Roth, R. H.; Giarman, N. J. (1968-05-01). "Evidence that central nervous system depression by 1,4-butanediol is mediated through a metabolite, gamma-hydroxybutyrate". Biochemical Pharmacology. 17 (5): 735–739. doi:10.1016/0006-2952(68)90010-5. ISSN 0006-2952. PMID 5649891.
- Maitre, Michel; Ratomponirina, Charline; Gobaille, Serge; Hodé, Yann; Hechler, Viviane (1994-04-21). "Displacement of [3H]γ-hydroxybutyrate binding by benzamide neuroleptics and prochlorperazine but not by other antipsychotics". European Journal of Pharmacology. 256 (2): 211–214. doi:10.1016/0014-2999(94)90248-8. ISSN 0014-2999. PMID 7914168.
- Ratomponirina, Charline; Gobaille, Serge; Hodé, Yann; Kemmel, Véronique; Maitre, Michel (1998-04-10). "Sulpiride, but not haloperidol, up-regulates γ-hydroxybutyrate receptors in vivo and in cultured cells". European Journal of Pharmacology. 346 (2): 331–337. doi:10.1016/S0014-2999(98)00068-5. ISSN 0014-2999. PMID 9652377.
- Viviani, Roberto; Graf, Heiko; Wiegers, Maike; Abler, Birgit (2013-09-01). "Effects of amisulpride on human resting cerebral perfusion". Psychopharmacology. 229 (1): 95–103. doi:10.1007/s00213-013-3091-z. ISSN 1432-2072. PMID 23584671. S2CID 253740656.
- Ferris, Trevor J.; Went, Michael J. (2012-03-10). "Synthesis, characterisation and detection of gamma-hydroxybutyrate salts" (PDF). Forensic Science International. 216 (1): 158–162. doi:10.1016/j.forsciint.2011.09.014. ISSN 0379-0738. PMID 22014974.
- Wolnik, Karen A.; Heitkemper, Douglas T.; Crowe, John B.; Barnes, Barbara S.; Brueggemeyer, Thomas W. (1995-01-01). "Application of inductively coupled plasma atomic emission and mass spectrometry to forensic analysis of sodium gamma hydroxy butyrate and ephedrine hydrochloride. Invited lecture". Journal of Analytical Atomic Spectrometry. 10 (3): 177–181. doi:10.1039/JA9951000177. ISSN 1364-5544.
- Heo, Young-A (2022-05-01). "Calcium, Magnesium, Potassium and Sodium Oxybates (Xywav®) in Sleep Disorders: A Profile of Its Use". CNS Drugs. 36 (5): 541–549. doi:10.1007/s40263-022-00912-6. ISSN 1179-1934. PMC 9095545. PMID 35357671.
- Tunnicliff, Godfrey; Raess, Beat U (2002-02-01). "Gamma-Hydroxybutyrate (orphan medical)". Current Opinion in Investigational Drugs. 3 (2): 278–283. ISSN 2040-3429. PMID 12020060.
- Strunc, Michael J.; Black, Jed; Lillaney, Prasheel; Profant, Judi; Mills, Sherice; Bujanover, Shay; Thorpy, Michael J. (2021-03-01). "The Xyrem® (Sodium Oxybate) Risk Evaluation and Mitigation Strategy (REMS) Program in the USA: Results From 2016 to 2017". Drugs - Real World Outcomes. 8 (1): 15–28. doi:10.1007/s40801-020-00223-6. ISSN 2198-9788. PMC 7984153. PMID 33439474.
- Yan, Han Helen (March 2013). "Off-Label Promotion Is Protected Speech: Second Circuit Sweeps Away Pharmaceutical Representative's Misbranding Conviction Under the First Amendment – United States v. Caronia". American Journal of Law & Medicine. 39 (1): 189–192. doi:10.1017/S0098858800000150. ISSN 0098-8588. S2CID 203716949.
- Tay, Emma; Lo, Wing Kwan Winky; Murnion, Bridin (2022-12-31). "Current Insights on the Impact of Gamma-Hydroxybutyrate (GHB) Abuse". Substance Abuse and Rehabilitation. 13: 13–23. doi:10.2147/SAR.S315720. PMC 8843350. PMID 35173515.
- Zvosec, Deborah L.; Smith, Stephen W.; Hall, Brad J. (2009-04-01). "Three deaths associated with use of Xyrem®". Sleep Medicine. 10 (4): 490–493. doi:10.1016/j.sleep.2009.01.005. ISSN 1389-9457. PMID 19269893.
- "Suspected GHB Overdoses in the Emergency Department". academic.oup.com. Retrieved 2023-03-28.
- Degenhardt, Louisa; Darke, Shane; Dillon, Paul (February 2003). "The prevalence and correlates of gamma-hydroxybutyrate (GHB) overdose among Australian users: GHB overdose among Australian users". Addiction. 98 (2): 199–204. doi:10.1046/j.1360-0443.2003.00265.x. PMID 12534425.
- van Amsterdam, Jan G. C.; Brunt, Tibor M.; McMaster, Minni T. B.; Niesink, Raymond J. M. (2012-04-01). "Possible long-term effects of γ-hydroxybutyric acid (GHB) due to neurotoxicity and overdose". Neuroscience & Biobehavioral Reviews. 36 (4): 1217–1227. doi:10.1016/j.neubiorev.2012.02.002. ISSN 0149-7634. PMID 22342779. S2CID 207089557.
- Venzi, Marcello; Di Giovanni, Giuseppe; Crunelli, Vincenzo (February 2015). "A Critical Evaluation of the Gamma-Hydroxybutyrate (GHB) Model of Absence Seizures". CNS Neuroscience & Therapeutics. 21 (2): 123–140. doi:10.1111/cns.12337. PMC 4335601. PMID 25403866.
- Steele, M T; Watson, W A (1995-07-01). "Acute poisoning from gamma hydroxybutyrate (GHB)". Missouri Medicine. 92 (7): 354–357. ISSN 0026-6620. PMID 7651315.
- Degenhardt, Louisa; Darke, Shane; Dillon, Paul (2002-06-01). "GHB use among Australians: characteristics, use patterns and associated harm". Drug and Alcohol Dependence. 67 (1): 89–94. doi:10.1016/S0376-8716(02)00017-0. ISSN 0376-8716. PMID 12062782.
- Davis, Lori L.; Trivedi, Madhukar; Choate, Amy; Kramer, Gerald L.; Petty, Frederick (1997-04-01). "Growth hormone response to the GABAB agonist baclofen in major depressive disorder". Psychoneuroendocrinology. 22 (3): 129–140. doi:10.1016/S0306-4530(96)00048-0. ISSN 0306-4530. PMID 9203224. S2CID 29674330.
- Gamel-Didelon, Katia; Corsi, Claudia; Pepeu, Giancarlo; Jung, Heike; Gratzl, Manfred; Mayerhofer, Artur (2002). "An Autocrine Role for Pituitary GABA: Activation of GABA-B Receptors and Regulation of Growth Hormone Levels". Neuroendocrinology. 76 (3): 170–177. doi:10.1159/000064523. ISSN 0028-3835. PMID 12218349. S2CID 18676115.
- Son, Seong Uk; Jang, Soojin; Kang, Byunghoon; Kim, Junseok; Lim, Jaewoo; Seo, Seungbeom; Kang, Taejoon; Jung, Juyeon; Lee, Kyu-Sun; Kim, Hyungjun; Lim, Eun-Kyung (2021-11-15). "Colorimetric paper sensor for visual detection of date-rape drug γ-hydroxybutyric acid (GHB)". Sensors and Actuators B: Chemical. 347: 130598. doi:10.1016/j.snb.2021.130598. ISSN 0925-4005.
- Zhai, Duanting; Tan, Yong Qiao Elton; Xu, Wang; Chang, Young-Tae (2014-02-18). "Development of a fluorescent sensor for illicit date rape drug GHB". Chemical Communications. 50 (22): 2904–2906. doi:10.1039/C3CC49603A. ISSN 1364-548X. PMID 24492471.
- Carter, Lawrence P.; Wu, Huifang; Chen, Weibin; Cruz, Christopher M.; Lamb, R. J.; Koek, Wouter; Coop, Andy; France, Charles P. (2004-01-01). "Effects of γ-Hydroxybutyrate (GHB) on Schedule-Controlled Responding in Rats: Role of GHB and GABAB Receptors". Journal of Pharmacology and Experimental Therapeutics. 308 (1): 182–188. doi:10.1124/jpet.103.058909. ISSN 0022-3565. PMID 14569056. S2CID 753852.
- Hu, R. Q; Banerjee, P. K; Snead III, O. C (2000-03-01). "Regulation of γ-aminobutyric acid (GABA) release in cerebral cortex in the γ-hydroxybutyric acid (GHB) model of absence seizures in rat". Neuropharmacology. 39 (3): 427–439. doi:10.1016/S0028-3908(99)00152-5. ISSN 0028-3908. PMID 10698009. S2CID 54323081.
- Iii, O. Carter Snead (August 1988). "γ-Hydroxybutyrate Model of Generalized Absence Seizures: Further Characterization and Comparison with Other Absence Models". Epilepsia. 29 (4): 361–368. doi:10.1111/j.1528-1157.1988.tb03732.x. ISSN 0013-9580. PMID 3391142. S2CID 221733630.
- Mamelak, Mortimer (1989-12-01). "Gammahydroxybutyrate: An endogenous regulator of energy metabolism". Neuroscience & Biobehavioral Reviews. 13 (4): 187–198. doi:10.1016/S0149-7634(89)80053-3. ISSN 0149-7634. PMID 2691926. S2CID 20217078.
- McDonough, Michael; Kennedy, Noel; Glasper, Anthony; Bearn, Jenny (2004-07-15). "Clinical features and management of gamma-hydroxybutyrate (GHB) withdrawal: a review". Drug and Alcohol Dependence. 75 (1): 3–9. doi:10.1016/j.drugalcdep.2004.01.012. ISSN 0376-8716. PMID 15225884.
- van Noorden, Martijn S; Kamal, Rama; de Jong, Cor A J; Vergouwen, A C M Ton; Zitman, Frans G (2010-01-01). "[Gamma-hydroxybutyric acid (GHB) dependence and the GHB withdrawal syndrome: diagnosis and treatment]". Nederlands Tijdschrift voor Geneeskunde. 154: A1286. ISSN 1876-8784. PMID 21040601.
- Dyer, Jo Ellen; Roth, Brett; Hyma, Bruce A. (2001-02-01). "Gamma-hydroxybutyrate withdrawal syndrome". Annals of Emergency Medicine. 37 (2): 147–153. doi:10.1067/mem.2001.112985. ISSN 0196-0644. PMID 11174231.
- Wolf, Casper J. H.; Beurmanjer, Harmen; Dijkstra, Boukje A. G.; Geerlings, Alexander C.; Spoelder, Marcia; Homberg, Judith R.; Schellekens, Arnt F. A. (January 2021). "Characterization of the GHB Withdrawal Syndrome". Journal of Clinical Medicine. 10 (11): 2333. doi:10.3390/jcm10112333. ISSN 2077-0383. PMC 8199158. PMID 34073640.
- Lingford-Hughes, Anne; Patel, Yash; Bowden-Jones, Owen; Crawford, Mike J.; Dargan, Paul I.; Gordon, Fabiana; Parrott, Steve; Weaver, Tim; Wood, David M. (2016-09-27). "Improving GHB withdrawal with baclofen: study protocol for a feasibility study for a randomised controlled trial". Trials. 17 (1): 472. doi:10.1186/s13063-016-1593-9. ISSN 1745-6215. PMC 5039898. PMID 27677382.
- Bennett, W. R. Murray; Wilson, Lawrence G.; Roy-Byrne, Peter P. (2007-09-01). "Gamma-Hydroxybutyric Acid (GHB) Withdrawal: A Case Report". Journal of Psychoactive Drugs. 39 (3): 293–296. doi:10.1080/02791072.2007.10400616. ISSN 0279-1072. PMID 18159783. S2CID 44864947.
- van Noorden, Martijn S.; van Dongen, Lieselotte C. A. M.; Zitman, Frans G.; Vergouwen, Ton (A. )C. M. (2009-07-01). "Gamma-hydroxybutyrate withdrawal syndrome: dangerous but not well-known". General Hospital Psychiatry. 31 (4): 394–396. doi:10.1016/j.genhosppsych.2008.11.001. ISSN 0163-8343. PMID 19555805.
- Dang, Amit; Garg, Amit; Rataboli, Padmanabh V. (October 2011). "Role of Zolpidem in the Management of Insomnia: Role of Zolpidem". CNS Neuroscience & Therapeutics. 17 (5): 387–397. doi:10.1111/j.1755-5949.2010.00158.x. PMC 6493830. PMID 20553305.
- Casida, John E. (1993). "Insecticide action at the GABA-gated chloride channel: Recognition, progress, and prospects". Archives of Insect Biochemistry and Physiology. 22 (1–2): 13–23. doi:10.1002/arch.940220104. ISSN 0739-4462. PMID 7679302.
- Sigel, E. (2002-08-01). "Mapping of the Benzodiazepine Recognition Site on GABA-A Receptors". Current Topics in Medicinal Chemistry. 2 (8): 833–839. doi:10.2174/1568026023393444. PMID 12171574.
- PhD, Hugh C. Hemmings, BS, MD; MD, Talmage D. Egan (2013-01-25). Pharmacology and Physiology for Anesthesia: Foundations and Clinical Application. Elsevier Health Sciences. ISBN 978-1-4377-1679-5.
{{cite book}}: CS1 maint: multiple names: authors list (link) - Dhaliwal, Armaan; Gupta, Mohit (2022), "Physiology, Opioid Receptor", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 31536249, retrieved 2023-02-10
- New, David C.; Wong, Yung H. (2002). "The ORL1 receptor: molecular pharmacology and signalling mechanisms". Neuro-Signals. 11 (4): 197–212. doi:10.1159/000065432. ISSN 1424-862X. PMID 12393946. S2CID 38056310.
- Purves, Dale; Augustine, George J.; Fitzpatrick, David; Katz, Lawrence C.; LaMantia, Anthony-Samuel; McNamara, James O.; Williams, S. Mark (2001). "Nociceptors". Neuroscience. 2nd Edition.
- Mallik, Adiel; Chanda, Mona Lisa; Levitin, Daniel J. (2017-02-08). "Anhedonia to music and mu-opioids: Evidence from the administration of naltrexone". Scientific Reports. 7 (1): 41952. Bibcode:2017NatSR...741952M. doi:10.1038/srep41952. ISSN 2045-2322. PMC 5296903. PMID 28176798.
- Chaudhry, Shazia R.; Gossman, William (2022), "Biochemistry, Endorphin", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 29262177, retrieved 2023-02-10
- Furlan AD, Sandoval JA, Mailis-Gagnon A, Tunks E (May 2006). "Opioids for chronic noncancer pain: a meta-analysis of effectiveness and side effects". CMAJ. 174 (11): 1589–94. doi:10.1503/cmaj.051528. PMC 1459894. PMID 16717269.
- Ho, Jo-Hao; Stahl, Edward L.; Schmid, Cullen L.; Scarry, Sarah M.; Aubé, Jeffrey; Bohn, Laura M. (2018-08-07). "G protein signaling–biased agonism at the κ-opioid receptor is maintained in striatal neurons". Science Signaling. 11 (542): eaar4309. doi:10.1126/scisignal.aar4309. ISSN 1945-0877. PMC 6373773. PMID 30087177.
- Chavkin, Charles (August 2018). "Kappa-opioid antagonists as stress resilience medications for the treatment of alcohol use disorders". Neuropsychopharmacology. 43 (9): 1803–1804. doi:10.1038/s41386-018-0046-4. ISSN 0893-133X. PMC 6046055. PMID 29752444.
- Jutkiewicz, Emily M.; Baladi, Michelle G.; Folk, John E.; Rice, Kenner C.; Woods, James H. (2006-06-01). "The Convulsive and Electroencephalographic Changes Produced by Nonpeptidic δ-Opioid Agonists in Rats: Comparison with Pentylenetetrazol". Journal of Pharmacology and Experimental Therapeutics. 317 (3): 1337–1348. doi:10.1124/jpet.105.095810. ISSN 0022-3565. PMID 16537798. S2CID 21838231.
- "OPRL1 opioid related nociceptin receptor 1 [Homo sapiens (human)] - Gene - NCBI". www.ncbi.nlm.nih.gov. Retrieved 2023-02-10.
- Calo', Girolamo; Guerrini, Remo; Rizzi, Anna; Salvadori, Severo; Regoli, Domenico (April 2000). "Pharmacology of nociceptin and its receptor: a novel therapeutic target". British Journal of Pharmacology. 129 (7): 1261–1283. doi:10.1038/sj.bjp.0703219. ISSN 0007-1188. PMC 1571975. PMID 10742280.
- Theriot, Jonathan; Sabir, Sarah; Azadfard, Mohammadreza (2022), "Opioid Antagonists", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 30725764, retrieved 2023-02-11
- Rzasa Lynn, Rachael; Galinkin, JL (January 2018). "Naloxone dosage for opioid reversal: current evidence and clinical implications". Therapeutic Advances in Drug Safety. 9 (1): 63–88. doi:10.1177/2042098617744161. ISSN 2042-0986. PMC 5753997. PMID 29318006.
- Sun, Hsiao Lun (March 1998). "Naloxone-Precipitated Acute Opioid Withdrawal Syndrome After Epidural Morphine". Anesthesia & Analgesia. 86 (3): 544–545. doi:10.1213/00000539-199803000-00019. ISSN 0003-2999. PMID 9495411.
- Introduction: The Pharmacology of Buprenorphine, Precipitated Withdrawal & Management of Adverse Effects
- Bourdy, Romain; Barrot, Michel (2012-11-01). "A new control center for dopaminergic systems: pulling the VTA by the tail". Trends in Neurosciences. 35 (11): 681–690. doi:10.1016/j.tins.2012.06.007. ISSN 0166-2236. PMID 22824232. S2CID 43434322.
- Barrot, Michel; Sesack, Susan R.; Georges, François; Pistis, Marco; Hong, Simon; Jhou, Thomas C. (2012-10-10). "Braking Dopamine Systems: A New GABA Master Structure for Mesolimbic and Nigrostriatal Functions". The Journal of Neuroscience. 32 (41): 14094–14101. doi:10.1523/JNEUROSCI.3370-12.2012. ISSN 0270-6474. PMC 3513755. PMID 23055478.
- "γ-Aminobutyric acid", Wikipedia, 2023-02-06, retrieved 2023-02-11
- Mars, Sarah G; Ondocsin, Jeff; Ciccarone, Daniel (2018). "Sold As Heroin: Perceptions and Use of an Evolving Drug in Baltimore, MD". Journal of Psychoactive Drugs. 50 (2): 167–176. doi:10.1080/02791072.2017.1394508. ISSN 0279-1072. PMC 6114137. PMID 29211971.
- Misailidi, Nektaria; Papoutsis, Ioannis; Nikolaou, Panagiota; Dona, Artemisia; Spiliopoulou, Chara; Athanaselis, Sotiris (2018). "Fentanyls continue to replace heroin in the drug arena: the cases of ocfentanil and carfentanil". Forensic Toxicology. 36 (1): 12–32. doi:10.1007/s11419-017-0379-4. ISSN 1860-8965. PMC 5754389. PMID 29367860.
- Hammer, Harriet; Bader, Benjamin M.; Ehnert, Corina; Bundgaard, Christoffer; Bunch, Lennart; Hoestgaard-Jensen, Kirsten; Schroeder, Olaf H.-U.; Bastlund, Jesper F.; Gramowski-Voß, Alexandra; Jensen, Anders A. (August 2015). "A Multifaceted GABAA Receptor Modulator: Functional Properties and Mechanism of Action of the Sedative-Hypnotic and Recreational Drug Methaqualone (Quaalude)". Molecular Pharmacology. 88 (2): 401–420. doi:10.1124/mol.115.099291. ISSN 0026-895X. PMC 4518083. PMID 26056160.
- "Methaqualone (Encyclopedia of Drugs and Addictive Substances) - eNotes.com". 2012-02-23. Archived from the original on 2012-02-23. Retrieved 2022-12-01.
- "Quaaludes Addiction and Abuse, Statistics, Signs, Symptoms & Side Effects". Addiction Hope. Retrieved 2022-12-01.
- "Lawrence Journal-World - Google News Archive Search". news.google.com. Retrieved 2022-12-01.
- van Zyl, Etienne F. (2001-11-01). "A survey of reported synthesis of methaqualone and some positional and structural isomers". Forensic Science International. 122 (2): 142–149. doi:10.1016/S0379-0738(01)00484-4. ISSN 0379-0738. PMID 11672968.
- Moghe, Sonia (2015-07-25). "Cosby deposition: Quaaludes came from L.A. gynecologist". CNN. Retrieved 2022-12-01.
- Bowley, Graham; Ember, Sydney (2015-07-19). "Bill Cosby, in Deposition, Said Drugs and Fame Helped Him Seduce Women". The New York Times. ISSN 0362-4331. Retrieved 2022-12-01.
- "Gloria Allred wins Cobb Energy Bill Cosby concert protest case | Radio & TV Talk". 2016-09-11. Archived from the original on 2016-09-11. Retrieved 2022-12-01.
- "New York Doll Murcia died here". shadyoldlady.com. Retrieved 2022-12-01.
- PubChem. "Cloroqualone". pubchem.ncbi.nlm.nih.gov. Retrieved 2022-12-01.
- "Microgram Journal" (PDF). 2011-07-19. Archived from the original (PDF) on 2011-07-19. Retrieved 2022-12-01.
- Szirmai, A. (November 1963). "Pharmacological and Therapeutic Studies with a New Quinazolone Derivative, Nitromethaqualone". Therapeutische Umschau. Revue Therapeutique. 20: 542–546. ISSN 0040-5930. PMID 14101319.
- Avery, S N; Clauss, J A; Blackford, J U (2015-06-24). "The Human BNST: Functional Role in Anxiety and Addiction". Neuropsychopharmacology. 41 (1): 126–141. doi:10.1038/npp.2015.185. ISSN 0893-133X. PMC 4677124. PMID 26105138.
External links
- Painfully Obvious – A Community Resource
- Fact sheets and Harm Reduction Strategies About Depressants and Other Recreational Drugs
- U.S. Department of Human and Health Services: Drug Categories for Substances of Abuse
- About Psychotropic Medications: Quick Reference to Medications Used in Mental Health Archived 2019-07-01 at the Wayback Machine
- National Institute on Drug Abuse: "NIDA for Teens: Prescription Depressant Medications".
Major chemical drug groups – based upon the Anatomical Therapeutic Chemical Classification System | |
|---|---|
| gastrointestinal tract / metabolism (A) | |
| blood and blood forming organs (B) | |
| cardiovascular system (C) | |
| skin (D) | |
| genitourinary system (G) | |
| endocrine system (H) | |
| infections and infestations (J, P, QI) | |
| malignant disease (L01–L02) | |
| immune disease (L03–L04) | |
| muscles, bones, and joints (M) | |
| brain and nervous system (N) |
|
| respiratory system (R) | |
| sensory organs (S) | |
| other ATC (V) | |
| |