Biliary colic
Biliary colic, also known as symptomatic cholelithiasis, a gallbladder attack or gallstone attack, is when a colic (sudden pain) occurs due to a gallstone temporarily blocking the cystic duct.[1] Typically, the pain is in the right upper part of the abdomen, and can be severe.[2] Pain usually lasts from 15 minutes to a few hours.[1] Often, it occurs after eating a heavy meal, or during the night.[1] Repeated attacks are common.[3]
| Biliary colic | |
|---|---|
| Other names | Gallstone attack, gallbladder attack |
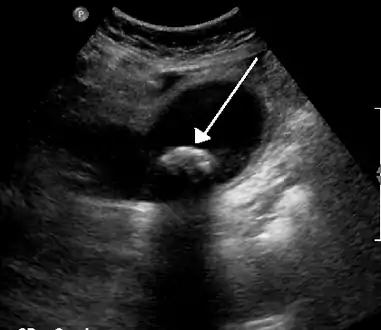 | |
| Biliary colic is often related to a stone in the gallbladder | |
| Specialty | Gastroenterology |
Gallstone formation occurs from the precipitation of crystals that aggregate to form stones. The most common form is cholesterol gallstones.[4] Other forms include calcium, bilirubin, pigment, and mixed gallstones.[4] Other conditions that produce similar symptoms include appendicitis, stomach ulcers, pancreatitis, and gastroesophageal reflux disease.[1]
Treatment for gallbladder attacks is typically surgery to remove the gallbladder.[1] This can be either done through small incisions or through a single larger incision.[1] Open surgery through a larger incision is associated with more complications than surgery through small incisions.[5] Surgery is typically done under general anesthesia.[1] In those who are unable to have surgery, medication to try to dissolve the stones or shock wave lithotripsy may be tried.[1] As of 2017, it is not clear whether surgery is indicated for everyone with biliary colic.[5]
In the developed world, 10 to 15% of adults have gallstones.[3] Of those with gallstones, biliary colic occurs in 1 to 4% each year.[3] Nearly 30% of people have further problems related to gallstones in the year following an attack.[3] About 15% of people with biliary colic eventually develop inflammation of the gallbladder if not treated.[3] Other complications include inflammation of the pancreas.[3]
Signs and symptoms
Pain is the most common presenting symptom. It is usually described as sharp, crampy, dull or severe right upper quadrant pain, which may radiate to the right shoulder, or less commonly, behind the breastbone.[6] Nausea and vomiting can be associated with biliary colic. Individuals may also present with pain that is induced following a fatty meal and the symptom of indigestion. The pain often lasts longer than 30 minutes, up to a few hours.[6] Patients usually have normal vital signs with biliary colic, whereas patients with cholecystitis are usually febrile and more ill appearing. Lab studies that should be ordered include a complete blood count, liver function tests and lipase. In biliary colic, lab findings are usually within normal limits. Alanine aminotransferase and aspartate transaminase are usually suggestive of liver disease whereas elevation of bilirubin and alkaline phosphatase suggests common bile duct obstruction.[7] Pancreatitis should be considered if the lipase value is elevated; gallstone disease is the major cause of pancreatitis.
Complications
The presence of gallstones can lead to inflammation of the gallbladder (cholecystitis) or the biliary tree (cholangitis) or acute inflammation of the pancreas (pancreatitis). Rarely, a gallstone can become impacted in the ileocecal valve that joins the caecum and the ileum, causing gallstone ileus (mechanical ileus).[6]
Complications from delayed surgery include pancreatitis, empyema, and perforation of the gallbladder, cholecystitis, cholangitis, and obstructive jaundice.[8]
Biliary pain in the absence of gallstones, known as postcholecystectomy syndrome, may severely affect the patient's quality of life, even in the absence of disease progression.[9]
Causes
Biliary pain is most frequently caused by obstruction of the common bile duct or the cystic duct by a gallstone. However, the presence of gallstones is a frequent incidental finding and does not always necessitate treatment, in the absence of identifiable disease. Furthermore, biliary pain may be associated with functional disorders of the biliary tract, so-called acalculous biliary pain (pain without stones), and can even be found in patients post-cholecystectomy (removal of the gallbladder), possibly as a consequence of dysfunction of the biliary tree and the sphincter of Oddi. Acute episodes of biliary pain may be induced or exacerbated by certain foods, most commonly those high in fat.[10]
Risk factors
Cholesterol gallstone formation risk factors include age, female sex, family history, race,[6][11] pregnancy, parity, obesity, hormonal birth control, diabetes mellitus, cirrhosis, prolonged fasting, rapid weight loss, total parenteral nutrition, ileal disease and impaired gallbladder emptying.[12]
Patients that have gallstones and biliary colic are at increased risk for complications, including cholecystitis.[13] Complications from gallstone disease is 0.3% per year and therefore prophylactic cholecystectomy are rarely indicated unless part of a special population that includes porcelain gallbladder, individuals eligible for organ transplant, diabetics and those with sickle cell anemia.[6]
Diagnosis
Diagnosis is guided by the person's presenting symptoms and laboratory findings. The gold standard imaging modality for the presence of gallstones is ultrasound of the right upper quadrant. There are many reasons for this choice, including no exposure to radiation, low cost, and availability in city, urban, and rural hospitals. Gallstones are detected with a specificity and sensitivity of greater than 95% with ultrasound.[14] Further signs on ultrasound may suggest cholecystitis or choledocholithiasis.[8] Computed Tomography (CT) is not indicated when investigating for gallbladder disease as 60% of stones are not radiopaque.[8] CT should only be utilized if other intra-abdominal pathology exists or the diagnosis is uncertain.[15] Endoscopic retrograde cholangiopancreatography (ERCP) should be used only if lab tests suggest the existence of a gallstone in the bile duct.[8] ERCP is then both diagnostic and therapeutic.
Management
Medications
Initial management includes the relief of symptoms and correcting electrolyte and fluid imbalance that may occur with vomiting.[7] Antiemetics, such as dimenhydrinate, are used to treat the nausea.[7] Pain may be treated with anti-inflammatories, NSAIDs such as ketorolac or diclofenac.[16] Opioids, such as morphine, less commonly may be used.[17] NSAIDs are more or less equivalent to opioids.[18] Hyoscine butylbromide, an antispasmodic, is also indicated in biliary colic.[19]
In biliary colic, the risk of infection is minimal and therefore antibiotics are not required.[20] Presence of infection indicates cholecystitis.[20]
Surgery
It is unclear whether those experiencing a gallstone attack should receive surgical treatment or not.[5] The scientific basis to assess whether surgery outperformed other treatment was insufficient and better studies were needed as of a SBU report in 2017.[5] Treatment of biliary colic is dictated by the underlying cause.[21] The presence of gallstones, usually visualized by ultrasound, generally necessitates a surgical treatment (removal of the gall bladder, typically via laparoscopy). [21] Removal of the gallbladder with surgery, known as a cholecystectomy, is the definitive surgical treatment for biliary colic. [22] A 2013 Cochrane review found tentative evidence to suggest that early gallbladder removal may be better than delayed removal.[23] Early laparoscopic cholecystectomy happens within 72 hours of diagnosis.[8] In a Cochrane review that evaluated receiving early versus delayed surgery, they found that 23% of those who waited on average 4 months ended up in hospital for complications, compared to none with early intervention with surgery.[8][23] Early intervention has other advantages including a reduced number of visits to the emergency department, fewer conversions to open surgery, less operating time required, and reduced time in hospital postoperatively.[8] The Swedish agency SBU estimated in 2017 that increasing acute phase surgeries could free multiple in-hospital days per patient and would additionally spare pain and suffering in wait of receiving an operation.[5] The report found that those with acute inflammation of the gallbladder can be surgically treated in the acute phase, within a few days of symptom debut, without increasing the risk for complications (compared to when the surgery is done later in an asymptomatic stage).[5]
References
- "Gallstones". NIDDK.NIH.gov. Washington DC: National Institute of Diabetes and Digestive and Kidney Diseases. November 2013. Archived from the original on 16 August 2016. Retrieved 27 July 2016.
- Internal Clinical Guidelines Team (October 2014). "Gallstone Disease: Diagnosis and Management of Cholelithiasis, Cholecystitis and Choledocholithiasis". NICE.org: 21. PMID 25473723. Clinical Guideline 188. Retrieved 24 June 2018.
- Ansaloni, L. (2016). "2016 WSES guidelines on acute calculous cholecystitis". World Journal of Emergency Surgery. 11: 25. doi:10.1186/s13017-016-0082-5. PMC 4908702. PMID 27307785.
- Sabiston, David C.; Townsend, Courtney M. (2012). Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. Philadelphia: Elsevier/Saunders. pp. 328–358. ISBN 978-1-4377-1560-6.
- "Surgery to treat gallstones and acute inflammation of the gallbladder". SBU.se. Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU). 2016-12-16. Retrieved 2017-06-01.
- Portincasa, P.; Moschetta, A.; Petruzzelli, M.; Palasciano, G.; Di Ciaula, A.; Pezzolla, A. (2006). "Gallstone disease: Symptoms and diagnosis of gallbladder stones". Best Practice & Research: Clinical Gastroenterology. 20 (6): 1017–1029. doi:10.1016/j.bpg.2006.05.005. PMID 17127185.
- Rosen, Peter; Marx, John A. (2013). Rosen's Emergency Medicine: Concepts and Clinical Practice. Philadelphia: Elsevier/Saunders. pp. 1186–1206. ISBN 978-1-4557-0605-1.
- Duncan, C. B.; Riall, T. S. (Nov 2012). "Evidence-based current surgical practice: calculous gallbladder disease". Journal of Gastrointestinal Surgery. 16 (11): 2011–2025. doi:10.1007/s11605-012-2024-1. PMC 3496004. PMID 22986769.
- Postcholecystectomy Syndrome at eMedicine
- Rodriguez, Diana. "When Gallbladder Problems Lead to Biliary Colic". Everyday Health.
- Stinton, Laura M.; Shaffer, Eldon A. (15 April 2012). "Epidemiology of Gallbladder Disease: Cholelithiasis and Cancer". Gut and Liver. 6 (2): 172–187. doi:10.5009/gnl.2012.6.2.172. PMC 3343155. PMID 22570746.
- Walton, Thomas J.; Lobo, Dileep N. (2009). "Gallstones". Surgery. 27 (1): 19–24. doi:10.1016/j.mpsur.2008.12.001.
- Afdhal, Nezam H. (2011). Goldman's Cecil Medicine (24th ed.). Philadelphia: Elsevier/Saunders. pp. 1011–1020. ISBN 978-1-4377-1604-7.
- Fischer, J. E., ed. (2007). Master of Surgery (5th ed.). Philadelphia: Lippincott Williams & Wilkins.
- Shakespear, J. S.; Shaaban, A. M.; Rezvani, M. (2010). "CT findings of acute cholecystitis and its complications". American Journal of Roentgenology. 194 (6): 1523–1529. doi:10.2214/ajr.09.3640. PMID 20489092.
- Fraquelli, M.; Casazza, G.; Conte, D.; Colli, A. (9 September 2016). "Non-steroid anti-inflammatory drugs for biliary colic". The Cochrane Database of Systematic Reviews. 2016 (9): CD006390. doi:10.1002/14651858.CD006390.pub2. PMC 6457716. PMID 27610712.
- Rosen, Peter; Marx, John A. (2013). Rosen's Emergency Medicine: Concepts and Clinical Practice. Philadelphia: Elsevier/Saunders. pp. 223–233. ISBN 978-1-4557-0605-1.
- Colli, A.; Conte, D.; Valle, S. D.; Sciola, V.; Fraquelli, M. (June 2012). "Meta-analysis: nonsteroidal anti-inflammatory drugs in biliary colic". Alimentary Pharmacology & Therapeutics. 35 (12): 1370–1378. doi:10.1111/j.1365-2036.2012.05115.x. PMID 22540869.
- "Hyoscine butylbromide (Buscopan) injection: Risk of serious adverse effects in patients with underlying cardiac disease". Gov.uk. Retrieved 23 September 2017.
- Cecil, Russell L. (Russell La Fayette); Goldman, Lee; Schafer, Andrew I. (2012). Goldman's Cecil Medicine. Philadelphia: Elsevier/Saunders. pp. 1011–1021. ISBN 978-1-4377-1604-7.
- Sigmon S, Dayal N, Meseeha M (2021). "Biliary Colic". National Center for Biotechnology Information, U.S. National Library of Medicine. PMID 28613523. Retrieved 8 July 2021.
- "Cholecystectomy: Approaches and Technique". The Lecturio Medical Concept Library. Retrieved 8 July 2021.
- Gurusamy, K. S.; Koti, R.; Fusai, G.; Davidson, B. R. (2013). "Early versus delayed laparoscopic cholecystectomy for uncomplicated biliary colic". Cochrane Database Syst Rev. 6 (6): CD007196. doi:10.1002/14651858.CD007196.pub3. PMID 23813478.