Blood in stool
Blood in stool looks different depending on how early it enters the digestive tract—and thus how much digestive action it has been exposed to—and how much there is. The term can refer either to melena, with a black appearance, typically originating from upper gastrointestinal bleeding; or to hematochezia, with a red color, typically originating from lower gastrointestinal bleeding.[6] Evaluation of the blood found in stool depends on its characteristics, in terms of color, quantity and other features, which can point to its source, however, more serious conditions can present with a mixed picture, or with the form of bleeding that is found in another section of the tract.[6][4] The term "blood in stool" is usually only used to describe visible blood, and not fecal occult blood, which is found only after physical examination and chemical laboratory testing.
| Blood in stool | |
|---|---|
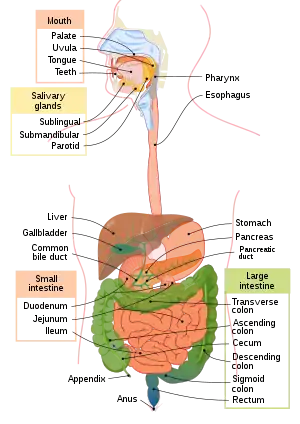 | |
| The transition from the upper to lower GI tract is considered to occur at the duodenal-jejunal junction,[1] therefore small intestine is part of both the upper and lower GI tract. Other organs participate in digestion including the liver, gallbladder, and pancreas.[2] Blood entering the upper GI tract travels further, therefore has more exposure to the GI system and can be partially digested into melena before leaving the system.[3] Hematochezia generally occurs lower in the GI tract, and is much closer to its exit, although fast bleeds can occur in the upper system as well.[3] Bleeding of the lower GI tract will typically appear as hematochezia and can vary in degree of seriousness.[4] Slow bleeding from the ascending portion of the colon can result in partial digestion of the blood and the appearance of melena in the stool.[5] | |
| Specialty | Gastroenterology |
| Types | Hematochezia, melena |
In infants, the Apt test can be used to distinguish fetal hemoglobin from maternal blood based on the differences in composition of fetal hemoglobin as compared to the hemoglobin found in adults.[7][8]
Differential diagnoses
Blood in the stool can come from many sources. The causes range from not harmful to very serious conditions. A common way to divide causes of bleeding is based on the source of bleeding. The GI tract can be divided into upper and lower, with some causes of bleeding affecting the entire tract (upper and lower).[9][10] Blood in the stool often appears different depending on its source. These differences can help when diagnosing these conditions. The rate of bleeding can also make blood in the stool look different from typical cases.[4][5]
Upper GI tract
The upper GI tract is defined as the organs involved in digestion above the ligament of Treitz and comprises the esophagus, stomach, and duodenum.[9] Upper gastrointestinal bleeding is typically characterized by melena (black stool). Bright red blood may be seen with active, rapid bleeding.[11]
Pathophysiology
The development of blood in a person's stool results from a variety of conditions, which can be divided into major categories of disease. These broad categories include cancerous processes or abnormal structure of bowel wall, inflammatory disease, colitis caused by infection or medications and vascular compromise.[5]
Motility
The gut wall is important for the movement of waste products through the GI tract. Repetitive attempts to have a bowel movement can lead to tearing around the exit of the rectum (anal fissure)
Structural
This list of diagnoses include diseases in which the wall of the bowel is compromised by disease.[5]
- Peptic ulcer disease[21][11][22][23]—divided into either duodenal or gastric ulcers, most common causes include:
- Non steroidal anti-inflammatory drug (NSAID)—the use of these medications results in a structural change in the wall of the gut, namely ulcers, and potential blood in the stool.[24]
- H. pylori infection—this bacterial infection can erode the wall of the stomach or duodenum, leading to a structural change in the stomach wall and bleeding in the stool.[23][25]
- Chronic disease[23]
- Diverticulitis[26] and diverticulosis[27] result from an out pouching of the colonic mucosa, or gut wall, leading to a break down of weak gut wall and an increased susceptibility to infection due to the bacteria in the GI tract, thus the potential for vascular compromise, the collection of bacteria in the area of perforation (abscess), the abnormal formation of communication between another part of the hollow GI tract (fistula), or blockage of the bowel (obstruction).[26]
- Meckel's diverticulum is a congenital remnant of the omphalo-mesenteric duct that connected the fetal yolk sac to the intestines which is normal closed off and destroyed during the process of development.[28] If a portion, or all of this duct remains a diverticulum or fistula can result, leading to the potential for a source of bleeding.[28]
Inflammatory bowel
Diseases causing inflammation in the GI tract can lead to blood in the stool.[29] Inflammation can occur anywhere along the GI tract in Crohn's disease,[30] or in the colon if a person has ulcerative colitis.[31]
Colitis
- Enteritis—inflammation of the small intestine, which has many causes including autoimmune conditions (e.g. Crohn's disease), certain drugs (e.g. ibuprofen), radiation therapy, and Coeliac disease.[36]
Infectious colitis
- Food poisoning—the bacteria that is associated with bloody diarrhea is typically E. coli
- Campylobacter enteritis[37]
- Shigellosis[38]
- Salmonellosis (Salmonella enteritis/Salmonella enterocolitis)[39][40]
- Bacterial gastroenteritis[41]
- Campylobacter jejuni
- Clostridium difficile
- Escherichia coli enteritis—most common cause of travelers' diarrhea[42]
- Salmonella enterica
- Shigella dysenteriae[38] see also dysentery
- Staphylococcus aureus[36]
Drug-induced colitis
Vascular compromise
- Angiodysplasia of the GI tract
- Arteriovenous malformation
- Anal fissure
- Esophageal varices[44]
- Hemorrhoids[45][46]
- Internal hemorrhoids are covered by a layer of mucosa and epithelium, making them more likely to bleed, but typically do not cause pain.[5]
- External hemorrhoids are less likely to bleed, they are covered by a different type of epithelium (squamous) but can cause significant pain as a result of thrombosis of the blood vessels within them.[5]
- Polypectomy during a colonoscopy can lead to a small amount of bleeding seen in the stool after the procedure
Other causes
- Blood in the diet, for example, the traditional diet of the Masai includes much blood drawn from cattle.
Diagnosis
The tests that are considered to evaluate of the passage of blood in the stool are based on the characteristics of bleeding (color, quantity) and whether or not the person passing blood has a low blood pressure with elevated heart rate, as opposed to normal vital signs.[4] The following tests are combined to determine the causes of the source of bleeding.
- Digital rectal exam (DRE) and fecal occult blood test (FOBT)
- Colonoscopy
- Anoscopy
- Esophagogastroduodenoscopy (EGD)
- Capsule endoscopy
- CT Scan
Melena is defined as dark, tarry stools, often black in color due to partial digestion of the RBCs.[6]
Hematochezia is defined as bright red blood seen in the toilet either inside of, or surrounding the stool.[6]
Hematochezia is typically presumed to come from the lower portion of the GI tract, and the initial steps of diagnosis include a DRE with FOBT, which if positive, will lead to a colonoscopy.[6][47][48][4] If the person has a large amount of blood in their stool, an EGD test may be necessary.[6][4][47][48] If no source of active bleeding is found on these examinations, a capsule endoscopy may be performed, in order to more closely examine the small bowel, which cannot be seen with the other types of studies.[48] With melena, a DRE with FOBT is often also performed, however the suspicion for a source from the upper GI tract is higher, leading first to the use of EGD with the other tests being required if no source is identified.[47][48] The anoscopy is another type of examination, which can be used along with a colonoscopy, which exams the rectum and distal portion of the descending colon.[6][4]
| Color | Medical term | Frequency | Quantity | Examples of types of bleeding considered |
|---|---|---|---|---|
| Bright red | Hematochezia[6] | Occasional occurrence of blood | Small | Hemorrhoids, inflammatory conditions, polyps[4] |
| Bright red | Hematochezia[6] | Increased stooling, blood with every stool | Large | Rapid bleeding, e.g. ulcer, varices[4][47] |
| Dark red/black | Melena[6] | Blood with every stool | Difficult to measure, mixed in with stool | Slow bleeding, cancer, ulcer, (peptobismol and iron use can be mimics)[47] |
Other features
Mucus may also be found in stool.[4]
A texture described as tarry stool is generally associated with dark black stool seen in partially digested blood.[6] This is generally associated with melena.
Patient age
A person's age is an important consideration when assessing the cause of the bleeding.[4]
| Age | Group | Types of bleeding considered |
|---|---|---|
| <20 years | Pediatric | Inherited/autoimmune condition or structural |
| 20–60 years | Middle aged | Inherited/autoimmune condition, vascular malformation |
| >60 years | Elderly | Vascular malformation, liver disease, cancer |
Treatment
Treatment of bloody stool depends largely on the cause of the bleeding. Bleeding is commonly associated with symptoms of fatigue, dizziness, headaches, or even shortness of breath, and these associated symptoms also require treatment.[49][50] These symptoms are the result of blood loss, and occur due to a lack of red blood cells (RBCs) circulating in the vascular system, resulting in less oxygen reaching the tissues and organs.[51][50] Blood in stool can be associated with serious complications as a result of blood volume loss (hemorrhage) or a slow leak of the blood leading to low levels of hemoglobin in the circulating blood (anemia).[51]
Anemia
Anemia is a common complication of blood in the stool, especially when there is a large amount of blood or bleeding occurs over a long period of time.[51] Anemia is also commonly associated with an iron deficiency, due to the importance of iron in the formation of red blood cells (RBCs).[50] When anemia is diagnosed as a result of blood in the stool, vitamins that are important for RBC formation (folate, vitamin B12, and vitamin C) are frequently prescribed in order to ensure that all the materials are available for those cells that are made.[50]
Specific treatment
Diagnostic measures can be used as interventions to help stop bleeding in some cases. Bleeding that occurs due to a neoplasm (cancer growth) can be treated using colonoscopy and clipping, surgical intervention, or other measures, depending on the form and stage of cancer.[52] Similarly, gastric cancer is treated depending on the staging, although typically requires surgical and medical therapy.[53]
The treatment for motility issues, namely constipation, is typically to improve the movement of waste through the GI tract. This is done by using stool softeners (which work by pulling water into the stool while in the colon), addition of fiber to the diet, and use of osmotic laxatives (which help fluid movement through the colon, improving overall motility). Improving a persons gut motility can reduce the straining during defection and decrease the risk of developing of anal fissures.[54] Anal fissures are associated with pain and blood on the toilet paper, and require time for healing.[55] Treatment includes topical nitrates or calcium channel blockers and surgical interventions for chronic or complex cases.[55] Similar to anal fissures, internal hemorrhoids can cause blood on the tissue when wiping, and be felt at the opening of the anus. Treatment options for hemorrhoids can be dependent on whether an underlying cause exists. An anorectal varices related hemorrhoids caused by cirrhosis, however symptomatic treatment often involves removal.[45]
Colitis can be divided into infectious and drug induced, as can the treatment for these conditions. With infectious colitis, treatment is pathogen dependent, and generally requires the use of antibiotics. With drug-induced colitis, treatment typically involves removal of the offending agent, as is the case in NSAID induced PUD,[24] however, removing radiation from a cancer patient is not always practical within a treatment regimen, so medical treatment is the primary mode of treatment.[56]
Structural compromise leading to blood in stool is caused by a variety of conditions, and therefore requires different treatment for each condition. Peptic ulcer disease alone can be divided into multiple causes, but is generally initially controlled primarily with a proton pump inhibitor, with the addition of an H2 blocker, or in serious cases, requiring surgical intervention.[11] Diverticulitis and diverticulosis require antibiotic treatment, and may require surgical intervention.[26]
Inflammatory bowel disease is also divided into separate conditions, namely ulcerative colitis and Crohn's disease, which have different medical treatment regimens, and may require surgical intervention in more serious conditions.[30]
See also
References
- pmhdev. "Lower Gastrointestinal Tract - National Library of Medicine". PubMed Health. Retrieved 2017-12-02.
- pmhdev. "Gastrointestinal Tract - National Library of Medicine". PubMed Health. Retrieved 2017-12-02.
- Wilson, I. Dodd (1990). Walker, H. Kenneth; Hall, W. Dallas; Hurst, J. Willis (eds.). Clinical Methods: The History, Physical, and Laboratory Examinations (3rd ed.). Boston: Butterworths. ISBN 978-0409900774. PMID 21250251.
- Cotter, Thomas G.; Buckley, Niamh S.; Loftus, Conor G. (2017). "Approach to the Patient With Hematochezia". Mayo Clinic Proceedings. 92 (5): 797–804. doi:10.1016/j.mayocp.2016.12.021. PMID 28473039.
- Kasper D, Fauci A, Hauser S, Longo D, Jameson J, Loscalzo J. eds. (Part 14: The Gastrointestinal System, Chs 344,345,348,351,353,365)'Harrison's Principles of Internal Medicine, 19e New York, NY: McGraw-Hill; 2014.
- Wilson, Dodd (1990). "85". In Walker, H. Kenneth; Hall, W. Dallas; Hurst, J. Willis (eds.). Clinical Methods: The History, Physical, and Laboratory Examinations. Boston: Butterworths. ISBN 9780409900774.
- "Hemoglobin F". phpa.health.maryland.gov. Retrieved 2017-12-06.
- "Apt-Downey test". www.allinahealth.org. Mar 29, 2016. Retrieved 2017-12-06.
- pmhdev. "Upper Gastrointestinal Tract - National Library of Medicine". PubMed Health. Retrieved 2017-11-25.
- pmhdev. "Lower Gastrointestinal Tract - National Library of Medicine". PubMed Health. Retrieved 2017-11-25.
- MD, Scott Moses. "Upper Gastrointestinal Bleeding". www.fpnotebook.com. Retrieved 2017-11-26.
- "What are Colon Cancer Symptoms". Coloncancer.about.com. 2009-01-20. Retrieved 2012-01-31.
- "Colon cancer: Symptoms". MayoClinic.com. 2011-08-13. Retrieved 2012-01-31.
- Lenz, Heinz-Josef (2009-03-06). "What are Early Symptoms of Colorectal Cancer? Watch out for Small Changes". Alexandria, Virginia: Fight Colorectal Cancer. Archived from the original on 2009-03-10. Retrieved 2013-02-23.
- "Colon Cancer Symptoms - Colorectal Cancer Symptoms". Webmd.com. 2010-10-31. Retrieved 2012-01-31.
- "Crohn's Disease: Inflammatory Bowel Diseases (IBD): Merck Manual Home Edition". Merckmanuals.com. Retrieved 2012-01-31.
- Gastric Cancer at eMedicine
- Chatoor D, Emmnauel A (2009). "Constipation and evacuation disorders". Best Pract Res Clin Gastroenterol. 23 (4): 517–30. doi:10.1016/j.bpg.2009.05.001. PMID 19647687.
- American Gastroenterological Association; Bharucha, AE; Dorn, SD; Lembo, A; Pressman, A (January 2013). "American Gastroenterological Association medical position statement on constipation". Gastroenterology (Review). 144 (1): 211–17. doi:10.1053/j.gastro.2012.10.029. PMID 23261064.
- "Complications". nhs.uk. 2017-10-20. Retrieved 2017-12-06.
- MD, Scott Moses (Nov 5, 2017). "Gastrointestinal Bleeding". www.fpnotebook.com. Retrieved 2017-11-26.
- "Peptic ulcer: Symptoms". MayoClinic.com. 2011-01-06. Retrieved 2012-01-31.
- MD, Scott Moses (Nov 5, 2017). "Peptic Ulcer Disease". www.fpnotebook.com.
- Wallace, J. L. (February 2000). "How do NSAIDs cause ulcer disease?". Baillière's Best Practice & Research. Clinical Gastroenterology. 14 (1): 147–159. doi:10.1053/bega.1999.0065. PMID 10749095.
- Testerman, Traci L; Morris, James (2014-09-28). "Beyond the stomach: An updated view of Helicobacter pylori pathogenesis, diagnosis, and treatment". World Journal of Gastroenterology. 20 (36): 12781–12808. doi:10.3748/wjg.v20.i36.12781. ISSN 1007-9327. PMC 4177463. PMID 25278678.
- Linzay, Catherine D.; Pandit, Sudha (2017). "Acute Diverticulitis". StatPearls. Treasure Island (FL): StatPearls Publishing. PMID 29083630.
- "Diverticulitis: Diverticular Disease: Merck Manual Home Edition". Merckmanuals.com. Retrieved 2012-01-31.
- Sagar, Jayesh; Kumar, Vikas; Shah, D K (Oct 2006). "Meckel's diverticulum: a systematic review". Journal of the Royal Society of Medicine. 99 (10): 501–505. doi:10.1177/014107680609901011. ISSN 0141-0768. PMC 1592061. PMID 17021300.
- "Learn the Facts About Crohn's Disease". Crohn's and Colitis. Retrieved 2017-12-06.
- "What is Crohn's Disease | Causes of Crohn's | Crohn's & Colitis Foundation". www.crohnscolitisfoundation.org. Retrieved 2017-12-06.
- "Ulcerative Colitis". NIDDK. September 2014. Retrieved Dec 6, 2017.
- "Crohn's disease: Symptoms". MayoClinic.com. 2011-08-09. Retrieved 2012-01-31.
- Travis SP, Higgins PD, Orchard T, Van Der Woude CJ, Panaccione R, Bitton A, O'Morain C, Panés J, Sturm A, Reinisch W, Kamm MA, D'Haens G (July 2011). "Review article: defining remission in ulcerative colitis" (PDF). Aliment Pharmacol Ther (Review). 34 (2): 113–24. doi:10.1111/j.1365-2036.2011.04701.x. hdl:2027.42/87130. PMID 21615435. S2CID 139549.
- Walmsley, R.S.; Ayres, R.C.S.; Pounder, R.E.; Allan, R N (1998). "A simple clinical colitis activity index". Gut. 43 (1): 29–32. doi:10.1136/gut.43.1.29. ISSN 0017-5749. PMC 1727189. PMID 9771402.
- Walmsley, R S; Ayres, R.C.S.; Pounder, R E; Allan, R.N. (1998). "A simple clinical colitis activity index: Table One". Gut. 43 (1): 29–32. doi:10.1136/gut.43.1.29. ISSN 0017-5749. PMC 1727189. PMID 9771402.
- MedlinePlus Encyclopedia: Enteritis
- MedlinePlus Encyclopedia: Campylobacter infection
- Shigellosis, National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention
- MedlinePlus Encyclopedia: Salmonella enterocolitis
- "Salmonella infection: Symptoms". MayoClinic.com. 2011-04-16. Retrieved 2012-01-31.
- MedlinePlus Encyclopedia: Bacterial gastroenteritis
- MedlinePlus Encyclopedia: E. coli enteritis
- MedlinePlus Encyclopedia: Radiation enteritis
- "Esophageal varices: Symptoms". MayoClinic.com. 2010-10-30. Retrieved 2012-01-31.
- Hemorrhoids Archived 2014-03-11 at the Wayback Machine, National Digestive Diseases Information Clearinghouse, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health.
- Hemorrhoids: Symptoms, Mayo Clinic.
- MD, Scott Moses,. "Upper Gastrointestinal Bleeding". www.fpnotebook.com. Retrieved 2017-11-26.
- Kasper D, Fauci A, Hauser S, Longo D, Jameson J, Loscalzo J. eds. 'Harrison's Principles of Internal Medicine, 19e New York, NY: McGraw-Hill; 2014.
- pmhdev. "Anemia - National Library of Medicine". PubMed Health. Retrieved 2017-12-09.
- "Anemia - Symptoms and causes - Mayo Clinic". www.mayoclinic.org. Retrieved 2017-12-09.
- "Anemia | Symptoms and Conditions | MUSC DDC". ddc.musc.edu. Retrieved 2017-12-07.
- "Treatment of Colon Cancer, by Stage". www.cancer.org. Retrieved 2017-12-09.
- "Treatment Choices by Type and Stage of Stomach Cancer". www.cancer.org. Retrieved 2017-12-09.
- "Constipation - Diagnosis and treatment - Mayo Clinic". www.mayoclinic.org. Retrieved 2017-12-09.
- McCallion, K.; Gardiner, K. R. (2001-12-01). "Progress in the understanding and treatment of chronic anal fissure". Postgraduate Medical Journal. 77 (914): 753–758. doi:10.1136/pmj.77.914.753. ISSN 0032-5473. PMC 1742193. PMID 11723312.
- Stacey, Rhodri; Green, John T. (Jan 2014). "Radiation-induced small bowel disease: latest developments and clinical guidance". Therapeutic Advances in Chronic Disease. 5 (1): 15–29. doi:10.1177/2040622313510730. ISSN 2040-6223. PMC 3871275. PMID 24381725.