Diverticulosis
Diverticulosis is the condition of having multiple pouches (diverticula) in the colon that are not inflamed. These are outpockets of the colonic mucosa and submucosa through weaknesses of muscle layers in the colon wall.[1] Diverticula do not cause symptoms in most people.[2] Diverticular disease occurs when diverticula become clinically inflamed, a condition known as diverticulitis.[3]
| Diverticulosis | |
|---|---|
| Other names | Diverticular disease of the colon |
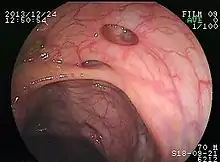
_01.svg.png.webp) | |
| Diverticulosis as seen endoscopically | |
| Specialty | General surgery |
Diverticula typically occur in the sigmoid colon, which is commonplace for increased pressure. The left side of the colon is more commonly affected in the United States while the right side is more commonly affected in Asia.[4] Diagnosis is often during routine colonoscopy or as an incidental finding during CT scan.[2]
It is common in Western countries with about half of those over the age of 60 affected in Canada and the United States.[4] Diverticula are uncommon before the age of 40, and increase in incidence beyond that age.[5] Rates are lower in Africa;[4] the reasons for this remain unclear but may involve the greater prevalence of a high fiber diet in contrast with the lower-fiber diet characteristic of many Western populations.[6]
Signs and symptoms
Some people with diverticulosis complain of symptoms such as cramping, bloating, flatulence, and irregular defecation. However, it is unclear if these symptoms are attributable to the underlying diverticulosis or to coexistent irritable bowel syndrome.[7]
Diverticular disease was found associated with a higher risk of left sided colon cancer.[8]
Bleeding
Diverticular disease can present with painless rectal bleeding as bright red blood per rectum. Diverticular bleeding is the most common cause of acute lower gastrointestinal bleeding.[9] However, it is estimated that 80% of these cases are self-limiting and require no specific therapy.[10]
Diverticulitis
Infection of a diverticulum can result in diverticulitis. A recent study[11] found that it happens only about 4% of the time. That contradicts the prevailing thinking that 10% to 25% of people with diverticulosis go on to develop diverticulitis. Tears in the colon leading to bleeding or perforations may occur; intestinal obstruction may occur (constipation or diarrhea does not rule this possibility out); and peritonitis, abscess formation, retroperitoneal fibrosis, sepsis, and fistula formation are also possible occurrences. Rarely, an enterolith may form. Infection of a diverticulum often occurs as a result of stool collecting in a diverticulum.
It is defined as diverticular disease with signs and symptoms of diverticular inflammation. Clinical features of acute diverticulitis include constant abdominal pain, localized abdominal tenderness in the left lower quadrant of the abdomen, nausea, vomiting, constipation or diarrhea, fever and leukocytosis.[12]
Most people with colonic diverticulosis are unaware of this structural change. When symptoms do appear in a person over 40 years of age it is important to obtain medical advice and exclude more dangerous conditions such as cancer of the colon or rectum.[13][14][15][16]
Segmental colitis associated with diverticulosis
Segmental colitis associated with diverticulosis (SCAD) is a condition characterized by localized inflammation of the colon between diverticula (interdiverticular mucosa) while sparing the diverticular orifices. SCAD may lead to abdominal pain, especially in the left lower quadrant, intermittent rectal bleeding, and chronic diarrhea.
Causes
Diet
The U.S. National Institutes of Health notes that, although the low-fiber theory of the cause of diverticulosis is the leading theory, it has not yet been proven.[17]
Genetics
The predisposition to diverticulosis for specific individuals is likely explained by a genetic component, a theory that is supported by studies examining the rates of diverticulosis among twins.[1] The heritability of diverticulosis is estimated to be approximately 40%.[1]
Intestinal motility
Another theory suggests the degeneration of glial neurons in the myenteric plexus and the interstitial cells of Cajal lead to slowed intestinal movement and consequently fecal content exerts increased pressure on the colon wall resulting in the formation of diverticula.[1]
Risk factors
- Advanced age
- constipation
- a diet that is low in dietary fiber (although this claim is controversial)
- connective tissue disorders (such as Marfan syndrome and Ehlers Danlos Syndrome) that may cause weakness in the colon wall
- hereditary or genetic predisposition,[18]
- extreme weight loss
- heavy meat consumption[19][20][21]
Pathophysiology
.jpg.webp)
The precise mechanisms by which diverticula are formed are unknown.[1] Multiple theories have been proposed including genetic susceptibility, diet, intestinal motility, changes in the microbiome, and inflammation. One leading theory suggests that diverticula form in weakened areas of the colon wall that are subjected to increased pressure.[1] The strength of the colon wall is known to decrease with age.[1] Previous theories proposed that impacted fecal matter and certain foods would get stuck in diverticula (thereby causing trauma), which caused poor blood flow, death of the affected intestinal wall cells, and intestinal perforation.[1] Newer theories have called this paradigm into question.[1]
Diagnosis



Diverticulosis is defined by the presence of multiple pouches (diverticula) in the colon.[22] In people without symptoms, these are usually found incidentally during other investigations.
While a good history is often sufficient to form a diagnosis of diverticulosis or diverticulitis, it is important to confirm the diagnosis and rule out other pathology (notably colorectal cancer) and complications.
Imaging
- Barium enema is inferior to colonoscopy in terms of image quality and is usually only performed if the patient has strictures or an excessively tortuous sigmoid colon where colonoscopy is difficult or dangerous.
- Colonoscopy will show the diverticulum and rule out malignancy. A colonoscopy should be performed 4–6 weeks after an acute episode.
- Contrast CT is the investigation of choice in acute episodes of diverticulitis and where complications exist.
- MRI provides a clear picture of the soft tissue of the abdomen, however, its expense often outweighs the benefits when compared to contrast CT or colonoscopy.
- Plain abdominal X-ray may show signs of a thickened wall, ileus, constipation, small bowel obstruction or free air in the case of perforation. Plain X-rays are insufficient to diagnose diverticular disease.
- There is no blood test for diverticulosis.
It is important to note that both barium enema and colonoscopy are contraindicated during acute episodes of diverticulitis, as the barium may leak out into the abdominal cavity, and colonoscopy can cause perforations of the bowel wall.
Management
Many people with diverticulosis have minimal to no symptoms and do not require any specific treatment. Colonic stimulants should be avoided. Treatments, like some colon cleansers, that cause hard stools, constipation, and straining, are not recommended.
Diet
A high-fiber diet and fiber supplements are advisable to prevent constipation.[23][24] The American Dietetic Association recommends 20–35 grams each day. Wheat bran has been shown to reduce intra colonic pressure.[25][26]
The US National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) says foods such as nuts, popcorn hulls, sunflower seeds, pumpkin seeds, caraway seeds, and sesame seeds have traditionally been labeled as problem foods for people with this condition; however, no scientific data exists to prove this hypothesis. The seeds in tomatoes, zucchini, cucumbers, strawberries, raspberries, and poppy seeds, are not considered harmful by the NIDDK.[2]
One study found that nuts and popcorn do not contribute positively or negatively to patients with diverticulosis or diverticular complications.[27][28]
Complications
Complicated diverticulosis requires treatment of the complication. These complications are often grouped under a single diagnosis of diverticulitis and require skilled medical care of the infection, bleeding and perforation which may include intensive antibiotic treatment, intravenous fluids, and surgery. Complications are more common in patients who are taking NSAIDs or aspirin. As diverticulosis occurs in an older population such complications are serious events.
Epidemiology
The prevalence of diverticulosis progressively increases with age. Approximately 50% of people over the age of 60 and 70% of people over the age of 80 have diverticulosis.[1] This disease is common in the U.S., Britain, Australia, Canada, and is uncommon in Asia and Africa.[5] Large-mouth diverticula are associated with scleroderma. Diverticular disease is more common in collagen disorders such as Ehlers Danlos Syndrome.[29]
History
The modern emphasis on the value of fiber in the diet began with Thomas L. Cleave.[30] A strong case was made by Neil Painter[31] and Adam Smith[32] that a deficiency of dietary fiber is the cause of diverticular disease. They argued that the colonic muscles needed to contract strongly in order to transmit and expel the small stool associated with a fiber deficient diet. The increased pressure within the segmented section of the bowel over years gave rise to herniation at the vulnerable point where blood vessels enter the colonic wall.
Society and culture
Economics
"The complications of diverticulosis cause considerable morbidity in the United States; health care expenditures for this disorder are estimated to be $2.5 billion per year."[33]
See also
- Salpingitis isthmica nodosa – diverticulosis of the Fallopian tube
References
- Feuerstein, JD; Falchuk, KR (August 2016). "Diverticulosis and Diverticulitis". Mayo Clinic Proceedings (Review). 91 (8): 1094–1104. doi:10.1016/j.mayocp.2016.03.012. PMID 27156370.
- "Diverticular Disease". www.niddk.nih.gov. September 2013. Retrieved 12 June 2016.
- Tursi A, Papa A, Danese S (September 2015). "Review article: the pathophysiology and medical management of diverticulosis and diverticular disease of the colon". Alimentary Pharmacology & Therapeutics. 42 (6): 664–84. doi:10.1111/apt.13322. PMID 26202723. S2CID 24568867.
- Tursi, A (March 2016). "Diverticulosis today: unfashionable and still under-researched". Therapeutic Advances in Gastroenterology. 9 (2): 213–28. doi:10.1177/1756283X15621228. PMC 4749857. PMID 26929783.
- Comparato G, Pilotto A, Franzè A, Franceschi M, Di Mario F (2007). "Diverticular disease in the elderly". Digestive Diseases. 25 (2): 151–9. doi:10.1159/000099480. PMID 17468551.
- Painter NS, Burkitt DP (May 1971). "Diverticular disease of the colon: a deficiency disease of Western civilization". British Medical Journal. 2 (5759): 450–4. doi:10.1136/bmj.2.5759.450. PMC 1796198. PMID 4930390.
- "Clinical manifestations and diagnosis of colonic diverticular disease". Literature review.
- Stefánsson T, Ekbom A, Sparèn P, Påhlman L (August 2004). "Association between sigmoid diverticulitis and left-sided colon cancer: a nested, population-based, case control study". Scand J Gastroenterol. 39 (8): 743–7. doi:10.1080/00365520410003272. PMID 15513359. S2CID 21100705.
- Acute lower gastrointestinal bleeding in 1,112 patients admitted to an urban emergency medical center. Gayer C1, Chino A, Lucas C, Tokioka S, Yamasaki T, Edelman DA, Sugawa C. http://www.surgjournal.com/article/S0039-6060(09)00481-4/pdf
- Barnert J, Messmann H (2008). "Management of lower gastrointestinal tract bleeding". Best Practice & Research. Clinical Gastroenterology. 22 (2): 295–312. doi:10.1016/j.bpg.2007.10.024. PMID 18346685.
- Peery, Anne F.; Sandler, Robert S. (2013). "Diverticular Disease: Reconsidering Conventional Wisdom". Clinical Gastroenterology and Hepatology. 11 (12): 1532–1537. doi:10.1016/j.cgh.2013.04.048. PMC 3785555. PMID 23669306.
- Tursi A, Papagrigoriadis S (September 2009). "Review article: the current and evolving treatment of colonic diverticular disease". Alimentary Pharmacology & Therapeutics. 30 (6): 532–46. doi:10.1111/j.1365-2036.2009.04072.x. PMID 19549266. S2CID 22765199.
- Shepherd NA (1992) Diverticular disease. In Oxford Textbook of Pathology, pp. 1256–1258 [J O'D McGee, PG Isaacson, and NA Wright, editors]. Oxford: Oxford University Press.
- Christensen J (1991) Gross and microscopic anatomy of the large intestine. In The Large Intestine Physiology, Pathophysiology and Disease, pp. 13-35 [SF Phillips, JH Pemberton and RG Shorter, editors]. New York: Raven Press.
- West, AB (2008). "The pathology of diverticulitis". J Clin Gastroenterol. 42 (10): 1137–8. doi:10.1097/MCG.0b013e3181862a9f. PMID 18936652.
- Drummond, H (1916). "Sacculi of the large intestine with special reference to their relation to the blood vessels of the bowel wall". British Journal of Surgery. 4 (15): 407–413. doi:10.1002/bjs.1800041505. S2CID 72222598.
- "Understanding Diverticulosis and Diverticulitis - NIH MedicinePlus". Nlm.nih.gov. 27 August 2012. Retrieved 4 October 2013.
- "Diverticulosis and Diverticulitis". American College of Gastroenterology.
- Humes D, Smith JK, Spiller RC (14 March 2011). "Colonic diverticular disease: medical treatments for acute diverticulitis". BMJ Clinical Evidence. 2011. PMC 3275154. PMID 21401970.
A prospective cohort study reported that consuming a vegetarian diet and a high intake of dietary fibre were associated with a lower risk of admission to hospital or death from diverticular disease. High meat intake is also a risk factor for developing diverticular disease.
- Grossi, Enzo; Pace, Fabio (12 May 2016). Human Nutrition from the Gastroenterologist's Perspective. Springer. p. 104. ISBN 9783319303611.
It has been hypothesized that the increased consumption of animal proteins increases the risk of diverticular disease by altering the metabolism of bacteria in the colon or increasing the intake of fat.
- DiMarino, Anthony J.; Benjamin, Stanley B. (2002). Gastrointestinal Disease: An Endoscopic Approach. SLACK Incorporated. p. 863. ISBN 9781556425110.
- Pemberton, John H (16 June 2016). "Colonic diverticulosis and diverticular disease: Epidemiology, risk factors, and pathogenesis". UpToDate. Retrieved 13 March 2017.
- Aldoori, WH; Giovannucci, EL; Rimm, EB; Wing, AL; et al. (1994). "A prospective study of diet and the risk of symptomatic diverticular disease in men". The American Journal of Clinical Nutrition. 60 (5): 757–64. doi:10.1093/ajcn/60.5.757. PMID 7942584.
- Gear, JS; Ware, A; Fursdon, P; Mann, JI; et al. (1979). "Symptomless diverticular disease and intake of dietary fibre". Lancet. 1 (8115): 511–4. doi:10.1016/S0140-6736(79)90942-5. PMID 85104. S2CID 37933413.
- Marlett, JA; McBurney, MI; Slavin, JL; American Dietetic, Association (2002). "Position of the American Dietetic Association: health implications of dietary fiber". Journal of the American Dietetic Association. 102 (7): 993–1000. doi:10.1016/S0002-8223(02)90228-2. PMID 12146567.
- Eglash, A; Lane, CH; Schneider, DM (2006). "Clinical inquiries. What is the most beneficial diet for patients with diverticulosis?". The Journal of Family Practice. 55 (9): 813–5. PMID 16948968.
- Strate, LL; Liu, YL; Syngal, S; Aldoori, WH; et al. (2008). "Nut, Corn, and Popcorn Consumption and the Incidence of Diverticular Disease". JAMA. 300 (8): 907–914. doi:10.1001/jama.300.8.907. PMC 2643269. PMID 18728264.
- "Eating Nuts, Popcorn Not Linked With Higher Risk of Diverticulosis". Newswise. 21 August 2008. Retrieved 26 August 2008.
- Hobson KG, Roberts PL (August 2004). "Etiology and pathophysiology of diverticular disease". Clinics in Colon and Rectal Surgery. 17 (3): 147–53. doi:10.1055/s-2004-832695. PMC 2780060. PMID 20011269.
- Cleave TL 1974 The Saccharine disease Wright Bristol
- Painter NS (1975) Diverticular disease of the colon. Heinemann Medical Books
- Smith, AN (1991). "Diverticular disease of the colon" in The Large Intestine. Ed. Phillips SF, Pemberton JH, and Shorter RG. Raven Press. pp. 549–578
- Peery, AF; Barrett, PR; Park, D; Rogers, AJ; et al. (February 2012). "A high-fiber diet does not protect against asymptomatic diverticulosis". Gastroenterology. 142 (2): 266–72.e1. doi:10.1053/j.gastro.2011.10.035. PMC 3724216. PMID 22062360.
External links
- Marlett JA, McBurney MI, Slavin JL (2002). "Position of the American Dietetic Association: health implications of dietary fiber". J Am Diet Assoc. 102 (7): 993–1000. doi:10.1016/S0002-8223(02)90228-2. PMID 12146567. Archived from the original on 3 December 2016. Retrieved 22 August 2008.