Hypochondroplasia
Hypochondroplasia (HCH) is a developmental disorder caused by an autosomal dominant genetic defect in the fibroblast growth factor receptor 3 gene (FGFR3) that results in a disproportionately short stature, micromelia[3] and a head that appears large in comparison with the underdeveloped portions of the body. It is classified as short-limbed dwarfism.[2][4]
| Hypochondroplasia | |
|---|---|
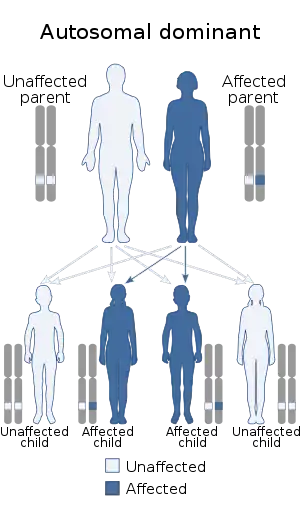 | |
| Hypochondroplasia is autosomal dominant in inheritance. | |
| Specialty | Medical genetics |
| Symptoms | Skeletal dysplasia[1] |
| Causes | FGFR3 gene mutation[2] |
| Diagnostic method | Physical finding, X-ray[3] |
| Treatment | Special education, Laminectomy [1] |
Signs and symptoms
Individuals affected by this disorder appear normal at birth. As the infant grows, however, their arms and legs do not develop properly, and their body becomes thicker and shorter than normal.[3] The following are characteristics consistent with this condition:[1]
- Brachydactyly
- Short stature
- Micromelia
- Skeletal dysplasia
- Abnormality of femur
Cause
Hypochondroplasia is transmitted as an autosomal dominant trait affecting the FGFR3 gene on chromosome 4p16.3. There is currently no cure for this condition.[2]
Pathophysiology

This disorder results from mutations in the proximal tyrosine kinase domain of the FGFR3 gene.[3] This gene plays an important role in embryonic development, playing a part in regulating activities such as cell division, migration and differentiation.
Hypochondroplasia can result from p. Lys650Asn as well.[5][3] In FGFR3, some 20 different mutations have been associated to hypochondroplasia,[6] and it seems to have a role in skeletal dysplasia.[7]
Diagnosis
The diagnosis of this condition can be done via X-rays (with lack of normal distance L1 to L5),[8] and additionally genetic testing is available to ascertain hypochondroplasia.[9] However, the physical characteristics are one of the most important in determining the condition.[3]
Treatment

Treatment of hypochondroplasia usually takes the form of orthopedic surgery and physical therapy. Genetic counseling is advised for individuals and their families. Specifically in the case of spinal stenosis, one option is laminectomy.[3][1]
Prognosis
Life expectancy for individuals with hypochondroplasia is normal; height is about 132–147 centimetres (4 ft 4 in – 4 ft 10 in).[10]
References
- "Hypochondroplasia | Genetic and Rare Diseases Information Center (GARD) – an NCATS Program". rarediseases.info.nih.gov. Retrieved 21 December 2016.
- "Hypochondroplasia - Genetics Home Reference". Retrieved 2009-03-12.
- Bober, Michael B.; Bellus, Gary A.; Nikkel, Sarah M.; Tiller, George E. (1 January 1993). "Hypochondroplasia". GeneReviews. PMID 20301650. Retrieved 18 December 2016.update 2013
- "Dwarfism: MedlinePlus". NIH. NIH. Retrieved 21 December 2016.
- "NM_000142.4(FGFR3):c.1950G>C (p.Lys650Asn) AND Hypochondroplasia - ClinVar - NCBI". www.ncbi.nlm.nih.gov. Retrieved 21 December 2016.
- Reference, Genetics Home. "FGFR3 gene". Genetics Home Reference. Retrieved 21 December 2016.
- Foldynova-Trantirkova, Silvie; Wilcox, William R.; Krejci, Pavel (21 December 2016). "Sixteen years and counting: the current understanding of fibroblast growth factor receptor 3 (FGFR3) signaling in skeletal dysplasias". Human Mutation. 33 (1): 29–41. doi:10.1002/humu.21636. ISSN 1059-7794. PMC 3240715. PMID 22045636.
- "OMIM Entry - # 146000 - HYPOCHONDROPLASIA; HCH". omim.org. Retrieved 21 December 2016.
- "Hypochondroplasia - Conditions - GTR - NCBI". www.ncbi.nlm.nih.gov. Retrieved 21 December 2016.
- RESERVED, INSERM US14 -- ALL RIGHTS. "Orphanet: Hypochondroplasia". www.orpha.net. Retrieved 21 December 2016.
Further reading
- ed, Sally Radovick; MacGillivray, Margaret H. (2010). Pediatric Endocrinology a Practical Clinical Guide, Second Edition (2nd ed.). Dordrecht: Springer. ISBN 9781607613954. Retrieved 21 December 2016.
- Kelly, Evelyn B. (2013). Encyclopedia of human genetics and disease. Santa Barbara, Calif.: Greenwood. ISBN 9780313387142. Retrieved 21 December 2016.