Hypokalemia
Hypokalemia is a low level of potassium (K+) in the blood serum.[1] Mild low potassium does not typically cause symptoms.[3] Symptoms may include feeling tired, leg cramps, weakness, and constipation.[1] Low potassium also increases the risk of an abnormal heart rhythm, which is often too slow and can cause cardiac arrest.[1][3]
| Hypokalemia | |
|---|---|
| Other names | Hypokalaemia, hypopotassaemia, hypopotassemia |
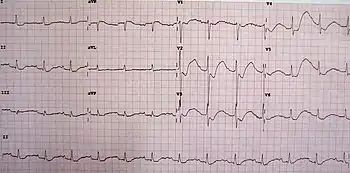 | |
| An ECG in a person with a potassium level of 1.1 meq/L showing the classical changes of ST segment depression, inverted T waves, large U waves, and a slightly prolonged PR interval. | |
| Specialty | Critical care medicine |
| Symptoms | Feeling tired, leg cramps, weakness, constipation, abnormal heart rhythm[1] |
| Complications | Cardiac arrest[1] |
| Causes | Diarrhea, medications like furosemide and steroids, dialysis, diabetes insipidus, hyperaldosteronism, hypomagnesemia, not enough intake in the diet[1] |
| Diagnostic method | Blood potassium < 3.5 mmol/L[1][2] |
| Treatment | Dietary changes, potassium supplements, based on the underlying cause[3] |
| Frequency | 20% of people admitted to hospital[4] |
Causes of hypokalemia include vomiting, diarrhea, medications like furosemide and steroids, dialysis, diabetes insipidus, hyperaldosteronism, hypomagnesemia, and not enough intake in the diet.[1] Normal potassium levels are between 3.5 and 5.0 mmol/L (3.5 and 5.0 mEq/L) with levels below 3.5 mmol/L defined as hypokalemia.[1][2] It is classified as severe when levels are less than 2.5 mmol/L.[1] Low levels may also be suspected based on an electrocardiogram (ECG).[1] Hyperkalemia is a high level of potassium in the blood serum.[1]
The speed at which potassium should be replaced depends on whether or not there are symptoms or abnormalities on an electrocardiogram.[1] Potassium levels that are only slightly below the normal range can be managed with changes in the diet.[3] Lower levels of potassium require replacement with supplements either taken by mouth or given intravenously.[3] If given intravenously, potassium is generally replaced at rates of less than 20 mmol/hour.[1] Solutions containing high concentrations of potassium (>40 mmol/L) should generally be given using a central venous catheter.[3] Magnesium replacement may also be required.[1]
Hypokalemia is one of the most common water–electrolyte imbalances.[4] It affects about 20% of people admitted to hospital.[4] The word hypokalemia comes from hypo- 'under' + kalium 'potassium' + -emia 'blood condition'.[5]
Signs and symptoms
Mild hypokalemia is often without symptoms, although it may cause elevation of blood pressure,[6] and can provoke the development of an abnormal heart rhythm. Severe hypokalemia, with serum potassium concentrations of 2.5–3 meq/L (Nl: 3.5–5.0 meq/L), may cause muscle weakness, myalgia, tremor, and muscle cramps (owing to disturbed function of skeletal muscle), and constipation (from disturbed function of smooth muscle). With more severe hypokalemia, flaccid paralysis and hyporeflexia may result. Reports exist of rhabdomyolysis occurring with profound hypokalemia with serum potassium levels less than 2 meq/L.[7] Respiratory depression from severe impairment of skeletal muscle function is found in some people.[8]
It can also cause psychotic as well as other mental symptoms.[9][10]
Causes
Hypokalemia can result from one or more of these medical conditions:
Inadequate potassium intake
Not eating a diet with enough potassium-containing foods or fasting can cause the gradual onset of hypokalemia. This is a rare cause and may occur in those with anorexia nervosa or those on a ketogenic diet.
Gastrointestinal or skin loss
A more common cause is excessive loss of potassium, often associated with heavy fluid losses that flush potassium out of the body. Typically, this is a consequence of diarrhea, excessive perspiration, or losses associated with muscle-crush injury, or surgical procedures. Vomiting can also cause hypokalemia, although not much potassium is lost from the vomitus. Rather, heavy urinary losses of K+ in the setting of post-emetic bicarbonaturia force urinary potassium excretion. (See discussion of alkalosis below.) Other gastrointestinal causes include pancreatic fistulae and the presence of adenoma.
Urinary loss
- Certain medications can cause excess potassium loss in the urine. Blood pressure medications such as loop diuretics (e.g. furosemide) and thiazide diuretics (e.g. hydrochlorothiazide) commonly cause hypokalemia. Other medications such as the antifungal amphotericin B or the cancer drug cisplatin can also cause long-term hypokalemia. Diuretic abuse among athletes[11] and people with eating disorders[12] may present with hypokalemia due to urinary potassium loss.
- A special case of potassium loss occurs with diabetic ketoacidosis. Hypokalemia is observed with low total body potassium and a low intracellular concentration of potassium. In addition to urinary losses from polyuria and volume contraction, also an obligate loss of potassium from kidney tubules occurs as a cationic partner to the negatively charged ketone, β-hydroxybutyrate.
- A low level of magnesium in the blood can also cause hypokalemia. Magnesium is required for adequate processing of potassium. This may become evident when hypokalemia persists despite potassium supplementation. Other electrolyte abnormalities may also be present.
- An increase in the pH of the blood (alkalosis) can cause temporary hypokalemia by causing a shift of potassium out of the plasma and interstitial fluids into the urine via a number of interrelated mechanisms.
1) Type B intercalated cells in the collecting duct reabsorb H+ and secrete HCO3, while in type A intercalated cells protons are secreted via both H+-K+ATPases and H+ ATP-ases on the apical/luminal surface of the cell. By definition, the H+-K+ATPase reabsorbs one potassium ion into the cell for every proton it secretes into the lumen of the collecting duct of a nephron. In addition, when H+ is expelled from the cell (by H+ATP-ase), cations—in this case potassium—are taken up by the cell in order to maintain electroneutrality (but not through direct exchange as with the H+-K+ATPase).[13] In order to correct the pH during alkalosis, these cells will use these mechanisms to reabsorb great amounts of H+, which will concomitantly increase their intracellular concentrations of potassium. This concentration gradient drives potassium to be secreted across the apical surface of the cell into the tubular lumen through potassium channels (this facilitated diffusion occurs in both Type B intercalated cells and Principal cells in the collecting duct).
2) Metabolic alkalosis is often present in states of volume depletion, such as vomiting, so potassium is also lost via aldosterone-mediated mechanisms.
3) During metabolic alkalosis, the acute rise of plasma HCO3− concentration (caused by vomiting, for example) will exceed the capacity of the renal proximal tubule to reabsorb this anion, and potassium will be excreted as an obligate cation partner to the bicarbonate.[14] - Disease states that lead to abnormally high aldosterone levels can cause hypertension and excessive urinary losses of potassium. These include renal artery stenosis and tumors (generally nonmalignant) of the adrenal glands, e.g., Conn's syndrome (primary hyperaldosteronism). Cushing's syndrome can also lead to hypokalemia due to excess cortisol binding the Na+/K+ pump and acting like aldosterone. Hypertension and hypokalemia can also be seen with a deficiency of the 11-beta-hydroxysteroid dehydrogenase type 2 enzyme which allows cortisols to stimulate aldosterone receptors. This deficiency—known as apparent mineralocorticoid excess syndrome—can either be congenital or caused by consumption of glycyrrhizin, which is contained in extract of licorice, sometimes found in herbal supplements, candies, and chewing tobacco.
- Rare hereditary defects of renal salt transporters, such as Bartter syndrome or Gitelman syndrome, can cause hypokalemia, in a manner similar to that of diuretics. As opposed to disease states of primary excesses of aldosterone, blood pressure is either normal or low in Bartter's or Gitelman's.
Distribution away from extracellular fluid
- In addition to alkalosis, other factors can cause transient shifting of potassium into cells, presumably by stimulation of the Na+/K+ pump.[15] These hormones and medications include insulin, epinephrine, and other beta agonists (e.g. salbutamol or salmeterol), and xanthines (e.g. theophylline).[16][17] Stimulants (amphetamines, methylphenidate, cocaine) can also cause hypokalemia by stimulating beta-2 receptors.[18][19]
- Rare hereditary defects of muscular ion channels and transporters that cause hypokalemic periodic paralysis can precipitate occasional attacks of severe hypokalemia and muscle weakness. These defects cause a heightened sensitivity to the normal changes in potassium produced by catecholamines and/or insulin and/or thyroid hormone, which lead to movement of potassium from the extracellular fluid into the muscle cells.
Other
- A handful of published reports describe individuals with severe hypokalemia related to chronic extreme consumption (4–10 L/day) of colas.[20] The hypokalemia is thought to be from the combination of the diuretic effect of caffeine[21] and copious fluid intake, although it may also be related to diarrhea caused by heavy fructose ingestion.[22][23]
Pseudohypokalemia
- Pseudohypokalemia is a decrease in the amount of potassium that occurs due to excessive uptake of potassium by metabolically active cells in a blood sample after it has been drawn. It is a laboratory artifact that may occur when blood samples remain in warm conditions for several hours before processing.[24]
Pathophysiology
About 98% of the body's potassium is found inside cells, with the remainder in the extracellular fluid including the blood. This concentration gradient is maintained principally by the Na+/K+ pump.
Potassium is essential for many body functions, including muscle and nerve activity. The electrochemical gradient of potassium between the intracellular and extracellular space is essential for nerve function; in particular, potassium is needed to repolarize the cell membrane to a resting state after an action potential has passed. Lower potassium levels in the extracellular space cause hyperpolarization of the resting membrane potential. This hyperpolarization is caused by the effect of the altered potassium gradient on resting membrane potential as defined by the Goldman equation. As a result, a greater-than-normal stimulus is required for depolarization of the membrane to initiate an action potential.
In the heart, hypokalemia causes arrhythmias because of less-than-complete recovery from sodium-channel inactivation, making the triggering of an action potential less likely. In addition, the reduced extracellular potassium (paradoxically) inhibits the activity of the IKr potassium current and delays ventricular repolarization. This delayed repolarization may promote reentrant arrhythmias.[25]
Diagnosis
Blood
Normal potassium levels are between 3.5 and 5.0 mmol/L with levels below 3.5 mmol/L (less than 3.5 mEq/L) defined as hypokalemia.[1][26]
Electrocardiogram
Hypokalemia leads to characteristic ECG changes (PR prolongation, ST-segment and T-wave depression, U-wave formation).[4]
The earliest electrocardiographic (ECG) findings, associated with hypokalemia, are decreased T wave height. Then, ST depressions and T inversions appear as serum potassium levels reduce further. Due to prolonged repolarization of ventricular Purkinje fibers, prominent U waves occur (usually seen at V2 and V3 leads), frequently superimposed upon T waves, therefore producing the appearance of prolonged QT intervals, when serum potassium levels fall below 3 mEq/L.[27]
Amount
The amount of potassium deficit can be calculated using the following formula:
Kdeficit (in mmol) = (Knormal lower limit − Kmeasured) × body weight (kg) × 0.4
Meanwhile, the daily body requirement of potassium is calculated by multiplying 1 mmol to body weight in kilograms. Adding potassium deficit and daily potassium requirement would give the total amount of potassium need to be corrected in mmol. Dividing mmol by 13.4 will give the potassium in grams.[28]
Treatment
Treatment includes addressing the cause, such as improving the diet, treating diarrhea, or stopping an offending medication. People without a significant source of potassium loss and who show no symptoms of hypokalemia may not require treatment. Acutely, repletion with 10 mEq of potassium is typically expected to raise serum potassium by 0.1 mEq/L immediately after administration. However, for those with chronic hypokalemia, repletion takes time due to tissue redistribution. For example, correction by 1 mEq/L can take more than 1000 mEq of potassium over many days.[6]
Oral potassium supplementation
Mild hypokalemia (>3.0 mEq/L) may be treated by eating potassium-containing foods or by taking potassium chloride supplements in a tablet or syrup form (by mouth supplements). Foods rich in potassium include dried fruits (particularly dried figs), nuts, bran cereals and wheat germ, lima beans, molasses, leafy green vegetables, broccoli, winter squash, beets, carrots, cauliflower, potatoes, avocados, tomatoes, coconut water, citrus fruits (particularly oranges), cantaloupe, kiwis, mangoes, bananas, and red meats.[29][30]
Eating potassium-rich foods may not be sufficient for correcting low potassium; potassium supplements may be recommended. Potassium contained in foods is almost entirely coupled with phosphate and is thus ineffective in correcting hypokalemia associated with hypochloremia that may occur due to vomiting, diuretic therapy, or nasogastric drainage. Additionally, replacing potassium solely through diet may be costly and result in weight gain due to potentially large amounts of food needed. An effort should also be made to limit dietary sodium intake due to an inverse relationship with serum potassium. Increasing magnesium intake may also be beneficial for similar physiological reasons.[30]
Potassium chloride supplements by mouth have the advantage of containing precise quantities of potassium, but the disadvantages of a taste which may be unpleasant, and the potential for side-effects including nausea and abdominal discomfort. Potassium bicarbonate is preferred when correcting hypokalemia associated with metabolic acidosis.[30]
Intravenous potassium replacement
Severe hypokalemia (<3.0 mEq/L) may require intravenous supplementation. Typically, a saline solution is used, with 20–40 meq/L KCl per liter over 3–4 hours.[31] Giving IV potassium at faster rates (20–25 meq/hr) may inadvertently expose the heart to a sudden increase in potassium, potentially causing dangerous abnormal heart rhythms such as heart block or asystole.[25] Faster infusion rates are therefore generally only performed in locations in which the heart rhythm can be continuously monitored such as a critical care unit.[31] When replacing potassium intravenously, particularly when higher concentrations of potassium are used, infusion by a central line is encouraged to avoid the occurrence of a burning sensation at the site of infusion, or the rare occurrence of damage to the vein.[32] When peripheral infusions are necessary, the burning can be reduced by diluting the potassium in larger amounts of fluid, or adding a small dose of lidocaine to the intravenous fluid,[31] although adding lidocaine may increase the likelihood of medical errors.[33] Even in severe hypokalemia, oral supplementation is preferred given its safety profile. Sustained-release formulations should be avoided in acute settings.
Potassium-sparing diuretics
Hypokalemia which is recurrent or resistant to treatment may be amenable to a potassium-sparing diuretic, such as amiloride, triamterene, spironolactone, or eplerenone. Concomitant hypomagnesemia will inhibit potassium replacement, as magnesium is a cofactor for potassium uptake.[30]
Popular culture
The plot of the science fiction novel Destiny's Road by Larry Niven centers around the setting's scarcity of available potassium, and the resulting deficiency and its effects on the world's colonists and their society.[34][35][36][37]
In the video game Deltarune, Queen expresses concern about one of the characters (Noelle) clipping into a wall and dying slowly from Hypokalemia.
See also
- Bartter syndrome
- Gitelman syndrome
- Hypokalemic acidosis
- Potassium deficiency (plant disorder)
- Superior mesenteric artery syndrome
References
- Soar, J; Perkins, GD; Abbas, G; Alfonzo, A; Barelli, A; Bierens, JJ; Brugger, H; Deakin, CD; Dunning, J; Georgiou, M; Handley, AJ; Lockey, DJ; Paal, P; Sandroni, C; Thies, KC; Zideman, DA; Nolan, JP (October 2010). "European Resuscitation Council Guidelines for Resuscitation 2010 Section 8. Cardiac arrest in special circumstances: Electrolyte abnormalities, poisoning, drowning, accidental hypothermia, hyperthermia, asthma, anaphylaxis, cardiac surgery, trauma, pregnancy, electrocution". Resuscitation. 81 (10): 1400–33. doi:10.1016/j.resuscitation.2010.08.015. PMID 20956045.
- Pathy, M.S. John (2006). "Appendix 1: Conversion of SI Units to Standard Units". Principles and Practice of Geriatric Medicine. Vol. 2 (4. ed.). Chichester: Wiley. p. Appendix. doi:10.1002/047009057X.app01. ISBN 9780470090558.
- Zieg, J; Gonsorcikova, L; Landau, D (July 2016). "Current views on the diagnosis and management of hypokalaemia in children". Acta Paediatrica. 105 (7): 762–72. doi:10.1111/apa.13398. PMID 26972906. S2CID 19579505.
- Marx, John; Walls, Ron; Hockberger, Robert (2013). Rosen's Emergency Medicine - Concepts and Clinical Practice (8 ed.). Elsevier Health Sciences. p. 1639. ISBN 978-1455749874. Archived from the original on 2016-08-15.
- Herlihy, Barbara (2014). The Human Body in Health and Illness. Elsevier Health Sciences. p. 487. ISBN 9781455756421. Archived from the original on 2016-10-01.
- Krishna, GG; Miller, E; Kapoor, S (1989). "Increased blood pressure during potassium depletion in normotensive men". The New England Journal of Medicine. 320 (18): 1177–82. doi:10.1056/NEJM198905043201804. PMID 2624617.
- Jain, VV; Gupta, OP; Jajoo, SU; Khiangate, B (January 2011). "Hypokalemia induced rhabdomyolysis". Indian Journal of Nephrology. 21 (1): 66. doi:10.4103/0971-4065.78085. PMC 3109789. PMID 21655176.
- Taal, Maarten W.; Chertow, Glenn M.; Marsden, Philip A.; Skorecki, Karl; Yu, Alan S. L.; Brenner, Barry M. (2011). Brenner and Rector's The Kidney E-Book. Elsevier Health Sciences. p. 618. ISBN 9781455723041.
- "Symptoms and Signs of Low Potassium (Hypokalemia)". Retrieved 2021-04-21.
- Hong, Ella (2016). "Hypokalemia and Psychosis: A Forgotten Association". American Journal of Psychiatry Residents' Journal. 11 (11): 6–7. doi:10.1176/appi.ajp-rj.2016.111103. Retrieved 2021-04-21.
- Cadwallader, Amy B; De La Torre, Xavier; Tieri, Alessandra; Botrè, Francesco (September 2010). "The abuse of diuretics as performance-enhancing drugs and masking agents in sport doping: pharmacology, toxicology and analysis: Diuretics in sport doping". British Journal of Pharmacology. 161 (1): 1–16. doi:10.1111/j.1476-5381.2010.00789.x. PMC 2962812. PMID 20718736.
- Mascolo, Margherita; Chu, Eugene S.; Mehler, Philip S. (April 2011). "Abuse and clinical value of diuretics in eating disorders therapeutic applications". International Journal of Eating Disorders. 44 (3): 200–202. doi:10.1002/eat.20814. PMID 20186716.
- Silverthorn, Dee Unglaub (2016). Human Physiology: An Integrated Approach (7th ed.). Pearson Education. pp. 646–647. ISBN 978-0-321-98122-6.
- Walmsley RN, White GH (August 1984). "Occult causes of hypokalaemia". Clin. Chem. 30 (8): 1406–8. doi:10.1093/clinchem/30.8.1406. PMID 6744598.
- Halperin, ML; Kamel, KS (1998). "Potassium". Lancet. 352 (9122): 135–40. doi:10.1016/S0140-6736(98)85044-7. PMID 9672294. S2CID 208790031.
- Whyte KF, Addis GJ, Whitesmith R, Reid JL (April 1987). "Failure of chronic theophylline therapy to alter circulating catecholamines". Eur J Respir Dis. 70 (4): 221–8. PMID 3582518.
- Veltri KT, Mason C (March 2015). "Medication-induced hypokalemia". P & T: A Peer-Reviewed Journal for Formulary Management. 40 (3): 185–190. ISSN 1052-1372. PMC 4357351. PMID 25798039.
- Charach G, Karniel E, Grosskopf I, Rabinovich A, Charach L (2 July 2020). "Methylphenidate has mild hyperglycemic and hypokalemia effects and increases leukocyte and neutrophil counts". Medicine. 99 (27): e20931. doi:10.1097/MD.0000000000020931. eISSN 1536-5964. ISSN 0025-7974. PMC 7337440. PMID 32629693.
- Alazami M (8 February 2006). "Unusual causes of hypokalaemia and paralysis". QJM. 99 (3): 181–192. doi:10.1093/qjmed/hcl011. ISSN 1460-2725. PMID 16469765.
- Tsimihodimos V, Kakaidi V, Elisaf M (June 2009). "Cola-induced hypokalaemia: pathophysiological mechanisms and clinical implications". International Journal of Clinical Practice. 63 (6): 900–2. doi:10.1111/j.1742-1241.2009.02051.x. PMID 19490200. S2CID 26191242.
- Shirley DG, Walter SJ, Noormohamed FH (November 2002). "Natriuretic effect of caffeine: assessment of segmental sodium reabsorption in humans". Clin. Sci. 103 (5): 461–6. doi:10.1042/cs1030461. PMID 12401118. S2CID 18740906.
- Packer, C.D. (June 2009). "Cola-induced hypokalaemia: a super-sized problem". International Journal of Clinical Practice. 63 (6): 833–5. doi:10.1111/j.1742-1241.2009.02066.x. PMID 19490191. S2CID 2856903.
- HealthGuru (2012-03-01). "Health.yahoo.com". Health.yahoo.com. Archived from the original on 2009-06-12. Retrieved 2012-03-10.
- Sodi R, Davison AS, Holmes E, Hine TJ, Roberts NB (June 2009). "The phenomenon of seasonal pseudohypokalemia: effects of ambient temperature, plasma glucose and role for sodium-potassium-exchanging-ATPase". Clin. Biochem. 42 (9): 813–8. doi:10.1016/j.clinbiochem.2009.01.024. PMID 19232334.
- Khan, Ehsan; Spiers, Christine; Khan, Maria (March 2013). "The heart and potassium: a banana republic". Acute Cardiac Care. 15 (1): 17–24. doi:10.3109/17482941.2012.741250. PMID 23425010. S2CID 35971172.
- "Potassium (Unit Conversion)". MediCalc. Archived from the original on 1 October 2016. Retrieved 27 September 2016.
- Levis, Joel T (2012). "ECG Diagnosis: Hypokalemia". The Permanente Journal. 16 (2): 57. doi:10.7812/tpp/12-015. PMC 3383164. PMID 22745618.
- Ingelfinger, Julie R (1 July 2015). "Fluids and Electrolytes Challenge - Disorders of Fluids and Electrolytes - Integrated View of Potassium Homeostasis". New England Journal of Medicine. doi:10.1056/feature.2015.06.16.43 (inactive 31 July 2022). Retrieved 16 November 2017.
{{cite journal}}: CS1 maint: DOI inactive as of July 2022 (link) - "Sources of Dietary Potassium" (PDF). University of Massachusetts Medical School. Archived from the original (PDF) on 3 January 2017. Retrieved 3 February 2017.
- Cohn, Jay N.; Kowey, Peter R.; Whelton, Paul K.; Prisant, L. Michael (2000-09-11). "New Guidelines for Potassium Replacement in Clinical Practice". Archives of Internal Medicine. 160 (16): 2429–36. doi:10.1001/archinte.160.16.2429. PMID 10979053.
- Kraft, Michael D.; Btaiche, Imad F.; Sacks, Gordon S.; Kudsk, Kenneth A. (2005-08-15). "Treatment of electrolyte disorders in adult patients in the intensive care unit". American Journal of Health-System Pharmacy. 62 (16): 1663–1682. doi:10.2146/ajhp040300. PMID 16085929.
- "How should intravenous (IV) potassium chloride be administered in adults? – SPS - Specialist Pharmacy Service – The first stop for professional medicines advice". www.sps.nhs.uk. Retrieved 2018-10-16.
- "Safety Issues With Adding Lidocaine to IV Potassium Infusions (Excerpt)". Archived from the original on 2008-12-22. Retrieved 2009-05-09.
- Clute, John (2003). "Wiser Book". Scores: Reviews 1993–2003. Harold Wood, London, UK: Beccon. ISBN 9781870824477. OCLC 53123451. Retrieved 13 August 2019. Originally published as "Excessive Candor" no. 48 in Science Fiction Weekly no. 48, 16 June 1997
{{cite book}}: CS1 maint: postscript (link) - Di Filippo, Paul (8 June 1997). "Destiny's Road". The Universe of Larry Niven. Retrieved 13 August 2019. Reprints the review from the July 1997 issue of Science Fiction Age.
- "Destiny's road". Open Library. 17 August 2010. OL 1012547M.
{{cite journal}}: Cite journal requires|journal=(help) - ambidexteri (26 January 2013). "Review of Destiny's Road by Larry Niven". Ambidexteri. Retrieved 4 August 2019.
Further reading
- Firth, J (2010). "Disorders of potassium homeostasis". In David A. Warrell; Timothy M. Cox; John D. Firth; Graham S. Ogg (eds.). Oxford Textbook of Medicine. Vol. 1 (5th ed.). Oxford: Oxford University Press. pp. 3831–3845. doi:10.1093/med/9780199204854.003.210202_update_001. ISBN 978-0199204854.
- Greenlee, M; Wingo, CS; McDonough, AA; Youn, JH; Kone, BC (May 5, 2009). "Narrative review: evolving concepts in potassium homeostasis and hypokalemia" (PDF). Annals of Internal Medicine. 150 (9): 619–25. doi:10.7326/0003-4819-150-9-200905050-00008. PMC 4944758. PMID 19414841. NIHMSID: NIHMS800438.