Radial head fracture
| Radial head fracture | |
|---|---|
 | |
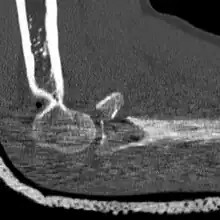
| Radial head fracture (red arrow) with posterior and anterior sail sign (blue arrows) | |
| Specialty | Orthopedic |
| Symptoms | Pain and swelling of the elbow[1] |
| Complications | Elbow stiffness[1] |
| Usual onset | 20s to 60s yr old[2] |
| Types | Type I, II, III, IV[3] |
| Causes | Fall on an outstretched arm[1] |
| Diagnostic method | X-rays[1] |
| Treatment | Arm sling or splint followed by mobilization, surgery[4] |
| Frequency | Relatively common (1 in 2,500 people a year)[1] |
Radial head fractures are a type of elbow fracture that typically occurs after a fall on an outstretched arm.[1][5] Symptoms generally include pain and swelling around the elbow.[1] There may also be difficulty moving the elbow or forearm.[4] About 30% of people have additional injuries.[5] Complications may include decreased ability to move the elbow.[1]
Most occur as a result of a fall onto a unbend or minimally bend elbow; though they may also occur due to a direct hit.[2] Diagnosis is generally based on X-rays, though the only indication may be a joint effusion.[1][2] They may be divided into four main types by the Mason classification.[3]
Treatment is based on the fracture type.[4] If the fracture is well aligned an arm sling for a few days followed by a gradual return to using it normally may be all that is required.[4] If the fracture is misaligned < 2 mm, an arm sling may be worn for a couple of weeks followed by physiotherapy.[4][3] For fractures with greater misalignment, surgery to place screws or remove peices of bone may be required.[4] For extensive fractures, the radial head may require replacement.[4] After surgery it can take 3 months to return to normal activity.[4]
Radial head fractures are relatively common, occurring in about 1 in 2,500 people a year.[1] They represent about a third of elbow fractures.[1] They most commonly occur in a person's 20s to 60s.[2] Women are more commonly affected than men.[4] The first in-depth classification of radial head fractures was in 1954 by Mark L. Mason.[1]
Signs and symptoms
Complications
Some of the more common complications of unstable radial head fractures includes stiffness, poor bone healing, nerve damage, and pain/prominent hardware.[6]
Diagnosis
Radial head fractures are diagnosed from an assessment and diagnostic imaging. Assessment may include pain or tenderness at the radial head, bruising, swelling, and a limited range of motion of the elbow.[7] Diagnostic imaging may include ultrasound, plain X-ray, CT scan, and magnetic resonance imaging (MRI).[7][8] A fat pad sign may be present on diagnostic imaging and may indicate a radial head fracture.[9]
 CT scan demonstrating the Mason type III radial head fracture
CT scan demonstrating the Mason type III radial head fracture CT scan showing a radial head fracture
CT scan showing a radial head fracture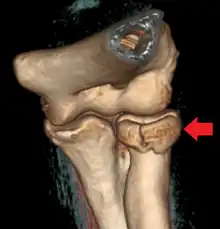 Radial head fracture seen on 3D CT reconstruction
Radial head fracture seen on 3D CT reconstruction
Classification
A diagnosed radial head fracture can be classified according to the Mason classification, also known as Mason-Johnston system.[3][10]
| Type | Description |
|---|---|
| 1 | Non-displaced fracture |
| 2 | Displacement >2mm |
| 3 | Comminuted fracture |
| 4 | Radial head fracture with dislocation of the elbow |
Treatment
Radial head fracture treatment is informed by the Mason-Johnston classification, patient symptoms, and fracture stability. An unstable fracture will involve fracture displacement, fractures to adjacent structures and injury to other associated soft tissues. A stable type 1 radial head fracture is typically managed with conservative measures including joint aspiration, immobilization in a sling for a few days and followed by early range of motion exercises.[7][6] If range of motion is still limited after joint aspiration it may indicate a mechanical block which is treated surgically.[9] Stable type 2 radial head fractures may be treated as a type 1 if the displacement is minimal. Unstable type 2 - 4 fractures generally warrant surgery. Surgical correction can include fracture fragment excision, radial head reconstruction, open reduction and internal fixation, and radial head excision with artificial replacement.[6] Associated structures that were damaged during the injury may also need to be repaired.
Rehabilitation exercises are recommended and tailored to fracture and treatment type. It is recommended to wait 6 weeks before resuming load bearing with a stable type 1 fracture and 10-12 weeks following surgery for unstable type 2-4 fractures.[11]
Prognosis
Stable type 1 and 2 radial head fractures often have good outcomes with most cases regaining complete range of motion and having minimal residual stiffness or pain.[9] Outcomes for unstable type 2-4 radial head fractures vary greatly depending on the severity of the injury and the surgical intervention.[9][6]
References
- 1 2 3 4 5 6 7 8 9 10 11 12 Khawar, Haseeb; Craxford, Simon; Ollivere, Benjamin (2 April 2020). "Radial head fractures". British Journal of Hospital Medicine. 81 (4): 1–6. doi:10.12968/hmed.2019.0404.
- 1 2 3 4 Mous, Anon Ny. "Radial head fracture | Radiology Reference Article | Radiopaedia.org". Radiopaedia. Archived from the original on 18 February 2023. Retrieved 3 July 2023.
- 1 2 3 4 5 Jones, Jeremy. "Mason classification of radial head fractures | Radiology Reference Article | Radiopaedia.org". Radiopaedia. Archived from the original on 9 August 2022. Retrieved 3 July 2023.
- 1 2 3 4 5 6 7 8 9 "Radial Head Fractures of the Elbow - OrthoInfo - AAOS". www.orthoinfo.org. Archived from the original on 21 May 2023. Retrieved 3 July 2023.
- 1 2 van Riet, RP; van den Bekerom, M; Van Tongel, A; Spross, C; Barco, R; Watts, AC (June 2020). "Radial head fractures". Shoulder & elbow. 12 (3): 212–223. doi:10.1177/1758573219876921. PMID 32565923.
- 1 2 3 4 Rosenblatt, Yishai; Athwal, George S.; Faber, Kenneth J. (April 2008). "Current Recommendations for the Treatment of Radial Head Fractures". Orthopedic Clinics of North America. 39 (2): 173–185. doi:10.1016/j.ocl.2007.12.008. PMID 18374808. Archived from the original on 2023-01-02. Retrieved 2023-02-12.
- 1 2 3 Bennett, James B. (September 1993). "Radial head fractures: Diagnosis and management". Journal of Shoulder and Elbow Surgery. 2 (5): 264–273. doi:10.1016/S1058-2746(09)80088-8. PMID 22959508. Archived from the original on 2023-04-11. Retrieved 2023-02-12.
- ↑ Pavić, Roman; Margetić, Petra; Hnatešen, Dijana (November 2015). "Diagnosis of occult radial head and neck fracture in adults". Injury. 46: S119–S124. doi:10.1016/j.injury.2015.10.050. PMID 26584731. Archived from the original on 2023-03-14. Retrieved 2023-02-12.
- 1 2 3 4 Duckworth, A. D.; McQueen, M. M.; Ring, D. (February 2013). "Fractures of the radial head". The Bone & Joint Journal. 95-B (2): 151–159. doi:10.1302/0301-620X.95B2.29877. ISSN 2049-4394. PMID 23365021. Archived from the original on 2023-04-11. Retrieved 2023-02-12.
- ↑ Kaas, Laurens; van Riet, Roger P.; Vroemen, Jos P.A.M.; Eygendaal, Denise (June 2010). "The epidemiology of radial head fractures". Journal of Shoulder and Elbow Surgery. 19 (4): 520–523. doi:10.1016/j.jse.2009.10.015. PMID 20149972. Archived from the original on 2022-12-28. Retrieved 2023-02-12.
- ↑ Hackl, Michael; Leschinger, Tim; Uschok, Stephan; Müller, Lars Peter; Wegmann, Kilian (December 2017). "Rehabilitation of elbow fractures and dislocations". Obere Extremität. 12 (4): 201–207. doi:10.1007/s11678-017-0425-1. ISSN 1862-6599. S2CID 79629978. Archived from the original on 2023-04-11. Retrieved 2023-02-12.
External links
| Classification |
|---|