Sotos syndrome
| Sotos syndrome | |
|---|---|
| Other names: Cerebral gigantism or Sotos-Dodge syndrome | |
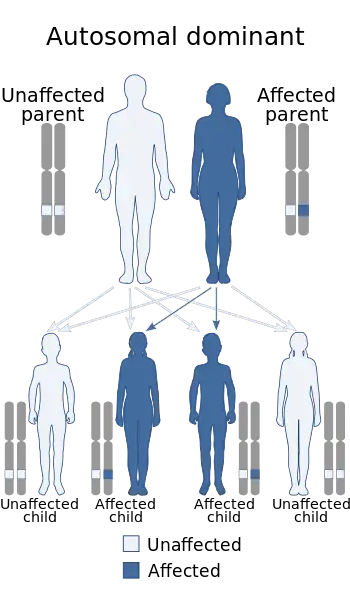 | |
| Sotos syndrome is an autosomal dominant inherited condition | |
Sotos syndrome is a rare genetic disorder characterized by excessive physical growth during the first years of life. Excessive growth often starts in infancy and continues into the early teen years. The disorder may be accompanied by autism,[1] mild intellectual disability, delayed motor, cognitive, and social development, hypotonia (low muscle tone), and speech impairments. Children with Sotos syndrome tend to be large at birth and are often taller, heavier, and have relatively large skulls (macrocephaly) than is normal for their age. Signs of the disorder, which vary among individuals, include a disproportionately large skull with a slightly protrusive forehead, large hands and feet, large mandible, hypertelorism (an abnormally increased distance between the eyes), and downslanting eyes. Clumsiness, an awkward gait, and unusual aggressiveness or irritability may also occur. Although most cases of Sotos syndrome occur sporadically, familial cases have also been reported. It is similar to Weaver syndrome.
Signs and symptoms
This syndrome is characterized by overgrowth and advanced bone age. Affected individuals are dysmorphic, with macrodolichocephaly, downslanting palpebral fissures and a pointed chin. The facial appearance is most notable in early childhood. Affected infants and children tend to grow quickly; they are significantly taller than their siblings and peers, and have an unusually large skull and large head. Adult height is usually in the normal range, although Broc Brown has the condition and was named the world's tallest teenager. As of late 2016, he was 7'8" and still growing.[2]
Individuals with Sotos syndrome often have intellectual impairment,[3][4] and most also display autistic traits.[5] Frequent behavioral impairments include attention deficit hyperactivity disorder (ADHD), phobias, obsessive compulsive disorder, tantrums, and impulsive behaviors (impulse control disorder). Problems with speech and language are also common.[6] Affected individuals may often have stuttering, difficulty with sound production, or a monotone voice. Additionally, weak muscle tone (hypotonia) may delay other aspects of early development, particularly motor skills such as sitting and crawling.
Other signs include scoliosis, seizures, heart or kidney defects, hearing loss, and problems with vision. Some infants with this disorder experience jaundice and poor feeding. A small number of patients with Sotos syndrome have developed cancer, most often in childhood, but no single form of cancer has been associated with this condition. It remains uncertain whether Sotos syndrome increases the risk of specific types of cancer. If persons with this disorder have any increased cancer risk, their risk is only slightly greater than that of the general population.[7]
 a) Prominent superciliary arches, prognathism b) prominent frontal/maxillary sinuses c) large sphenoid
a) Prominent superciliary arches, prognathism b) prominent frontal/maxillary sinuses c) large sphenoid Child with Sotos syndrome showing characteristic facial features
Child with Sotos syndrome showing characteristic facial features
Genetics
Mutations in the NSD1 gene cause Sotos syndrome.[8][9] The NSD1 gene provides instructions for making a protein (histone methyltransferase) that is involved in normal growth and development. The function of this protein is unknown, however. In the Japanese population, the most common genetic change leading to Sotos syndrome deletes genetic material from the region of chromosome 5 containing the NSD1 gene. In other populations, small mutations within the NSD1 gene occur more frequently. Genetic changes involving the NSD1 gene prevent one copy of the gene from producing any functional protein. It is unclear how a reduced amount of this protein during development leads to learning disabilities, overgrowth, and the other features of Sotos syndrome.
About 95 percent of Sotos syndrome cases occur by spontaneous mutation. Most of these cases result from new mutations involving the NSD1 gene. A few families have been described with more than one affected family member. These inherited cases enabled researchers to determine that Sotos syndrome has an autosomal dominant pattern of inheritance.
Diagnosis
Diagnosis is based on physical examination, looking for excessive growth among other symptoms. There are no biochemical markers for the disease.[10]
Treatment
Treatment is symptomatic.[10] There is no standard course of treatment for Sotos syndrome.
Prognosis
Sotos syndrome is not a life-threatening disorder and patients may have a normal life expectancy. Developmental delays may improve in the school-age years; however, coordination problems may persist into adulthood, along with any learning disabilities and/or other physical or mental issues.
Epidemiology
Incidence is approximately 1 in 14,000 births.[11]
See also
References
- ↑ "Archive copy". Archived from the original on 2012-07-29. Retrieved 2021-08-11.
{{cite web}}: CS1 maint: archived copy as title (link) - ↑ "7-foot-tall Broc Brown: Facts". Morning News USA. Archived from the original on 12 March 2017. Retrieved 8 March 2017.
- ↑ Lane C, Milne E, Freeth M (2016). "Cognition and Behaviour in Sotos Syndrome: A Systematic Review". PLOS ONE. 11 (2): e0149189. Bibcode:2016PLoSO..1149189L. doi:10.1371/journal.pone.0149189. PMC 4752321. PMID 26872390.
- ↑ Lane C, Milne E, Freeth M (January 2018). "The cognitive profile of Sotos syndrome" (PDF). J Neuropsychol. 13 (2): 240–252. doi:10.1111/jnp.12146. PMID 29336120. Archived (PDF) from the original on 2019-04-27. Retrieved 2021-08-11.
- ↑ Lane C, Milne E, Freeth M (January 2017). "Characteristics of Autism Spectrum Disorder in Sotos Syndrome". J Autism Dev Disord. 47 (1): 135–143. doi:10.1007/s10803-016-2941-z. PMC 5222916. PMID 27771801.
- ↑ Lane C, Van Herwegen J, Freeth M (December 2018). "Parent-Reported Communication Abilities of Children with Sotos Syndrome: Evidence from the Children's Communication Checklist-2". J Autism Dev Disord. 49 (4): 1475–1483. doi:10.1007/s10803-018-3842-0. PMC 6450847. PMID 30536215.
- ↑ Reference, Genetics Home. "Sotos syndrome". Genetics Home Reference. Archived from the original on 2020-10-01. Retrieved 2021-08-11.
- ↑ Kurotaki N, Imaizumi K, Harada N, Masuno M, Kondoh T, Nagai T, et al. (April 2002). "Haploinsufficiency of NSD1 causes Sotos syndrome". Nat. Genet. 30 (4): 365–6. doi:10.1038/ng863. PMID 11896389. S2CID 205357840.
- ↑ Melchior L, Schwartz M, Duno M (March 2005). "dHPLC screening of the NSD1 gene identifies nine novel mutations--summary of the first 100 Sotos syndrome mutations". Ann. Hum. Genet. 69 (Pt 2): 222–6. doi:10.1046/j.1529-8817.2004.00150.x. PMID 15720303.
- 1 2 "Sotos Syndrome". NORD (National Organization for Rare Disorders). Archived from the original on 2016-03-05. Retrieved 2016-03-01.
- ↑ "Latest Australian & World News". Yahoo7 News. Archived from the original on 2013-04-01. Retrieved 2016-03-01.
External links
| Classification |
|---|