Osgood–Schlatter disease
| Osgood–Schlatter disease | |
|---|---|
| Other names: Apophysitis of the tibial tubercle, Lannelongue's disease,[1] osteochondrosis of the tibial tubercle[2] | |
 | |
| Lateral view X-ray of the knee demonstrating fragmentation of the tibial tubercle with overlying soft tissue swelling. | |
| Specialty | Orthopedics |
| Symptoms | Painful bump just below the knee, worse with activity and better with rest[3] |
| Usual onset | Males between the ages of 10 and 15[3] |
| Duration | Few weeks to months[3][4] |
| Risk factors | Sports that involve running or jumping[3] |
| Diagnostic method | Based on symptoms[3] |
| Treatment | Applying cold, stretching, strengthening exercises[3] |
| Medication | NSAIDs |
| Prognosis | Good[3] |
| Frequency | ~4%[5] |
Osgood–Schlatter disease (OSD) is inflammation of the patellar ligament at the tibial tuberosity (apophysitis).[3] It is characterized by a painful bump just below the knee that is worse with activity and better with rest.[3] Episodes of pain typically last a few weeks to months.[3][4] One or both knees may be affected and flares may recur.[3][6]
Risk factors include overuse, especially sports which involve frequent running or jumping.[3] The underlying mechanism is repeated tension on the growth plate of the upper tibia.[3] Diagnosis is typically based on the symptoms.[3] A plain X-ray may be either normal or show fragmentation in the attachment area.[3]
Pain typically resolves with time.[3] Applying cold to the affected area, rest, stretching, and strengthening exercises may help.[3][4] NSAIDs such as ibuprofen may be used.[6] Slightly less stressful activities such as swimming or walking may be recommended.[3] Casting the leg for a period of time may help.[4] After growth slows, typically age 16 in boys and 14 in girls, the pain will no longer occur despite a bump potentially remaining.[6][7]
About 4% of people are affected at some point in time.[5] Males between the ages of 10 and 15 are most often affected.[3] The condition is named after Robert Bayley Osgood (1873–1956), an American orthopedic surgeon, and Carl B. Schlatter (1864–1934), a Swiss surgeon, who described the condition independently in 1903.[1][8]
Signs and symptoms
Osgood–Schlatter disease causes pain in the front lower part of the knee.[9] This is usually at the ligament-bone junction of the patellar ligament and the tibial tuberosity.[10] The tibial tuberosity is a slight elevation of bone on the anterior and proximal portion of the tibia. The patellar tendon attaches the anterior quadriceps muscles to the tibia via the knee cap.[11]
Intense knee pain is usually the presenting symptom that occurs during activities such as running, jumping, lifting things, squatting, and especially ascending or descending stairs and during kneeling.[12] The pain is worse with acute knee impact. The pain can be reproduced by extending the knee against resistance, stressing the quadriceps, or striking the knee. Pain is initially mild and intermittent. In the acute phase, the pain is severe and continuous in nature. Impact of the affected area can be very painful. Bilateral symptoms are observed in 20–30% of people.[13]
Risk factors
Risk factors include overuse, especially sports which involve running or jumping.[3] The underlying mechanism is repeated tension on the growth plate of the upper tibia.[3] It also occurs frequently in male pole vaulters aged 14–22.[14]
Diagnosis
Diagnosis is made based on signs and symptoms.[15]
Ultrasonography
This test can see various warning signs that predict if OSD might occur. Ultrasonography can detect if there is any tissue swelling and cartilage swelling.[11] Ultrasonography's main goal is to identify OSD in the early stage rather than later on. It has unique features such as detection of an increase of swelling within the tibia or the cartilage surrounding the area and can also see if there is any new bone starting to build up around the tibial tuberosity.
Types
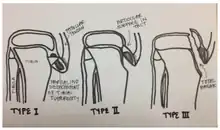
OSD may result in an avulsion fracture, with the tibial tuberosity separating from the tibia (usually remaining connected to a tendon or ligament). This injury is uncommon because there are mechanisms that prevent strong muscles from doing damage. The fracture on the tibial tuberosity can be a complete or incomplete break.
Type I: A small fragment is displaced proximally and does not require surgery.
Type II: The articular surface of the tibia remains intact and the fracture occurs at the junction where the secondary center of ossification and the proximal tibial epiphysis come together (may or may not require surgery).
Type III: Complete fracture (through articular surface) including high chance of meniscal damage. This type of fracture usually requires surgery.
Differential diagnosis
Sinding-Larsen and Johansson syndrome,[16] is an analogous condition involving the patellar tendon and the lower margin of the patella bone, instead of the upper margin of the tibia. Sever's disease is an analogous condition affecting the Achilles tendon attachment to the heel.
Prevention

One of the main ways to prevent OSD is to check the participant's flexibility in their quadriceps and hamstrings. Lack of flexibility in these muscles can be direct risk indicator for OSD. Muscles can shorten, which can cause pain but this is not permanent.[17] Stretches can help reduce shortening of the muscles. The main stretches for prevention of OSD focus on the hamstrings and quadriceps.[18]
Treatment
Treatment is generally conservative with rest, ice, and specific exercises being recommended.[19] Simple pain medication may be used such as acetaminophen (paracetamol), or NSAIDs such as ibuprofen.[20] Typically symptoms resolve as the growth plate closes.[19] Physiotherapy is generally recommended once the initial symptoms have improved to prevent recurrence.[19] Surgery may rarely be used in those who have stopped growing yet still have symptoms.[19]
Physiotherapy
Recommended efforts include exercises to improve the strength of the quadriceps, hamstring and gastrocnemius muscles.[19]
Bracing or use of an orthopedic cast to enforce joint immobilization is rarely required and does not necessarily encourage a quicker resolution. However, bracing may give comfort and help reduce pain as it reduces strain on the tibial tubercle.[21]
Surgery
Surgical excision may rarely be required in people who have stopped growing.[22] Surgical removal of the ossicles generally results in good outcomes, with symptoms improvement after several weeks.[23]
Rehabilitation

Rehabilitation focuses on muscle strengthening, gait training, and pain control to restore knee function.[24] Nonsurgical treatments for less severe symptoms include: exercises for strength, stretches to increase range of motion, ice packs, knee tape, knee braces, anti-inflammatory agents, and electrical stimulation to control inflammation and pain. Quadriceps and hamstring exercises prescribed by rehabilitation experts restore flexibility and muscle strength.
Education and knowledge on stretches and exercises is important. Exercises should lack pain and increase gradually with intensity. The patient is given strict guidelines on how to perform exercises at home to avoid more injury.[24] Exercises can include leg raises, squats, and wall stretches to increase quadriceps and hamstring strength. This helps to avoid pain, stress, and tight muscles that lead to further injury that oppose healing. Knee orthotics such as patella straps and knee sleeves help decrease force traction and prevent painful tibia contact by restricting unnecessary movement, providing support, and also adding compression to the area of pain.
Prognosis
The condition is usually self-limiting and is caused by stress on the patellar tendon that attaches the quadriceps muscle at the front of the thigh to the tibial tuberosity. Following an adolescent growth spurt, repeated stress from contraction of the quadriceps is transmitted through the patellar tendon to the immature tibial tuberosity. This can cause multiple subacute avulsion fractures along with inflammation of the tendon, leading to excess bone growth in the tuberosity and producing a visible lump which can be very painful, especially when hit. Activities such as kneeling may also irritate the tendon.
The syndrome may develop without trauma or other apparent cause; however, some studies report up to 50% of patients relate a history of precipitating trauma. Several authors have tried to identify the actual underlying etiology and risk factors that predispose Osgood–Schlatter disease and postulated various theories. However, currently it is widely accepted that Osgood–Schlatter disease is a traction apophysitis of the proximal tibial tubercle at the insertion of the patellar tendon caused by repetitive micro-trauma. In other words, Osgood–Schlatter disease is an overuse injury and closely related to the physical activity of the child. It was shown that children who actively participate in sports are affected more frequently as compared with non-participants. In a retrospective study of adolescents, old athletes actively participating in sports showed a frequency of 21% reporting the syndrome compared with only 4.5% of age-matched nonathletic controls.[25]
The symptoms usually resolve with treatment but may recur for 12–24 months before complete resolution at skeletal maturity, when the tibial epiphysis fuses. In some cases the symptoms do not resolve until the patient is fully grown. In approximately 10% of patients the symptoms continue unabated into adulthood, despite all conservative measures.[22]
Long-term implications
OSD occurs from the combined effects of tibial tuberosity immaturity and quadriceps tightness.[11] There is a possibility of migration of the ossicle or fragmentation in Osgood-Schlatter patients.[10] The implications of OSD and the ossification of the tubercle can lead to functional limitations and pain for patients into adulthood.[18]
Of people admitted with OSD, about half were children who were between the ages of 1 and 17. In addition, in 2014, a case study of 261 patients was observed over 12 to 24 months. 237 of these people responded well to sport restriction and non-steroid anti-inflammatory agents, which resulted in recovery to normal athletic activity.[26]
Epidemiology
Osgood–Schlatter disease generally occurs in boys and girls aged 9–16[27] coinciding with periods of growth spurts. It occurs more frequently in boys than in girls, with reports of a male-to-female ratio ranging from 3:1 to as high as 7:1. It has been suggested that difference is related to a greater participation by boys in sports and risk activities than by girls.[28]
References
- 1 2 "Osgood-Schlatter disease". whonamedit. Archived from the original on 12 July 2017. Retrieved 4 June 2017.
- ↑ Smith, James; Varacallo, Matthew (15 November 2018). "Osgood Schlatter Disease". StatPearls. PMID 28723024. Archived from the original on 28 August 2021. Retrieved 21 January 2019.
{{cite journal}}: Cite journal requires|journal=(help) - 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 "Questions and Answers About Knee Problems". www.niams.nih.gov. 2017-04-05. Archived from the original on 13 May 2017. Retrieved 4 June 2017.
- 1 2 3 4 Vaishya, R; Azizi, AT; Agarwal, AK; Vijay, V (13 September 2016). "Apophysitis of the Tibial Tuberosity (Osgood-Schlatter Disease): A Review". Cureus. 8 (9): e780. doi:10.7759/cureus.780. PMC 5063719. PMID 27752406.
- 1 2 Ferri, Fred F. (2013). Ferri's Clinical Advisor 2014 E-Book: 5 Books in 1. Elsevier Health Sciences. p. 804. ISBN 978-0323084314. Archived from the original on 2017-09-10.
- 1 2 3 4 "Osgood-Schlatter Disease (Knee Pain)". orthoinfo.aaos.org. May 2015. Archived from the original on 18 June 2017. Retrieved 3 June 2017.
- ↑ Circi, E; Atalay, Y; Beyzadeoglu, T (December 2017). "Treatment of Osgood-Schlatter disease: review of the literature". Musculoskeletal Surgery. 101 (3): 195–200. doi:10.1007/s12306-017-0479-7. PMID 28593576.
- ↑ Nowinski RJ, Mehlman CT (1998). "Hyphenated history: Osgood-Schlatter disease". Am J. Orthopaedic. 27 (8): 584–5. PMID 9732084.
- ↑ Atanda A, Jr; Shah, SA; O'Brien, K (1 February 2011). "Osteochondrosis: common causes of pain in growing bones". American Family Physician. 83 (3): 285–91. PMID 21302869.
- 1 2 Çakmak, S., Tekin, L., & Akarsu, S. (2014). Long-term outcome of Osgood-Schlatter disease: not always favorable. Rheumatology International, 34(1), 135–136.
- 1 2 3 Nakase, J., Aiba, T., Goshima, K., Takahashi, R., Toratani, T., Kosaka, M., Ohashi, Y. & Tsuchiya, H. (2014). "Relationship between the skeletal maturation of the distal attachment of the patellar tendon and physical features in preadolescent male football players". Knee Surgery, Sports Traumatology, Arthroscopy. 22 (1): 195–199. doi:10.1007/s00167-012-2353-3. hdl:2297/36490. PMID 23263228.
{{cite journal}}: CS1 maint: uses authors parameter (link) - ↑ Smith, Benjamin (11 January 2018). "Incidence and prevalence of patellofemoral pain: A systematic review and meta-analysis". PLOS ONE. 13 (1): e0190892. doi:10.1371/journal.pone.0190892. PMC 5764329. PMID 29324820.
- ↑ Guttman, Jeffery (April 23, 1996). "Osgood-Schlatter Disease". The Alfred I. DuPont Institute. Archived from the original on 30 July 2017. Retrieved 22 February 2017.
- ↑ "OrthoKids - Osgood-Schlatter's Disease". Archived from the original on 2019-03-07. Retrieved 2018-09-13.
- ↑ Cassas KJ, Cassettari-Wayhs A (2006). "Childhood and adolescent sports-related overuse injuries". Am Fam Physician. 73 (6): 1014–22. PMID 16570735.
- ↑ Sinding-Larsen and Johansson syndrome at Who Named It?
- ↑ Lucena G. L., Gomes C. A., Guerro R. O. (2010). "Prevalence and Associated Factors of Osgood-Schlatter Syndrome in a Population-Based Sample of Brazilian Adolescents". The American Journal of Sports Medicine. 39: 415–420. doi:10.1177/0363546510383835.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - 1 2 Kabiri, L., Tapley, H., & Tapley, S. (2014). "Evaluation and conservative treatment for Osgood–Schlatter disease: A critical review of the literature". International Journal of Therapy & Rehabilitation. 21 (2): 91–96. doi:10.12968/ijtr.2014.21.2.91.
{{cite journal}}: CS1 maint: uses authors parameter (link) - 1 2 3 4 5 Gholve, PA; Scher, DM; Khakharia, S; Widmann, RF; Green, DW (February 2007). "Osgood Schlatter syndrome". Current Opinion in Pediatrics. 19 (1): 44–50. doi:10.1097/mop.0b013e328013dbea. PMID 17224661.
- ↑ Peck, DM (June 1995). "Apophyseal injuries in the young athlete". American Family Physician. 51 (8): 1891–5, 1897–8. PMID 7762480.
- ↑ Engel A, Windhager R (1987). "[Importance of the ossicle and therapy of Osgood-Schlatter disease]". Sportverletz Sportschaden (in German). 1 (2): 100–8. doi:10.1055/s-2007-993701. PMID 3508010.
{{cite journal}}: CS1 maint: unrecognized language (link) - 1 2 Gholve PA, Scher DM, Khakharia S, Widmann RF, Green DW (2007). "Osgood Schlatter syndrome". Curr. Opin. Pediatr. 19 (1): 44–50. doi:10.1097/MOP.0b013e328013dbea. PMID 17224661.
- ↑ O. Josh Bloom; Leslie Mackler (February 2004). "What is the best treatment for Osgood-Schlatter disease?" (PDF). Journal of Family Practice. 53 (2). Archived (PDF) from the original on 2014-10-06.
- 1 2 Baltaci H., Ozer V., Tunay B. (2004). "Rehabilitation of avulsion fracture of the tibial tuberosity". Knee Surgery, Sports Traumatology, Arthroscopy. 12: 115–118. doi:10.1007/s00167-003-0383-6.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Kujala UM, Kvist M, Heinonen O (1985). "Osgood-Schlatter's disease in adolescent athletes. Retrospective study of incidence and duration". Am J Sports Med. 13 (4): 236–41. doi:10.1177/036354658501300404. PMID 4025675.
- ↑ Bloom J (2004). "What is the best treatment for Osgood-Schlatter disease?". Journal of Family Practice. 53 (2): 153–156.
- ↑ Yashar A, Loder RT, Hensinger RN (1995). "Determination of skeletal age in children with Osgood-Schlatter disease by using radiographs of the knee". J Pediatr Orthop. 15 (3): 298–301. doi:10.1097/01241398-199505000-00006. PMID 7790482.
- ↑ Vreju F, Ciurea P, Rosu A (December 2010). "Osgood-Schlatter disease—ultrasonographic diagnostic". Med Ultrason. 12 (4): 336–9. PMID 21210020. Archived from the original on 2019-12-18. Retrieved 2013-06-27.
External links
| Classification | |
|---|---|
| External resources |