Benzbromarone
Benzbromarone is a uricosuric agent and non-competitive inhibitor of xanthine oxidase[1] used in the treatment of gout, especially when allopurinol, a first-line treatment, fails or produces intolerable adverse effects. It is structurally related to the antiarrhythmic amiodarone.[2]
 | |
| Clinical data | |
|---|---|
| AHFS/Drugs.com | International Drug Names |
| ATC code | |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| ChemSpider | |
| UNII | |
| ChEBI | |
| ChEMBL | |
| CompTox Dashboard (EPA) | |
| ECHA InfoCard | 100.020.573 |
| Chemical and physical data | |
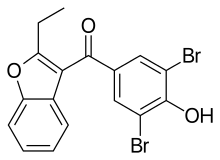
| Formula | C17H12Br2O3 |
| Molar mass | 424.088 g·mol−1 |
| 3D model (JSmol) | |
| Melting point | 161 to 163 °C (322 to 325 °F) |
| |
| |
| | |
Benzbromarone is highly effective and well tolerated,[3][4][5][6] and clinical trials as early as 1981 and as recently as April 2008 have suggested it is superior to both allopurinol, a non-uricosuric xanthine oxidase inhibitor, and probenecid, another uricosuric drug.[7][8]
Mechanism of action
Benzbromarone is a very potent inhibitor of CYP2C9.[2][9] Several analogues of the drug have been developed as CYP2C9 and CYP2C19 inhibitors for use in research.[10][11]
History
Benzbromarone was introduced in the 1970s and was viewed as having few associated serious adverse reactions. It was registered in about 20 countries throughout Europe, Asia and South America.
In 2003, the drug was withdrawn by Sanofi-Synthélabo, after reports of serious hepatotoxicity, although it is still marketed in several countries by other drug companies.[12]
References
- Sinclair DS, Fox IH (December 1975). "The pharmacology of hypouricemic effect of benzbromarone". The Journal of Rheumatology. 2 (4): 437–45. PMID 1206675.
- Kumar V, Locuson CW, Sham YY, Tracy TS (October 2006). "Amiodarone analog-dependent effects on CYP2C9-mediated metabolism and kinetic profiles". Drug Metabolism and Disposition. 34 (10): 1688–96. doi:10.1124/dmd.106.010678. PMID 16815961.
- Heel RC, Brogden RN, Speight TM, Avery GS (November 1977). "Benzbromarone: a review of its pharmacological properties and therapeutic use in gout and hyperuricaemia". Drugs. 14 (5): 349–66. doi:10.2165/00003495-197714050-00002. PMID 338280. S2CID 8198915.
- Masbernard A, Giudicelli CP (May 1981). "Ten years' experience with benzbromarone in the management of gout and hyperuricaemia" (PDF). South African Medical Journal = Suid-Afrikaanse Tydskrif vir Geneeskunde. 59 (20): 701–6. PMID 7221794.
- Perez-Ruiz F, Alonso-Ruiz A, Calabozo M, Herrero-Beites A, García-Erauskin G, Ruiz-Lucea E (September 1998). "Efficacy of allopurinol and benzbromarone for the control of hyperuricaemia. A pathogenic approach to the treatment of primary chronic gout". Annals of the Rheumatic Diseases. 57 (9): 545–9. doi:10.1136/ard.57.9.545. PMC 1752740. PMID 9849314.
- Reinders MK, van Roon EN, Houtman PM, Brouwers JR, Jansen TL (September 2007). "Biochemical effectiveness of allopurinol and allopurinol-probenecid in previously benzbromarone-treated gout patients". Clinical Rheumatology. 26 (9): 1459–65. doi:10.1007/s10067-006-0528-3. PMID 17308859.
- Schepers GW (1981). "Benzbromarone therapy in hyperuricaemia; comparison with allopurinol and probenecid". The Journal of International Medical Research. 9 (6): 511–5. doi:10.1177/030006058100900615. PMID 7033016. S2CID 33337546.
- Reinders MK, van Roon EN, Jansen TL, Delsing J, Griep EN, Hoekstra M, et al. (January 2009). "Efficacy and tolerability of urate-lowering drugs in gout: a randomised controlled trial of benzbromarone versus probenecid after failure of allopurinol". Annals of the Rheumatic Diseases. 68 (1): 51–6. doi:10.1136/ard.2007.083071. PMID 18250112.
- Hummel MA, Locuson CW, Gannett PM, Rock DA, Mosher CM, Rettie AE, Tracy TS (September 2005). "CYP2C9 genotype-dependent effects on in vitro drug-drug interactions: switching of benzbromarone effect from inhibition to activation in the CYP2C9.3 variant". Molecular Pharmacology. 68 (3): 644–51. doi:10.1124/mol.105.013763. PMC 1552103. PMID 15955872.
- Locuson CW, Rock DA, Jones JP (June 2004). "Quantitative binding models for CYP2C9 based on benzbromarone analogues". Biochemistry. 43 (22): 6948–58. CiteSeerX 10.1.1.127.2015. doi:10.1021/bi049651o. PMID 15170332.
- Locuson CW, Suzuki H, Rettie AE, Jones JP (December 2004). "Charge and substituent effects on affinity and metabolism of benzbromarone-based CYP2C19 inhibitors". Journal of Medicinal Chemistry. 47 (27): 6768–76. doi:10.1021/jm049605m. PMID 15615526.
- Lee MH, Graham GG, Williams KM, Day RO (2008). "A benefit-risk assessment of benzbromarone in the treatment of gout. Was its withdrawal from the market in the best interest of patients?". Drug Safety. 31 (8): 643–65. doi:10.2165/00002018-200831080-00002. PMID 18636784. S2CID 1204662.