Bronchiolitis
Bronchiolitis is inflammation of the small airways in the lungs. Acute bronchiolitis is due to a viral infection usually affecting children younger than two years of age.[5] Symptoms may include fever, cough, runny nose, wheezing, and breathing problems.[1] More severe cases may be associated with nasal flaring, grunting, or the skin between the ribs pulling in with breathing.[1] If the child has not been able to feed properly, signs of dehydration may be present.[1]
| Bronchiolitis | |
|---|---|
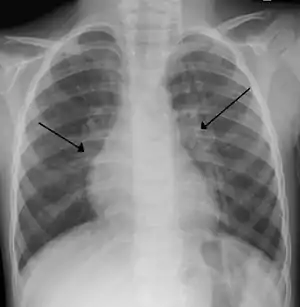 | |
| An X-ray of a child with RSV showing the typical bilateral perihilar fullness of bronchiolitis. | |
| Specialty | Emergency medicine, pediatrics |
| Symptoms | Fever, cough, runny nose, wheezing, breathing problems[1] |
| Complications | Shortness of breath, dehydration[1] |
| Usual onset | Less than 2 years old[2] |
| Causes | Viral disease (respiratory syncytial virus, human rhinovirus)[2] |
| Diagnostic method | Based on symptoms[1] |
| Differential diagnosis | Asthma, pneumonia, heart failure, allergic reaction, cystic fibrosis[1] |
| Treatment | Symptomatic treatment (oxygen, support with feeding, intravenous fluids)[3] |
| Frequency | ~20% (children less than 2)[2][1] |
| Deaths | 1% (among those hospitalized)[4] |
Chronic bronchiolitis is the general term used for small airways disease in adults, notably in chronic obstructive pulmonary disease.[5][6]
Acute bronchiolitis is usually the result of infection by respiratory syncytial virus (72% of cases) or human rhinovirus (26% of cases).[2] Diagnosis is generally based on symptoms.[1] Tests such as a chest X-ray or viral testing are not routinely needed.[2]
There is no specific treatment.[3][7] Symptomatic treatment at home is generally sufficient.[1] Occasionally, hospital admission for oxygen, support with feeding, or intravenous fluids is required.[1] Tentative evidence supports nebulized hypertonic saline.[8] Evidence for antibiotics, antivirals, bronchodilators, or nebulized epinephrine is either unclear or not supportive.[9]
About 10% to 30% of children under the age of two years are affected by bronchiolitis at some point in time.[1][2] It commonly occurs in the winter in the Northern Hemisphere.[1] It is the leading cause of hospitalizations in those less than one year of age in the United States.[10][7] The risk of death among those who are admitted to hospital is about 1%.[4] Outbreaks of the condition were first described in the 1940s.[11]
Signs and symptoms
Bronchiolitis typically presents in children under two years old and is characterized by a constellation of respiratory symptoms that consists of fever, rhinorrhea, cough, wheeze, tachypnea and increased work of breathing such as nasal flaring or grunting that develops over one to three days.[10] Crackles or wheeze are typical findings on listening to the chest with a stethoscope. The child may also experience apnea, or brief pauses in breathing. After the acute illness, it is common for the airways to remain sensitive for several weeks, leading to recurrent cough and wheeze.
Some signs of severe disease include:[12]
- increased work of breathing (such as use of accessory muscles of respiration, rib & sternal retraction, tracheal tug)
- severe chest wall recession (Hoover's sign)
- presence of nasal flaring and/or grunting
- increased respiratory rate above normal
- hypoxia (low oxygen levels)
- cyanosis (bluish skin)
- lethargy and decreased activity
- poor feeding (less than half of usual fluid intake in preceding 24 hours)
- history of stopping breathing
Causes
.jpg.webp)
The term usually refers to acute viral bronchiolitis, a common disease in infancy. This is most commonly caused by respiratory syncytial virus[13] (RSV, also known as human pneumovirus). Other agents that cause this illness include human metapneumovirus, influenza, parainfluenza, coronavirus, adenovirus, rhinovirus and mycoplasma.[14][15]
Risk factors
Children are at an increased risk for progression to severe respiratory disease if they have any of the following additional factors:[7][10][15][16]
- Preterm infant (gestational age less than 37 weeks)
- Younger age at onset of illness (less than 3 months of age)
- Congenital heart disease
- Immunodeficiency
- Chronic lung disease
- Neurological disorders
- Tobacco smoke exposure
Diagnosis
The diagnosis is typically made by clinical examination. Chest X-ray is sometimes useful to exclude bacterial pneumonia, but not indicated in routine cases.[17] Chest x-ray may also be useful in people with impending respiratory failure.[18] Additional testing such as blood cultures, complete blood count, and electrolyte analyses are not recommended for routine use although may be useful in children with multiple comorbidities or signs of sepsis or pneumonia.[7][18]
Testing for the specific viral cause can be done but has little effect on management and thus is not routinely recommended.[17] RSV testing by direct immunofluorescence testing on nasopharyngeal aspirate had a sensitivity of 61% and specificity of 89%.[15][18] Identification of those who are RSV-positive can help for disease surveillance, grouping ("cohorting") people together in hospital wards to prevent cross infection, predicting whether the disease course has peaked yet, and reducing the need for other diagnostic procedures (by providing confidence that a cause has been identified).[7] Identification of the virus may help reduce the use of antibiotics.[18]
Infants with bronchiolitis between the age of two and three months have a second infection by bacteria (usually a urinary tract infection) less than 6% of the time.[19] When further evaluated with a urinalysis, infants with bronchiolitis had a concomitant UTI 0.8% of the time.[20] Preliminary studies have suggested that elevated procalcitonin levels may assist clinicians in determining the presence of bacterial co-infection, which could prevent unnecessary antibiotic use and costs.[21]
Differential diagnosis
There are many childhood illnesses that can present with respiratory symptoms, particularly persistent cough and wheezing.[10][22] Bronchiolitis may be differentiated from some of these by the characteristic pattern of preceding febrile upper respiratory tract symptoms lasting for 1 to 3 days followed by the persistent cough, tachypnea, and wheezing.[22] However, some infants may present without fever (30% of cases) or may present with apnea without other signs or with poor weight gain prior to onset of symptoms.[22] In such cases, additional laboratory testing and radiographic imaging may be useful.[10][22] The following are some other diagnoses to consider in an infant presenting with signs of bronchiolitis:
Prevention
Prevention of bronchiolitis relies strongly on measures to reduce the spread of the viruses that cause respiratory infections (that is, handwashing, and avoiding exposure to those symptomatic with respiratory infections).[7][10] Guidelines are mixed on the use of gloves, aprons, or personal protective equipment.[7] In addition to good hygiene, an improved immune system is a great tool for prevention.
One way to improve the immune system is to feed the infant with breast milk, especially during the first month of life.[16][23] Respiratory infections were shown to be significantly less common among breastfed infants and fully breastfed RSV-positive hospitalized infants had shorter hospital stays than non or partially breastfed infants.[10] Guidelines recommend exclusive breastfeeding for infants for the first 6 months of life.[10]
Palivizumab, a monoclonal antibody against RSV, can be administered to prevent bronchiolitis to infants less than one year of age that were born very prematurely or that have underlying heart disease or chronic lung disease of prematurity.[10] Passive immunization therapy requires monthly injections during winter.[10] Otherwise healthy premature infants that were born after a gestational age of 29 weeks should not be administered palivizumab as the harms outweigh the benefits.[10] Passive protection through the administration of other novel monoclonal antibodies is also under evaluation.[18]
Immunizations for RSV are being developed but none are available currently outside of clinical trials.[18][24]
Tobacco smoke exposure has been shown to increase both the rates of lower respiratory disease in infants, as well as the risk and severity of bronchiolitis.[10] Tobacco smoke lingers in the environment for prolonged periods and on clothing even when smoking outside the home.[10] Guidelines recommend that parents be fully educated on the risks of tobacco smoke exposure on children with bronchiolitis.[10][22]
Management
Treatment of bronchiolitis is usually focused on the hydration and symptoms instead of the infection itself since the infection will run its course and complications are typically from the symptoms themselves.[25] Without active treatment, half of cases will go away in 13 days and 90% in three weeks.[26] Children with severe symptoms, especially poor feeding or dehydration, may be considered for hospital admission.[7] Oxygen saturation under 90%-92% as measured with pulse oximetry is also frequently used as an indicator of need for hospitalization.[7] High-risk infants, apnea, cyanosis, malnutrition, and diagnostic uncertainty are additional indications for hospitalization.[7]
Most guidelines recommend sufficient fluids and nutritional support for affected children.[7] Measures for which the recommendations were mixed include nebulized hypertonic saline, nebulized epinephrine, and nasal suctioning.[1][7][27][28] Treatments which the evidence does not support include salbutamol, steroids, antibiotics, antivirals, heliox, continuous positive airway pressure (CPAP), chest physiotherapy, and cool mist or steam inhalation.[1][29][30][31][32]
Diet
Maintaining hydration is an important part of management of bronchiolitis.[10][18][33] Infants with mild pulmonary symptoms may require only observation if feeding is unaffected.[10] However, oral intake may be affected by nasal secretions and increased work of breathing.[10] Poor feeding or dehydration, defined as less than 50% of usual intake, is often cited as an indication for hospital admission.[7] Guidelines recommend the use of nasogastric or intravenous fluids in children with bronchiolitis who cannot maintain usual oral intake.[10][22][18] The risk of health care caused hyponatremia and fluid retention are minimal with the use of isotonic fluids such as normal saline, breast milk, or formula.[10]
Oxygen

Inadequate oxygen supply to the tissue is one of the main concerns during severe bronchiolitis and oxygen saturation is often closely associated with both the need for hospitalization and continued length of hospital stay in children with bronchiolitis.[18] However, oxygen saturation is a poor predictor of respiratory distress.[10] Accuracy of pulse oximetry is limited in the 76% to 90% range and there is weak correlation between oxygen saturation and respiratory distress as brief hypoxemia is common in healthy infants.[10][18] Additionally, pulse oximetry is associated with frequent false alarms and parental stress and fatigue.[10] Clinicians may choose not to given additional oxygen to children with bronchiolitis if their oxygen saturation is above 90%.[10][22][18] Additionally, clinicians may choose not to use continuous pulse oximetry in these people.[10]
When choosing to use oxygen therapy for a child with bronchiolitis, there is evidence that home oxygen may reduce hospitalization rate and length of stay although readmission rates and follow-up visits are increased.[10] Also, the use of humidified, heated, high-flow nasal cannula may be a safe initial therapy to decrease work of breathing and need for intubation.[10][34] However, evidence is lacking regarding the use of high-flow nasal cannula compared to standard oxygen therapy or continuous positive airway pressure.[18][34][35] These practices may still be used in severe cases prior to intubation.[22][36][37]
Blood gas testing is not recommended for people hospitalized with the disease and is not useful in the routine management of bronchiolitis.[18][22] People with severe worsening respiratory distress or impending respiratory failure may be considered for capillary blood gas testing.[22]
Hypertonic saline
Guidelines recommend against the use of nebulized hypertonic saline in the emergency department for children with bronchiolitis but it may be given to children who are hospitalized.[10][18]
Nebulized hypertonic saline (3%) has limited evidence of benefit and previous studies lack consistency and standardization.[8][9][38][39] A 2017 review found tentative evidence that it reduces the risk of hospitalization, duration of hospital stay, and improved the severity of symptoms.[8][40] The majority of evidence suggests that hypertonic saline is safe and effective at improving respiratory symptoms of mild to moderate bronchiolitis after 24 hours of use.[41] However, it does not appear effective in reducing the rate of hospitalization when used in the emergency room or other outpatient settings in which length of therapy is brief.[10] Side effects were mild and resolved spontaneously.[8]
Bronchodilators
Guidelines recommend against the use of bronchodilators in children with bronchiolitis as evidence does not support a change in outcomes with such use.[10][22][42][43] Additionally, there are adverse effects to the use of bronchodilators in children such as tachycardia and tremors, as well as adding increased financial expenses.[44][45]
Several studies have shown that bronchodilation with β-adrenergic agents such as salbutamol may improve symptoms briefly but do not affect the overall course of the illness or reduce the need for hospitalization.[10] However, there are conflicting recommendations about the use of a trial of a bronchodilator, especially in those with history of previous wheezing, due to the difficulty with assessing an objective improvement in symptoms.[7][10][18] Bronchiolitis-associated wheezing is likely not effectively alleviated by bronchodilators anyway as it is caused by airway obstruction and plugging of the small airway diameters by luminal debris, not bronchospasm as in asthma-associated wheezing that bronchodilators usually treat well.[45]
Anticholinergic inhalers, such as ipratropium bromide, have a modest short-term effect at best and are not recommended for treatment.[22][46][47]
Epinephrine
The current state of evidence suggests that nebulized epinephrine is not indicated for children with bronchiolitis except as a trial of rescue therapy for severe cases.[10][22]
Epinephrine is an α and β adrenergic agonist that has been used to treat other upper respiratory tract illnesses, such as croup, as a nebulized solution.[48] A Cochrane meta-analysis in 2011 found no benefit to the use of epinephrine in the inpatient setting and suggested that there may be utility in the outpatient setting in reducing the rate of hospitalization.[49][28] However, current guidelines do not support the outpatient use of epinephrine given the lack of substantial sustained benefit.[10]
A 2017 review found inhaled epinephrine with corticosteroids did not change the need for hospitalization or the time spent in hospital.[50] Other studies suggest a synergistic effect of epinephrine with corticosteroids but have not consistently demonstrated benefits in clinical trials.[10] Guidelines recommend against its use currently.[10][7]
Unclear evidence
Currently other medications do not yet have evidence to support their use, although they have been studied for use in bronchiolitis.[10][51] Experimental trials with novel antiviral medications in adults are promising but it remains unclear if the same benefit will be present.[18]
- Surfactant had favorable effects for severely critical infants on duration of mechanical ventilation and ICU stay however studies were few and small.[52][14]
- Chest physiotherapy, such as vibration or percussion, to promote airway clearance may slightly reduce duration of oxygen therapy but there is a lack of evidence that demonstrates any other benefits.[10][53] People with difficulty clearing secretions due to underlying disorders such as spinal muscle atrophy or severe tracheomalacia may be considered for chest physiotherapy.[22]
- Suctioning of the nares may provide temporarily relief of nasal congestion but deep suctioning of the nasopharynx has been shown prolong length of hospital stay in infants.[10][22] Upper airway suctioning may be considered in people with respiratory distress, feeding difficulties, or infants presenting with apnea.[22]
- Heliox, a mixture of oxygen and the inert gas helium, may be beneficial in infants with severe acute RSV bronchiolitis who require CPAP but overall evidence is lacking.[54]
- DNAse has not been found to be effective but might play a role in severe bronchiolitis complicated by atelectasis.[55]
- There are no systematic reviews or controlled trials on the effectiveness of nasal decongestants, such as xylometazoline, for the treatment of bronchiolitits.[14]
- Overall evidence is insufficient to support the use of alternative medicine.[56] There is tentative evidence for Chinese herbal medicine, vitamin D, N-acetylcysteine, and magnesium but this is insufficient to recommend their use.[56]
Non-effective treatments
- Ribavirin is an antiviral drug which does not appear to be effective for bronchiolitis.[57]
- Antibiotics are often given in case of a bacterial infection complicating bronchiolitis, but have no effect on the underlying viral infection and their benefit is not clear.[57][58][59][60] The risks of bronchiolitis with a concomitant serious bacterial infection among hospitalized febrile infants is minimal and work-up and antibiotics are not justified.[10][20] Azithromycin adjuvant therapy may reduce the duration of wheezing and coughing in children with bronchiolitis but has not effect on length of hospital stay or duration of oxygen therapy.[61]
- Corticosteroids, although useful in other respiratory disease such as asthma and croup, have no proven benefit in bronchiolitis treatment and are not advised.[10][7][57][62][63] Additionally, corticosteroid therapy in children with bronchiolitis may prolong viral shedding and transmissibility.[10] The overall safety of corticosteroids is questionable.[64]
- Leukotriene inhibitors, such as montelukast, have not been found to be beneficial and may increase adverse effects.[7][65][66][67]
- Immunoglobulins are of unclear benefit.[68]
Epidemiology
Bronchiolitis typically affects infants and children younger than two years, principally during the autumn and winter.[18] It is the leading cause of hospital admission for respiratory disease among infants in the United States and accounts for one out of every 13 primary care visits.[7] Bronchiolitis accounts for 3% of emergency department visits for children under 2 years old.[14] Bronchiolitis is the most frequent lower respiratory tract infection and hospitalization in infants worldwide.[18]
References
- Friedman JN, Rieder MJ, Walton JM, Canadian Paediatric Society, Acute Care Committee, Drug Therapy and Hazardous Substances (November 2014). "Bronchiolitis: Recommendations for diagnosis, monitoring and management of children one to 24 months of age". Paediatrics & Child Health. 19 (9): 485–98. doi:10.1093/pch/19.9.485. PMC 4235450. PMID 25414585.
- Schroeder, AR; Mansbach, JM (June 2014). "Recent evidence on the management of bronchiolitis". Current Opinion in Pediatrics. 26 (3): 328–33. doi:10.1097/MOP.0000000000000090. PMC 4552182. PMID 24739493.
- Hancock, DG; Charles-Britton, B; Dixon, DL; Forsyth, KD (September 2017). "The heterogeneity of viral bronchiolitis: A lack of universal consensus definitions". Pediatric Pulmonology. 52 (9): 1234–1240. doi:10.1002/ppul.23750. PMID 28672069. S2CID 3454691.
- Kendig, Edwin L.; Wilmott, Robert W.; Boat, Thomas F.; Bush, Andrew; Chernick, Victor (2012). Kendig and Chernick's Disorders of the Respiratory Tract in Children. Elsevier Health Sciences. p. 450. ISBN 978-1437719840.
- Ryu, JH; Azadeh, N; Samhouri, B; Yi, E (2020). "Recent advances in the understanding of bronchiolitis in adults". F1000Research. 9: 568. doi:10.12688/f1000research.21778.1. PMC 7281671. PMID 32551095.
- Kumar, Vinay; Abbas, Abul K.; Aster, Jon C. (2018). Robbins basic pathology (Tenth ed.). Philadelphia, Pennsylvania. p. 502. ISBN 9780323353175.
- Kirolos, Amir; Manti, Sara; Blacow, Rachel; Tse, Gabriel; Wilson, Thomas; Lister, Martin; Cunningham, Steve; Campbell, Alasdair; Nair, Harish; Reeves, Rachel M.; Fernandes, Ricardo M. (2019). "A Systematic Review of Clinical Practice Guidelines for the Diagnosis and Management of Bronchiolitis". The Journal of Infectious Diseases. 222 (Supplement_7): S672–S679. doi:10.1093/infdis/jiz240. hdl:20.500.11820/7d4708e3-7cdc-49f7-a9b3-a29040f4ff4e. PMID 31541233.
- Zhang, L; Mendoza-Sassi, RA; Wainwright, C; Klassen, TP (21 December 2017). "Nebulised hypertonic saline solution for acute bronchiolitis in infants". The Cochrane Database of Systematic Reviews. 2017 (12): CD006458. doi:10.1002/14651858.CD006458.pub4. PMC 6485976. PMID 29265171.
- Brooks, CG; Harrison, WN; Ralston, SL (18 April 2016). "Association Between Hypertonic Saline and Hospital Length of Stay in Acute Viral Bronchiolitis: A Reanalysis of 2 Meta-analyses". JAMA Pediatrics. 170 (6): 577–84. doi:10.1001/jamapediatrics.2016.0079. PMID 27088767.
- Ralston, Shawn L.; Lieberthal, Allan S.; Meissner, H. Cody; Alverson, Brian K.; Baley, Jill E.; Gadomski, Anne M.; Johnson, David W.; Light, Michael J.; Maraqa, Nizar F.; Mendonca, Eneida A.; Phelan, Kieran J. (1 November 2014). "Clinical Practice Guideline: The Diagnosis, Management, and Prevention of Bronchiolitis". Pediatrics. 134 (5): e1474–e1502. doi:10.1542/peds.2014-2742. ISSN 0031-4005. PMID 25349312.
- Anderson, Larry J.; Graham, Barney S. (2013). Challenges and Opportunities for Respiratory Syncytial Virus Vaccines. Current Topics in Microbiology and Immunology. Vol. 372. Springer Science & Business Media. p. 392. doi:10.1007/978-3-642-38919-1_20. ISBN 9783642389191. PMC 7121045. PMID 24362701.
- BRONCHIOLITIS IN CHILDREN (Sign Guideline 91). Scottish Intercollegiate Guidelines Network. 2006. ISBN 9781905813018. Archived from the original on 1 November 2012. Retrieved 6 December 2012.
- Smyth RL, Openshaw PJ (July 2006). "Bronchiolitis". Lancet. 368 (9532): 312–22. doi:10.1016/S0140-6736(06)69077-6. PMID 16860701. S2CID 208791826.
- Bourke, Thomas; Shields, Michael (11 April 2011). "Bronchiolitis". BMJ Clinical Evidence. 2011. ISSN 1752-8526. PMC 3275170. PMID 21486501.
- Bordley, W. Clayton; Viswanathan, Meera; King, Valerie J.; Sutton, Sonya F.; Jackman, Anne M.; Sterling, Laura; Lohr, Kathleen N. (1 February 2004). "Diagnosis and Testing in Bronchiolitis: A Systematic Review". Archives of Pediatrics & Adolescent Medicine. 158 (2): 119–126. doi:10.1001/archpedi.158.2.119. ISSN 1072-4710. PMID 14757603.
- Carbonell-Estrany X, Figueras-Aloy J (2004). "Identifying risk factors for severe respiratory syncytial virus among infants born after 33 through 35 completed weeks of gestation: different methodologies yield consistent findings". Pediatr Infect Dis J. 23 (11 Suppl): S193–201. doi:10.1097/01.inf.0000144664.31888.53. PMID 15577573. S2CID 39990266.
- Zorc, JJ; Hall, CB (February 2010). "Bronchiolitis: recent evidence on diagnosis and management". Pediatrics. 125 (2): 342–9. doi:10.1542/peds.2009-2092. PMID 20100768. S2CID 4932917.
- Caballero, Mauricio T.; Polack, Fernando P.; Stein, Renato T. (1 November 2017). "Viral bronchiolitis in young infants: new perspectives for management and treatment". Jornal de Pediatria. 93: 75–83. doi:10.1016/j.jped.2017.07.003. ISSN 0021-7557. PMID 28859915.
- Ralston, S; Hill, V; Waters, A (October 2011). "Occult serious bacterial infection in infants younger than 60 to 90 days with bronchiolitis: a systematic review". Archives of Pediatrics & Adolescent Medicine. 165 (10): 951–6. doi:10.1001/archpediatrics.2011.155. PMID 21969396.
- McDaniel, Corrie E.; Ralston, Shawn; Lucas, Brian; Schroeder, Alan R. (1 March 2019). "Association of Diagnostic Criteria With Urinary Tract Infection Prevalence in Bronchiolitis: A Systematic Review and Meta-analysis". JAMA Pediatrics. 173 (3): 269–277. doi:10.1001/jamapediatrics.2018.5091. ISSN 2168-6211. PMC 6439888. PMID 30688987.
- Laham, James L.; Breheny, Patrick J.; Gardner, Brian M.; Bada, Henrietta (2014). "Procalcitonin to Predict Bacterial Coinfection in Infants With Acute Bronchiolitis". Pediatric Emergency Care. 30 (1): 11–15. doi:10.1097/PEC.0000000000000026. PMID 24365727. S2CID 11141711.
- "1 Recommendations | Bronchiolitis in children: diagnosis and management | Guidance | NICE". www.nice.org.uk. Retrieved 31 October 2019.
- Belderbos ME, Houben ML, van Bleek GM, et al. (February 2012). "Breastfeeding modulates neonatal innate immune responses: a prospective birth cohort study". Pediatric Allergy and Immunology. 23 (1): 65–74. doi:10.1111/j.1399-3038.2011.01230.x. PMID 22103307. S2CID 7605378.
- CDC (29 October 2019). "Protect Against RSV". Centers for Disease Control and Prevention. Retrieved 2 November 2019.
- Wright, M; Mullett CJ; Piedimonte G; et al. (October 2008). "Pharmacological management of acute bronchiolitis". Therapeutics and Clinical Risk Management. 4 (5): 895–903. doi:10.2147/tcrm.s1556. PMC 2621418. PMID 19209271.
- Thompson, M; Vodicka, TA; Blair, PS; Buckley, DI; Heneghan, C; Hay, AD; TARGET Programme, Team (11 December 2013). "Duration of symptoms of respiratory tract infections in children: systematic review". BMJ (Clinical Research Ed.). 347: f7027. doi:10.1136/bmj.f7027. PMC 3898587. PMID 24335668.
- Liet, Jean-Michel; Ducruet, Thierry; Gupta, Vineet; Cambonie, Gilles (18 September 2015). "Heliox inhalation therapy for bronchiolitis in infants". Cochrane Database of Systematic Reviews. 2015 (9): CD006915. doi:10.1002/14651858.CD006915.pub3. PMC 8504435. PMID 26384333.
- Hartling, Lisa; Bialy, Liza M.; Vandermeer, Ben; Tjosvold, Lisa; Johnson, David W.; Plint, Amy C.; Klassen, Terry P.; Patel, Hema; Fernandes, Ricardo M. (15 June 2011). "Epinephrine for bronchiolitis". The Cochrane Database of Systematic Reviews (6): CD003123. doi:10.1002/14651858.CD003123.pub3. ISSN 1469-493X. PMID 21678340.
- Fernandes, Ricardo M; Bialy, Liza M; Vandermeer, Ben; Tjosvold, Lisa; Plint, Amy C; Patel, Hema; Johnson, David W; Klassen, Terry P; Hartling, Lisa (4 June 2013). "Glucocorticoids for acute viral bronchiolitis in infants and young children". Cochrane Database of Systematic Reviews (6): CD004878. doi:10.1002/14651858.CD004878.pub4. PMC 6956441. PMID 23733383.
- Roqué i Figuls, Marta; Giné-Garriga, Maria; Granados Rugeles, Claudia; Perrotta, Carla; Vilaró, Jordi (1 February 2016). "Chest physiotherapy for acute bronchiolitis in paediatric patients between 0 and 24 months old". Cochrane Database of Systematic Reviews. 2 (7): CD004873. doi:10.1002/14651858.CD004873.pub5. PMC 6458017. PMID 26833493.
- Jat, Kana R.; Dsouza, Jeanne M.; Mathew, Joseph L. (4 April 2022). "Continuous positive airway pressure (CPAP) for acute bronchiolitis in children". The Cochrane Database of Systematic Reviews. 2022 (4): CD010473. doi:10.1002/14651858.CD010473.pub4. ISSN 1469-493X. PMC 8978604. PMID 35377462.
- Umoren, Rachel; Odey, Friday; Meremikwu, Martin M (19 January 2011). "Steam inhalation or humidified oxygen for acute bronchiolitis in children up to three years of age". Cochrane Database of Systematic Reviews (1): CD006435. doi:10.1002/14651858.CD006435.pub2. PMID 21249676.
- Kua, Kok Pim; Lee, Shaun Wen Huey (2017). "Complementary and alternative medicine for the treatment of bronchiolitis in infants: A systematic review". PLOS ONE. 12 (2): e0172289. Bibcode:2017PLoSO..1272289K. doi:10.1371/journal.pone.0172289. ISSN 1932-6203. PMC 5315308. PMID 28212381.
- Lin, Jilei; Zhang, Yin; Xiong, Limei; Liu, Sha; Gong, Caihui; Dai, Jihong (June 2019). "High-flow nasal cannula therapy for children with bronchiolitis: a systematic review and meta-analysis". Archives of Disease in Childhood. 104 (6): 564–576. doi:10.1136/archdischild-2018-315846. ISSN 1468-2044. PMID 30655267. S2CID 58666508.
- Beggs, Sean; Wong, Zee Hame; Kaul, Sheena; Ogden, Kathryn J; Walters, Julia AE (20 January 2014). "High-flow nasal cannula therapy for infants with bronchiolitis". Cochrane Database of Systematic Reviews (1): 1–26. doi:10.1002/14651858.CD009609.pub2. PMID 24442856.
- Combret, Yann; Prieur, Guillaume; LE Roux, Pascal; Médrinal, Clément (June 2017). "Non-invasive ventilation improves respiratory distress in children with acute viral bronchiolitis: a systematic review". Minerva Anestesiologica. 83 (6): 624–637. doi:10.23736/S0375-9393.17.11708-6. ISSN 1827-1596. PMID 28192893.
- Jat, Kana R.; Mathew, Joseph L. (31 January 2019). "Continuous positive airway pressure (CPAP) for acute bronchiolitis in children". The Cochrane Database of Systematic Reviews. 1: CD010473. doi:10.1002/14651858.CD010473.pub3. ISSN 1469-493X. PMC 6354031. PMID 30701528.
- Zhang, L; Mendoza-Sassi, RA; Klassen, TP; Wainwright, C (October 2015). "Nebulized Hypertonic Saline for Acute Bronchiolitis: A Systematic Review". Pediatrics. 136 (4): 687–701. doi:10.1542/peds.2015-1914. PMID 26416925.
- Brooks, Corinne G.; Harrison, Wade N.; Ralston, Shawn L. (1 June 2016). "Association Between Hypertonic Saline and Hospital Length of Stay in Acute Viral Bronchiolitis: A Reanalysis of 2 Meta-analyses". JAMA Pediatrics. 170 (6): 577–584. doi:10.1001/jamapediatrics.2016.0079. ISSN 2168-6211. PMID 27088767.
- Zhang, Linjie; Gunther, Carlos B.; Franco, Ozeia S.; Klassen, Terry P. (August 2018). "Impact of hypertonic saline on hospitalization rate in infants with acute bronchiolitis: A meta-analysis". Pediatric Pulmonology. 53 (8): 1089–1095. doi:10.1002/ppul.24066. ISSN 1099-0496. PMID 29893029. S2CID 48358175.
- Zhang, Linjie; Mendoza-Sassi, Raúl A.; Wainwright, Claire; Klassen, Terry P. (21 December 2017). "Nebulised hypertonic saline solution for acute bronchiolitis in infants". The Cochrane Database of Systematic Reviews. 2017 (12): CD006458. doi:10.1002/14651858.CD006458.pub4. ISSN 1469-493X. PMC 6485976. PMID 29265171.
- Gadomski, Anne M; Scribani, Melissa B (17 June 2014). "Bronchodilators for bronchiolitis". Cochrane Database of Systematic Reviews (6): CD001266. doi:10.1002/14651858.CD001266.pub4. PMC 7055016. PMID 24937099.
- "Bronchiolitis - Clinical Practice Guideline". www.aafp.org. Archived from the original on 23 October 2019. Retrieved 23 October 2019.
- Chavasse, Richard JPG; Seddon, Paul; Bara, Anna; McKean, Michael C. (2002). "Short acting beta2‐agonists for recurrent wheeze in children under two years of age". Cochrane Database of Systematic Reviews. 2010 (2): CD002873. doi:10.1002/14651858.CD002873. ISSN 1465-1858. PMC 8456461. PMID 12137663.
- Gadomski, Anne M.; Scribani, Melissa B. (17 June 2014). "Bronchodilators for bronchiolitis". The Cochrane Database of Systematic Reviews (6): CD001266. doi:10.1002/14651858.CD001266.pub4. ISSN 1469-493X. PMC 7055016. PMID 24937099.
- Kellner, J. D.; Ohlsson, A.; Gadomski, A. M.; Wang, E. E. (November 1996). "Efficacy of bronchodilator therapy in bronchiolitis. A meta-analysis". Archives of Pediatrics & Adolescent Medicine. 150 (11): 1166–1172. doi:10.1001/archpedi.1996.02170360056009. ISSN 1072-4710. PMID 8904857. S2CID 25465924.
- Everard, M. L.; Bara, A.; Kurian, M.; Elliott, T. M.; Ducharme, F. (2002). "Anticholinergic drugs for wheeze in children under the age of two years". The Cochrane Database of Systematic Reviews (1): CD001279. doi:10.1002/14651858.CD001279. ISSN 1469-493X. PMID 11869598.
- Bjornson, Candice; Russell, Kelly; Vandermeer, Ben; Klassen, Terry P.; Johnson, David W. (10 October 2013). "Nebulized epinephrine for croup in children". The Cochrane Database of Systematic Reviews (10): CD006619. doi:10.1002/14651858.CD006619.pub3. ISSN 1469-493X. PMID 24114291.
- Hartling, Lisa; Fernandes, Ricardo M.; Bialy, Liza; Milne, Andrea; Johnson, David; Plint, Amy; Klassen, Terry P.; Vandermeer, Ben (6 April 2011). "Steroids and bronchodilators for acute bronchiolitis in the first two years of life: systematic review and meta-analysis". BMJ (Clinical Research Ed.). 342: d1714. doi:10.1136/bmj.d1714. ISSN 1756-1833. PMC 3071611. PMID 21471175.
- Kua, KP; Lee, SWH (2017). "Systematic Review and Meta-Analysis of the Efficacy and Safety of Combined Epinephrine and Corticosteroid Therapy for Acute Bronchiolitis in Infants". Frontiers in Pharmacology. 8: 396. doi:10.3389/fphar.2017.00396. PMC 5479924. PMID 28690542.
- Hartling, L; Fernandes, RM; Bialy, L; Milne, A; Johnson, D; Plint, A; Klassen, TP; Vandermeer, B (6 April 2011). "Steroids and bronchodilators for acute bronchiolitis in the first two years of life: systematic review and meta-analysis". BMJ (Clinical Research Ed.). 342: d1714. doi:10.1136/bmj.d1714. PMC 3071611. PMID 21471175.
- Jat, Kana R.; Chawla, Deepak (24 August 2015). "Surfactant therapy for bronchiolitis in critically ill infants". The Cochrane Database of Systematic Reviews (8): CD009194. doi:10.1002/14651858.CD009194.pub3. ISSN 1469-493X. PMC 7104667. PMID 26299681.
- Lauwers, Eline; Ides, Kris; Van Hoorenbeeck, Kim; Verhulst, Stijn (November 2018). "The effect of intrapulmonary percussive ventilation in pediatric patients: A systematic review". Pediatric Pulmonology. 53 (11): 1463–1474. doi:10.1002/ppul.24135. hdl:10067/1522720151162165141. ISSN 1099-0496. PMID 30019451. S2CID 51680313.
- Liet, Jean-Michel; Ducruet, Thierry; Gupta, Vineet; Cambonie, Gilles (18 September 2015). "Heliox inhalation therapy for bronchiolitis in infants". The Cochrane Database of Systematic Reviews. 2015 (9): CD006915. doi:10.1002/14651858.CD006915.pub3. ISSN 1469-493X. PMC 8504435. PMID 26384333.
- Enriquez, Annabelle; Chu, I.-Wen; Mellis, Craig; Lin, Wan-Yu (14 November 2012). "Nebulised deoxyribonuclease for viral bronchiolitis in children younger than 24 months". The Cochrane Database of Systematic Reviews. 11: CD008395. doi:10.1002/14651858.CD008395.pub2. ISSN 1469-493X. PMC 7388903. PMID 23152257.
- Kua, Kok Pim; Lee, Shaun Wen Huey (17 February 2017). "Complementary and alternative medicine for the treatment of bronchiolitis in infants: A systematic review". PLOS ONE. 12 (2): e0172289. Bibcode:2017PLoSO..1272289K. doi:10.1371/journal.pone.0172289. ISSN 1932-6203. PMC 5315308. PMID 28212381.
- Bourke, T; Shields, M (11 April 2011). "Bronchiolitis". Clinical Evidence. 2011. PMC 3275170. PMID 21486501.
- Farley R, Spurling GK, Eriksson L, Del Mar CB (2014). "Antibiotics for bronchiolitis in children under two years of age" (PDF). Cochrane Database of Systematic Reviews. 2014 (10): CD005189. doi:10.1002/14651858.CD005189.pub4. PMID 25300167.
- McCallum, Gabrielle B.; Plumb, Erin J.; Morris, Peter S.; Chang, Anne B. (2017). "Antibiotics for persistent cough or wheeze following acute bronchiolitis in children". The Cochrane Database of Systematic Reviews. 2017 (8): CD009834. doi:10.1002/14651858.CD009834.pub3. ISSN 1469-493X. PMC 6483479. PMID 28828759.
- McCallum, Gabrielle B.; Plumb, Erin J.; Morris, Peter S.; Chang, Anne B. (22 August 2017). "Antibiotics for persistent cough or wheeze following acute bronchiolitis in children". The Cochrane Database of Systematic Reviews. 2017 (8): CD009834. doi:10.1002/14651858.CD009834.pub3. ISSN 1469-493X. PMC 6483479. PMID 28828759.
- Che, Si-Yi; He, Huan; Deng, Yu; Liu, En-Mei (August 2019). "[Clinical effect of azithromycin adjuvant therapy in children with bronchiolitis: a systematic review and Meta analysis]". Zhongguo Dang Dai Er Ke Za Zhi = Chinese Journal of Contemporary Pediatrics. 21 (8): 812–819. doi:10.7499/j.issn.1008-8830.2019.08.014. ISSN 1008-8830. PMC 7389899. PMID 31416508.
- Alarcón-Andrade, Gonzalo; Cifuentes, Lorena (7 May 2018). "Should systemic corticosteroids be used for bronchiolitis?". Medwave. 18 (3): e7207. doi:10.5867/medwave.2018.03.7206. ISSN 0717-6384. PMID 29750779.
- Alarcón-Andrade, Gonzalo; Cifuentes, Lorena (17 April 2018). "Do inhaled corticosteroids have a role for bronchiolitis?". Medwave. 18 (2): e7183. doi:10.5867/medwave.2018.02.7182. ISSN 0717-6384. PMID 29677180.
- Fernandes, Ricardo M.; Wingert, Aireen; Vandermeer, Ben; Featherstone, Robin; Ali, Samina; Plint, Amy C.; Stang, Antonia S.; Rowe, Brian H.; Johnson, David W.; Allain, Dominic; Klassen, Terry P. (1 August 2019). "Safety of corticosteroids in young children with acute respiratory conditions: a systematic review and meta-analysis". BMJ Open. 9 (8): e028511. doi:10.1136/bmjopen-2018-028511. ISSN 2044-6055. PMC 6688746. PMID 31375615.
- Pérez-Gutiérrez, Fernanda; Otárola-Escobar, Isidora; Arenas, Deidyland (16 December 2016). "Are leukotriene inhibitors useful for bronchiolitis?". Medwave. 16 (Suppl5): e6799. doi:10.5867/medwave.2016.6799. ISSN 0717-6384. PMID 28032855.
- Peng, Wan-Sheng; Chen, Xin; Yang, Xiao-Yun; Liu, En-Mei (March 2014). "Systematic review of montelukast's efficacy for preventing post-bronchiolitis wheezing". Pediatric Allergy and Immunology. 25 (2): 143–150. doi:10.1111/pai.12124. ISSN 1399-3038. PMID 24118637. S2CID 27539127.
- Liu, Fang; Ouyang, Jing; Sharma, Atul N; Liu, Songqing; Yang, Bo; Xiong, Wei; Xu, Rufu (16 March 2015). "Leukotriene inhibitors for bronchiolitis in infants and young children". Cochrane Database of Systematic Reviews (3): CD010636. doi:10.1002/14651858.CD010636.pub2. PMID 25773054.
- Sanders, Sharon L; Agwan, Sushil; Hassan, Mohamed; van Driel, Mieke L; Del Mar, Chris B (26 August 2019). "Immunoglobulin treatment for hospitalised infants and young children with respiratory syncytial virus infection". Cochrane Database of Systematic Reviews. 8: CD009417. doi:10.1002/14651858.CD009417.pub2. PMC 6708604. PMID 31446622.
External links
- Bronchiolitis. Patient information from NHS Choices
- "Bronchiolitis in children – A national clinical guideline" (PDF). Archived from the original (PDF) on 4 March 2016. Retrieved 6 December 2007. (1.74 MB) from the Scottish Intercollegiate Guidelines Network
- Ralston, SL; Lieberthal, AS; Meissner, HC; Alverson, BK; Baley, JE; Gadomski, AM; Johnson, DW; Light, MJ; Maraqa, NF; Mendonca, EA; Phelan, KJ; Zorc, JJ; Stanko-Lopp, D; Brown, MA; Nathanson, I; Rosenblum, E; Sayles S, 3rd; Hernandez-Cancio, S (27 October 2014). "Clinical Practice Guideline: The Diagnosis, Management, and Prevention of Bronchiolitis". Pediatrics. 134 (5): e1474–502. doi:10.1542/peds.2014-2742. PMID 25349312.