Esthesioneuroblastoma
| Esthesioneuroblastoma | |
|---|---|
| Other names: Neuroblastoma | |
 | |
| Esthesioneuroblastoma | |
| Specialty | Neuro-oncology |
Esthesioneuroblastoma is a rare cancer of the nasal cavity. Arising from the upper nasal tract, esthesioneuroblastoma is believed to originate from sensory neuroepithelial cells, also known as neuroectodermal olfactory cells.[1]
Due to the location of the tumor and its proximity to the cranial cavity, esthesioneuroblastoma can be highly invasive and challenging to treat. There is no consensus on an appropriate treatment approach of esthesioneuroblastoma because of the rarity of the disease. Most studies reported cranial surgical resection with radiotherapy or chemotherapy to target the tumor.[2]
Signs and symptoms
Esthesioneuroblastoma frequently first presents as a nasal mass.[3] The most common signs and symptoms of esthesioneuroblastoma are nasal obstruction (70%) and epistaxis (50%).[4][1] Less common symptoms include hyposmia (loss of smell), headache, rhinorrhea, vision loss, proptosis, facial pain, diplopia (double vision), masses in the neck and changes in mental status.[4] Esthesioneuroblastoma occurs in the upper nasal cavity, near the optic nerves and optic chiasm. Thus, tumor growth can impinge nerve function and result in vision loss and diplopia.[5] As the tumor metastasizes to the oral cavity, there can be tooth pain and tooth mobility.[6]
Genetics
There is limited research on the genetic role in esthesioneuroblastoma development. Of the research to date, the sonic hedgehog pathway, MYC and KDR genes are implicated for esthesioneuroblastoma.[7][8]
Mutations in dystrophin and Laminin, alpha 2 (LAMA2) have also been implicated in this disease.[9]
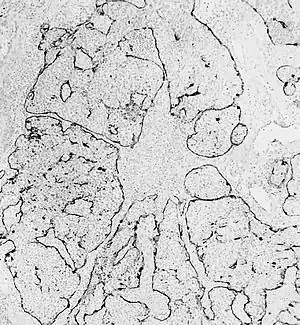
Pathophysiology
Esthesioneuroblastoma is of neurocrest origin, arising from olfactory sensory cells in the olfactory epithelium.[1] The olfactory epithelium consists of olfactory sensory cells, sustentacular cells and basal cells.[1] Esthesioneuroblastoma consists of lobular sheets with neurofibrullar fibers and rosettes.[4] Hyam's classifications are an important way of determining prognosis.[10]
Hyam's histopathological grades for esthesioneuroblastoma[11]
| Grade | Lobular architexture preservation | Mitotic index | Nuclear polymorphism | Fibrillary matrix | Rosettes | Necrosis |
|---|---|---|---|---|---|---|
| I | + | none | none | prominent | Homer Wright (HW) rosettes | none |
| II | + | low | moderate | present | HW rosettes | none |
| III | +/- | moderate | prominent | low | Flexner-Wintersteiner rosettes | rare |
| IV | +/- | high | marked | absent | none | frequent |
Diagnosis
Esthesioneuroblastoma can resemble small blue cell tumors like squamous cell carcinoma, sinonasal undifferentiated carcinoma, extranodal NK/T cell lymphoma, nasal type, rhabdomyosarcoma, Ewing/PNET, mucosal malignant melanoma and neuroendocrine carcinomas (NEC) that occur in the intranasal tract.[1] Compared to other tumors in the region, esthesioneuroblastoma has the best prognosis, with an overall five-year survival rate of 60–80%.[1] Fewer than 700 cases have been documented in the United States alone.[12] Esthesioneuroblastoma is characterized by neurofibrillary stroma and neurosecretary granules that are not seen concurrently by any other pathologies in the region.[1] Histological tests such as keratin, CK5/6, S-100 protein or NSE can be run to further differentiate esthesioneuroblastoma from other tumors.[1]
Staging
The Kadish classification is used for clinical classification of sinonasal tumors including esthesioneuroblastoma. Subsequent research articles have been published to determine prognosis based on tumor grade.
Modified Kadish classification[13][4]
| Stage | Description | 5 year survival |
|---|---|---|
| A | Tumor confined to nasal cavity | 75–91 |
| B | Nasal cavity and paranasal sinuses | 68–71 |
| C | Tumor extends beyond nasal cavity and paranasal sinuses, including skull base, orbit or cribiform plate | 41–47 |
| D | Tumor metastasizes to cervical lymph nodes and beyond | <40 |
Dulguerov classification[14]
| Stage | Characteristics |
|---|---|
| T1 | Tumour involving the nasal cavity and/or paranasal sinuses (excluding sphenoid), sparing the most superior ethmoidal cells |
| T2 | Tumour involving the nasal cavity and/or paranasal sinuses (including the sphenoid) with extension to or erosion of the cribriform plate |
| T3 | Tumour extending into the orbit or protruding into the anterior cranial fossa, without dural invasion |
| T4 | Tumour involving the brain |
| N0 | No cervical lymph-node metastasis |
| N1 | Any form of cervical lymph-node metastasis |
| M0 | No metastases |
| M1 | Distant metastasis |
Treatment
The preferred treatment for esthesioneuroblastoma is surgery followed by radiotherapy to prevent recurrence of the tumor.[14]
Surgical approaches
Several surgical approaches have been described,[15][16][17][18][19] but post-excision recurrence rates have remained relatively high. Studies suggest better results with a bilateral approach. For cases with cribriform plate involvement, tumors are resected bilaterally using a transfacial and craniotomy approach.[20] In a research study, the craniofacial approach decreased recurrence of esthesioneuroblastoma by 20%.[20] Craniofacial resection can help preserve the optic nerves and brain while removing the cribriform plate, olfactory bulb, dura surrounding the bulb and even the orbital periosteum.[14]
Radiotherapy
Radiotherapy alone is reserved only for small lesions not appropriate for either surgery or chemotherapy.[4] Both photon and proton radiotherapy have been used effectively to treat esthesioneuroblastoma.[14][21] Proton radiotherapy has recently been shown to be effective in a 10-person study with Kadish C tumors, while delivering less toxicity to the nervous system.[21]
Chemotherapy
Chemotherapy is used in a multimodality treatment plan generally for more advanced, unresectable or reoccurring tumors.[4] Cyclophosphamide, vincristine and doxorubicin have been used as neoadjuvant chemotherapy drugs for grade C esthesioneuroblastoma before surgical resection, producing fair outcomes. Cisplatin and etoposide are often used to treat esthesioneuroblastoma as neoadjuvants or adjuvants with radiotherapy or surgery.[22][23][24]
Study results are promising. In advanced stage esthesioneuroblastoma in pediatric patients, where surgery is no longer possible, aggressive chemotherapy and radiotherapy has resulted in some tumor control and long-term survival.[25]
Prognosis
Esthesioneuroblastoma is a slow developing but malignant tumor with high recurrence rates because of its anatomical position.[10] The tumor composition, location and metastatic characteristics as well as the treatment plan determine prognosis. Common clinical classification systems for esthesioneuroblastoma include the Kadish classification and the Dulguerov classification. Histopathological characteristics on top of Kadish classification can further determine cancer prognosis. In severe, Kadish class C tumors, Haym's grades of pathology are important for prognosis. Patients with low grade Kadish class C tumors have a 10-year survival rate of 86 percent compared to patients with high grade class C tumors who have a survival rate of 28 percent.[10] Surgically treated patients with high grade tumors are more likely to experience leptomeningeal metastases or involvement of the cerebral spinal fluid unlike patients with low grade tumors who usually only see local recurrence.[26]
Survival rates for treated esthesioneuroblastoma are best for surgery with radiotherapy (65%), then for radiotherapy and chemotherapy (51%), just surgery (48%), surgery, radiotherapy and chemotherapy (47%) and finally just radiotherapy (37%).[14] From the literature, radiotherapy and surgery seem to boast the best outcome for patients. However, it is important to understand that to some degree, prognosis is related to tumor severity. More progressed, higher grade tumors would result in chemotherapy or radiotherapy as the only treatment. It is no surprise that the prognosis would be worse in these cases.
Incidence
Esthesioneuroblastoma accounts for 2% of all intranasal tumors with an incidence of 0.4 cases per million people.[1] Fewer than 700 cases have been documented in the United States.[12] Fewer than 400 unique cases have been reported globally.[4][1] Esthesioneuroblastoma can occur at any time, with peak occurrence reported in the second and sixth decades of life.[1]
History
Esthesioneuroblastoma was first characterized in 1924.[27][28]
Notable cases
The disease was brought into prominence by the case of Chantal Sébire, who was suffering from the disease and ended her life after being denied euthanasia.[29]
References
- 1 2 3 4 5 6 7 8 9 10 11 Thompson LD (2009). Olfactory neuroblastoma. Head and neck pathology. 3: 252–259
- ↑ Jiang GY, Li FC, Chen WK, Liu AM, Cai WQ (December 2011). "Therapy and prognosis of intracranial invasive olfactory neuroblastoma". Otolaryngology–Head and Neck Surgery. 145 (6): 951–955. doi:10.1177/0194599811416752. PMID 21825099. S2CID 9860811.
- ↑ Ghaffar S, Salahuddin I (March 2005). "Olfactory neuroblastoma: a case report and review of the literature". Ear, Nose, & Throat Journal. 84 (3): 150–152. doi:10.1177/014556130508400311. PMID 15871582. S2CID 20079359. Archived from the original on 2021-11-09. Retrieved 2022-04-25.
- 1 2 3 4 5 6 7 Sheehan JM (2011). "Esthesioneuroblastoma". In Jane JA (ed.). Youmans Neurological Surgery (6th ed.). Retrieved 7 December 2016.
- ↑ Oskouian RJ, Jane JA, Dumont AS, Sheehan JM, Laurent JJ, Levine PA (May 2002). "Esthesioneuroblastoma: clinical presentation, radiological, and pathological features, treatment, review of the literature, and the University of Virginia experience". Neurosurgical Focus. 12 (5): e4. doi:10.3171/foc.2002.12.5.5. PMID 16119902.
- ↑ von Zeidler SV, Guidi R, Alencar R, Aguiar R, Mendonça EF, Batista AC, Ribeiro-Rotta RF (January 2014). "Atypical esthesioneuroblastoma invading oral cavity: a case report and review of the literature". Diagnostic Pathology. 9: 10. doi:10.1186/1746-1596-9-10. PMC 3943513. PMID 24443792.
- ↑ Mao L, Xia YP, Zhou YN, Dai RL, Yang X, Wang YJ, et al. (2009). "Activation of sonic hedgehog signaling pathway in olfactory neuroblastoma". Oncology. 77 (3–4): 231–243. doi:10.1159/000236047. PMID 19738389. S2CID 33078469.
- ↑ Weiss GJ, Liang WS, Izatt T, Arora S, Cherni I, Raju RN, et al. (2012). "Paired tumor and normal whole genome sequencing of metastatic olfactory neuroblastoma". PLOS ONE. 7 (5): e37029. Bibcode:2012PLoSO...737029W. doi:10.1371/journal.pone.0037029. PMC 3359355. PMID 22649506.
- ↑ Gallia GL, Zhang M, Ning Y, Haffner MC, Batista D, Binder ZA, et al. (December 2018). "Genomic analysis identifies frequent deletions of Dystrophin in olfactory neuroblastoma". Nature Communications. 9 (1): 5410. Bibcode:2018NatCo...9.5410G. doi:10.1038/s41467-018-07578-z. PMC 6303314. PMID 30575736.
- 1 2 3 Kaur G, Kane AJ, Sughrue ME, Madden M, Oh MC, Sun MZ, et al. (February 2013). "The prognostic implications of Hyam's subtype for patients with Kadish stage C esthesioneuroblastoma". Journal of Clinical Neuroscience. 20 (2): 281–286. doi:10.1016/j.jocn.2012.05.029. PMC 3795510. PMID 23266076.
- ↑ Hyams VG, Baksakis JG, Michaels L, eds. (1988). Tumors of the upper respiratory tract and ear. Washington DC: Armed Forces Institute of Pathology. pp. 240–248.
- 1 2 Stokes WA, Camilon PR, Banglawala SM, Nguyen SA, Harvey R, Vandergrift WA, Schlosser RJ (2015). "Is sex an independent prognostic factor in esthesioneuroblastoma?". American Journal of Rhinology & Allergy. 29 (5): 369–372. doi:10.2500/ajra.2015.29.4204. PMID 26358349. S2CID 41961725.
- ↑ Kadish S, Goodman M, Wang CC (March 1976). "Olfactory neuroblastoma. A clinical analysis of 17 cases". Cancer. 37 (3): 1571–1576. doi:10.1002/1097-0142(197603)37:3<1571::aid-cncr2820370347>3.0.co;2-l. PMID 1260676.
- 1 2 3 4 5 Dulguerov P, Allal AS, Calcaterra TC (November 2001). "Esthesioneuroblastoma: a meta-analysis and review". The Lancet. Oncology. 2 (11): 683–90. doi:10.1016/S1470-2045(01)00558-7. PMID 11902539. Archived from the original on 2021-11-09. Retrieved 2022-04-25.
- ↑ Roxbury CR, Ishii M, Gallia GL, Reh DD (February 2016). "Endoscopic Management of Esthesioneuroblastoma". Otolaryngologic Clinics of North America. 49 (1): 153–165. doi:10.1016/j.otc.2015.09.010. PMID 26614835.
- ↑ Vergani F, Pirola E, Fiori L, Pagni F, Parmigiani F, Sganzerla EP (June 2007). "Combined transcranial and endoscopic nasal resection for esthesioneuroblastoma. Technical note". Journal of Neurosurgical Sciences. 51 (2): 99–102. PMID 17571044.
- ↑ Unger F, Walch C, Stammberger H, Papaefthymiou G, Haselsberger K, Pendl G (June 2001). "Olfactory neuroblastoma (esthesioneuroblastoma): report of six cases treated by a novel combination of endoscopic surgery and radiosurgery". Minimally Invasive Neurosurgery. 44 (2): 79–84. doi:10.1055/s-2001-16000. PMID 11487789.
- ↑ Cakmak O, Ergin NT, Yilmazer C, Kayaselçuk F, Barutcu O (July 2002). "Endoscopic removal of esthesioneuroblastoma". International Journal of Pediatric Otorhinolaryngology. 64 (3): 233–238. doi:10.1016/S0165-5876(02)00036-8. PMID 12090952.
- ↑ Prasad KC, Kumar A, Prasad SC, Jain D (September 2007). "Endoscopic-assisted excision of esthesioneuroblastoma". The Journal of Craniofacial Surgery. 18 (5): 1034–1038. doi:10.1097/scs.0b013e318157264c. PMID 17912077. S2CID 27445039.
- 1 2 Spaulding CA, Kranyak MS, Constable WC, Stewart FM (September 1988). "Esthesioneuroblastoma: a comparison of two treatment eras". International Journal of Radiation Oncology, Biology, Physics. 15 (3): 581–590. doi:10.1016/0360-3016(88)90298-2. PMID 3138210.
- 1 2 Nichols AC, Chan AW, Curry WT, Barker FG, Deschler DG, Lin DT (September 2008). "Esthesioneuroblastoma: the massachusetts eye and ear infirmary and massachusetts general hospital experience with craniofacial resection, proton beam radiation, and chemotherapy". Skull Base. 18 (5): 327–337. doi:10.1055/s-2008-1076098. PMC 2637063. PMID 19240832.
- ↑ Porter AB, Bernold DM, Giannini C, Foote RL, Link MJ, Olsen KD, et al. (November 2008). "Retrospective review of adjuvant chemotherapy for esthesioneuroblastoma". Journal of Neuro-Oncology. 90 (2): 201–204. doi:10.1007/s11060-008-9645-y. PMID 18633576. S2CID 25788460.
- ↑ Bhattacharyya N, Thornton AF, Joseph MP, Goodman ML, Amrein PC (January 1997). "Successful treatment of esthesioneuroblastoma and neuroendocrine carcinoma with combined chemotherapy and proton radiation. Results in 9 cases". Archives of Otolaryngology–Head & Neck Surgery. 123 (1): 34–40. doi:10.1001/archotol.1997.01900010038005. PMID 9006501.
- ↑ Kim DW, Jo YH, Kim JH, Wu HG, Rhee CS, Lee CH, et al. (November 2004). "Neoadjuvant etoposide, ifosfamide, and cisplatin for the treatment of olfactory neuroblastoma". Cancer. 101 (10): 2257–2260. doi:10.1002/cncr.20648. PMID 15484215. S2CID 44518377.
- ↑ Bisogno G, Soloni P, Conte M, Podda M, Ferrari A, Garaventa A, et al. (March 2012). "Esthesioneuroblastoma in pediatric and adolescent age. A report from the TREP project in cooperation with the Italian Neuroblastoma and Soft Tissue Sarcoma Committees". BMC Cancer. 12: 117. doi:10.1186/1471-2407-12-117. PMC 3368746. PMID 22443159.
- ↑ Malouf GG, Casiraghi O, Deutsch E, Guigay J, Temam S, Bourhis J (April 2013). "Low- and high-grade esthesioneuroblastomas display a distinct natural history and outcome". European Journal of Cancer. 49 (6): 1324–1334. doi:10.1016/j.ejca.2012.12.008. PMID 23312882.
- ↑ Fordice JO (3 March 1994). "Esthesioneuroblastoma". Baylor College of Medicine. Archived from the original on April 9, 2007. Retrieved 2008-03-22.
- ↑ Berger L, Luc G, Richard D (1924). "L'esthésioneuroépithéliome olfactif". Bull Assoc Franç Étude Cancer. 13: 410–421.
- ↑ "BBC NEWS - Europe - Tumour woman's death not natural". BBC. 21 March 2008. Archived from the original on 10 December 2008. Retrieved 1 November 2016.
External links
| Classification | |
|---|---|
| External resources |