Congenital absence of the vas deferens
| Congenital absence of the vas deferens | |
|---|---|
| Specialty | Urology |
| Causes | genetic mutations. |
Congenital absence of the vas deferens (CAVD) is a condition in which the vasa deferentia reproductive organs fail to form properly prior to birth. It may either be unilateral (CUAVD) or bilateral (CBAVD).
Signs and symptoms
The vas deferens connect the sperm-producing testicles to the penis. Therefore, those who are missing both vas deferens are typically able to create sperm but are unable to transport them appropriately. Their semen does not contain sperm, a condition known as azoospermia. Unilateral absence may not show any abnormalities in semen analysis.
Vas deferens are less commonly palpated during routine a physical examination, hence the absence may go unnoticed. Also, injury to Vas deferens common in surgery.[1] Vas deferens may be absent on one or both sides, and in whole or in part. When only a part of Vas deferens is absent, it may fail to establish communication with the epididymis.[2]
In one of the largest such studies, a study of 23,013 individuals seeking for vasectomy, 159 were suspected to be having UAVD. Among 159 men identified as potentially having CUAVD, 47 had only one testicle, 26 had bilateral vasa, and four were misdiagnosed (post-vasectomy semen analysis showing motile sperm after unilateral vasectomy) leaving 82 men deemed cases of CUAVD (0.36% of total sample). 82 men were further classified as confirmed (n=48, 0.21%) and possible (n=34, 0.15%; 22 without and 12 with scrotal anomalies) congenital UAVD. The misdiagnosis ratio of CUAVD was low when scrotal content was otherwise normal (1:48), but higher if anomalies were present (3:12). Miller, Sarah et al. “Unilateral absence of vas deferens: prevalence among 23.013 men seeking vasectomy.”[3]
Causes
There are two main populations of CAVD; the larger group is associated with cystic fibrosis and occurs because of a mutation in the CFTR gene,[4][5] while the smaller group (estimated between 10 and 40%) is associated with unilateral renal agenesis (URA). The mutational spectrum of CFTR in the first group differs from that observed in classic cystic fibrosis, with milder missense or splice variants present on at least one chromosome.[6][7] The genetic basis of the second group is not well understood. In the subset of males with both CBAVD and URA, the CFTR mutation has been shown to occur at a rate only slightly higher than the overall population. It has been suggested that another gene may be responsible for this condition.[7][8]
Mutation of the CFTR gene is found to result in obstructive azoospermia in postpubertal males with cystic fibrosis. Strikingly, CAVD is one of the most consistent features of cystic fibrosis as it affects 98-99% of individuals in this CF patient population. In contrast, acute or persistent respiratory symptoms present in only 51% of total CF patients.[9]
Diagnosis
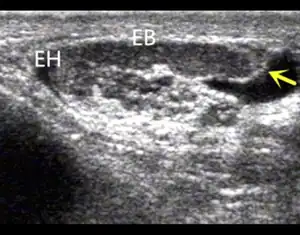
Scrotal ultrasonography and transrectal ultrasonography (TRUS) are useful in detecting uni- or bilateral CAVD, which may be associated with visible abnormalities or agenesis of the epididymis, seminal vesicles or kidneys.[10]
Treatment
Individuals with CAVD can reproduce with the assistance of modern technology with a combination of testicular sperm extraction and intracytoplasmic sperm injection (ICSI). However, as the risk of either cystic fibrosis or renal agenesis is likely to be higher in the children, genetic counseling is generally recommended.
References
- ↑ Donohue, R. E.; Fauver, H. E. (1989-02-24). "Unilateral absence of the vas deferens. A useful clinical sign". JAMA. 261 (8): 1180–1182. doi:10.1001/jama.1989.03420080100041. PMID 2604761.
- ↑ Chawla, S (October 1999). "Congenital Unilateral Absence of the Vas Deferens". Medical Journal Armed Forces India. 55 (4): 375. doi:10.1016/S0377-1237(17)30530-0. PMC 5531955. PMID 28790624.
- ↑ Miller, Sarah; Couture, Sophie; James, Gareth; Plourde, Simon; Rioux, Jacky; Labrecque, Michel (October 2016). "Unilateral absence of vas deferens: prevalence among 23,013 men seeking vasectomy". International Braz J Urol. 42 (5): 1010–1017. doi:10.1590/S1677-5538.IBJU.2015.0717. PMC 5066900. PMID 27509370.
- ↑ Online Mendelian Inheritance in Man (OMIM): VAS DEFERENS, CONGENITAL BILATERAL APLASIA OF; CBAVD - 277180
- ↑ Grangeia A, Sá R, Carvalho F, et al. (2007). "Molecular characterization of the cystic fibrosis transmembrane conductance regulator gene in congenital absence of the vas deferens". Genet. Med. 9 (3): 163–72. doi:10.1097/GIM.0b013e3180318aaf. PMID 17413420.
- ↑ Chillón M, Casals T, Mercier B, Bassas L, Lissens W, Silber S, Romey MC, Ruiz-Romero J, Verlingue C, Claustres M, et al. (1995). "Mutations in the cystic fibrosis gene in patients with congenital absence of the vas deferens". N. Engl. J. Med. 332 (22): 1475–80. doi:10.1056/NEJM199506013322204. hdl:2445/44112. PMID 7739684.
- 1 2 Dörk T, Dworniczak B, Aulehla-Scholz C, Wieczorek D, Böhm I, Mayerova A, Seydewitz HH, Nieschlag E, Meschede D, Horst J, Pander HJ, Sperling H, Ratjen F, Passarge E, Schmidtke J, Stuhrmann M (1997). "Distinct spectrum of CFTR gene mutations in congenital absence of vas deferens". Hum. Genet. 100 (3–4): 365–377. doi:10.1007/s004390050518. PMID 9272157. S2CID 24344109.
- ↑ McCallum T, Milunsky J, Munarriz R, Carson R, Sadeghi-Nejad H, Oates R (2001). "Unilateral renal agenesis associated with congenital bilateral absence of the vas deferens: phenotypic findings and genetic considerations". Hum. Reprod. 16 (2): 282–288. doi:10.1093/humrep/16.2.282. PMID 11157821.
- ↑ Rosenstein BJ, Cutting GR (1998). "The diagnosis of cystic fibrosis: a consensus statement. Cystic Fibrosis Foundation Consensus Panel". J. Pediatr. 132 (4): 589–95. doi:10.1016/S0022-3476(98)70344-0. PMID 9580754.
- ↑ Lotti, F.; Maggi, M. (2014). "Ultrasound of the male genital tract in relation to male reproductive health" (PDF). Human Reproduction Update. 21 (1): 56–83. doi:10.1093/humupd/dmu042. ISSN 1355-4786. PMID 25038770. Archived (PDF) from the original on 2021-12-15. Retrieved 2022-04-02.
External links
| Classification |
|---|
- "Congenital bilateral absence of the vas deferens". Genetics Home Reference. Archived from the original on 2010-04-08. Retrieved 2022-04-02.
- Congenital bilateral aplasia of vas deferens; Congenital bilateral absence of the vas deferens at NIH's Office of Rare Diseases