Diabetic retinopathy
| Diabetic retinopathy | |
|---|---|
| Other names: diabetic eye disease, DED | |
 | |
| Image of fundus showing scatter laser surgery for diabetic retinopathy | |
| Pronunciation |
|
| Specialty | Ophthalmology, optometry |
| Symptoms | Ranges from asymptomatic to blurry vision, partial vision loss, nyctalopia and blindness |
| Complications | Vitreous hemorrhage, Retinal detachment, Glaucoma, Blindness[2] |
| Duration | Lifelong |
| Causes | Long-term poor control of diabetes mellitus |
| Risk factors | Diabetes, poor control of blood sugar, smoking |
| Diagnostic method | Eye examination[3] |
| Treatment | Laser coagulation, Vitrectomy[3] |
| Medication | Anti-VEGF Injection[3] |
| Frequency | Nearly all patients with type 1 diabetes and >60% of patients with type 2 diabetes[4] |
Diabetic retinopathy, also known as diabetic eye disease (DED),[5] is a medical condition in which damage occurs to the retina due to diabetes mellitus. It is a leading cause of blindness in developed countries.[6]
Diabetic retinopathy affects up to 80 percent of those who have had both type 1 and type 2 diabetes for 20 years or more.[7] In at least 90% of new cases, progression to more aggressive forms of sight threatening retinopathy and maculopathy could be reduced with proper treatment and monitoring of the eyes.[8] The longer a person has diabetes, the higher his or her chances of developing diabetic retinopathy.[9] Each year in the United States, diabetic retinopathy accounts for 12% of all new cases of blindness. It is also the leading cause of blindness in people aged 20 to 64.[10]
Signs and symptoms

Diabetic retinopathy often has no early warning signs. Even macular edema, which can cause rapid central vision loss, may not have any warning signs for some time. In general, however, a person with macular edema is likely to have blurred vision, making it hard to do things like read or drive. In some cases, the vision will get better or worse during the day.
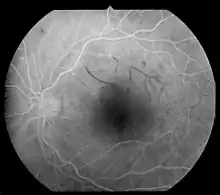
The first stage, called non-proliferative diabetic retinopathy (NPDR), has no symptoms. Patients may not notice the signs and have 20/20 vision. The only way to detect NPDR is by fundus examination by direct or indirect ophthalmoscope by a trained ophthalmologist or optometrist, fundus photography can be used for objective documentation of the fundus findings, in which microaneurysms (microscopic blood-filled bulges in the artery walls) can be seen. If there is reduced vision, fluorescein angiography can show narrowing or blocked retinal blood vessels clearly (lack of blood flow or retinal ischemia).
Macular edema, in which blood vessels leak their contents into the macular region, can occur at any stage of NPDR. Its symptoms are blurred vision and darkened or distorted images that are not the same in both eyes. Ten percent (10%) of diabetic patients will have vision loss related to macular edema. Optical Coherence Tomography can show areas of retinal thickening due to fluid accumulation from macular edema.[11]
In the second stage, abnormal new blood vessels (neovascularisation) form at the back of the eye as part of proliferative diabetic retinopathy (PDR); these can burst and bleed (vitreous hemorrhage) and blur the vision, because these new blood vessels are fragile. The first time this bleeding occurs, it may not be very severe. In most cases, it will leave just a few specks of blood, or spots floating in a person's visual field which may last for months.
These spots are often followed within a few days or weeks by a much greater leakage of blood, which blurs the vision. In extreme cases, a person may only be able to tell light from dark in that eye. It may take the blood anywhere from a few days to months or even years to clear from the inside of the eye, and in some cases the blood will not clear. These types of large hemorrhages tend to happen more than once.
On funduscopic exam, a doctor will see cotton wool spots, flame hemorrhages, and dot-blot hemorrhages.
Risk factors
All people with diabetes are at risk—those with Type I diabetes and those with Type II diabetes. The longer a person has had diabetes, the higher their risk of developing some ocular problem. Between 40 and 45 percent of Americans diagnosed with diabetes have some stage of diabetic retinopathy.[12] After 20 years of diabetes, nearly all patients with Type I diabetes and >60% of patients with Type II diabetes have some degree of retinopathy; however, these statistics were published in 2002 using data from four years earlier, limiting the usefulness of the research. The subjects would have been diagnosed with diabetes in the late 1970s, before modern fast-acting insulin and home glucose testing.
Prior studies had also assumed a clear glycemic threshold between people at high and low risk of diabetic retinopathy.[13][14]
Published rates vary between trials, the proposed explanation being differences in study methods and reporting of prevalence rather than incidence values.[15]
During pregnancy, diabetic retinopathy may also be a problem for women with diabetes. The US National Institutes of Health recommends[16] that all pregnant women with diabetes have comprehensive eye examination.
People with Down syndrome, who have extra chromosome 21 material, almost never acquire diabetic retinopathy. This protection appears to be due to the elevated levels of endostatin,[17] an anti-angiogenic protein, derived from collagen XVIII. The collagen XVIII gene is located on chromosome 21.
Incidence of Retinitis Pigmentosa is observed to result in fewer and less severe microvascular lesions in both humans and mouse models.[18] Retinitis Pigmentosa results in loss of rod receptors in the mid peripheral field, reducing the oxygen consumption that is linked with release of VEGF and growth of unwanted blood vessels in the retina.
Genetics also play a role in diabetic retinopathy. Genetic predisposition to diabetic retinopathy in type 2 diabetes consists of many genetic variants across the genome that are collectively associated with diabetic retinopathy (polygenic risk) and overlaps with genetic risk for glucose, low-density lipoprotein cholesterol, and systolic blood pressure.[19]
Pathogenesis

Diabetic retinopathy is the result of damage to the small blood vessels and neurons of the retina. The earliest changes leading to diabetic retinopathy include narrowing of the retinal arteries associated with reduced retinal blood flow; dysfunction of the neurons of the inner retina, followed in later stages by changes in the function of the outer retina, associated with subtle changes in visual function; dysfunction of the blood-retinal barrier, which protects the retina from many substances in the blood (including toxins and immune cells), leading to the leaking of blood constituents into the retinal neuropile.[20] Later, the basement membrane of the retinal blood vessels thickens, capillaries degenerate and lose cells, particularly pericytes and vascular smooth muscle cells. This leads to loss of blood flow and progressive ischemia, and microscopic aneurysms which appear as balloon-like structures jutting out from the capillary walls, which recruit inflammatory cells; and advanced dysfunction and degeneration of the neurons and glial cells of the retina.[20][21] The condition typically develops about 10–15 years after receiving the diagnosis of diabetes mellitus.
An experimental study suggests that pericyte death is caused by blood glucose persistently activating protein kinase C and mitogen-activated protein kinase (MAPK), which, through a series of intermediates, inhibits signaling through platelet-derived growth factor receptors — signaling that supports cellular survival, proliferation, and growth. The resulting withdrawal of this signaling leads to the programmed cell death (apoptosis) of the cells in this experimental model.[22]
In addition, excessive sorbitol in diabetics is deposited on retina tissue and it is also proposed to play a role in diabetic retinopathy.[23]
Small blood vessels – such as those in the eye – are especially vulnerable to poor blood sugar (blood glucose) control. An overaccumulation of glucose damages the tiny blood vessels in the retina. During the initial stage, called nonproliferative diabetic retinopathy (NPDR), most people do not notice any change in their vision. Early changes that are reversible and do not threaten central vision are sometimes termed background retinopathy.[24]
A genetic study showed that diabetic retinopathy shares a similar genetic predisposition with levels of glucose, low-density lipoprotein cholesterol, and systolic blood pressure,[19] indicating that glycemic control and cardiometabolic factors may be important in the development of diabetic retinopathy.
Some people develop a condition called macular edema. It occurs when the damaged blood vessels leak fluid and lipids onto the macula, the part of the retina that lets us see detail. The fluid makes the macula swell, which blurs vision.
Proliferative diabetic retinopathy
As the disease progresses, severe nonproliferative diabetic retinopathy enters an advanced or proliferative (PDR) stage, where blood vessels proliferate/grow. The lack of oxygen in the retina causes formation of new fragile blood vessels to grow along the retina and in the clear, gel-like vitreous humour that fills the inside of the eye. Without timely treatment, these new blood vessels can bleed and cause cloudy vision, and destroy the retina. Fibrovascular proliferation can also cause tractional retinal detachment. The new blood vessels can also grow into the angle of the anterior chamber of the eye and cause neovascular glaucoma.
Nonproliferative diabetic retinopathy shows up as cotton wool spots, or microvascular abnormalities or as superficial retinal hemorrhages. Even so, the advanced proliferative diabetic retinopathy (PDR) can remain asymptomatic for a very long time, and so should be monitored closely with regular checkups.
Diagnosis

Diabetic retinopathy is detected during an eye examination that includes:
- Visual acuity test: Uses an eye chart to measure how well a person sees at various distances (i.e., visual acuity).
- Pupil dilation: The eye care professional places drops into the eye to dilate the pupil. This allows him or her to see more of the retina and look for signs of diabetic retinopathy. After the examination, close-up vision may remain blurred for several hours.
- Ophthalmoscopy or fundus photography: Ophthalmoscopy is an examination of the retina in which the eye care professional: (1) looks through a slit lamp biomicroscope with a special magnifying lens that provides a narrow view of the retina, or (2) wearing a headset (indirect ophthalmoscope) with a bright light, looks through a special magnifying glass and gains a wide view of the retina. Hand-held ophthalmoscopy is insufficient to rule out significant and treatable diabetic retinopathy. Fundus photography generally captures considerably larger areas of the fundus, and has the advantage of photo documentation for future reference, as well as availing the image to be examined by a specialist at another location and/or time.
- Fundus Fluorescein angiography (FFA): This is an imaging technique which relies on the circulation of fluorescein dye to show staining, leakage, or non-perfusion of the retinal and choroidal vasculature.
- Retinal vessel analysis detects abnormalities of the autoregulation of small retinal arteries and veins in diabetic patients even before the manifestation of diabetic retinopathy.[25] Such an impairment of retinal responsiveness is seen as one of the earliest markers of vascular dysfunction in diabetes possibly indicating subsequent risk of stroke.[26]
- Optical coherence tomography (OCT): This is an optical imaging modality based upon laser beam interference. It produces cross-sectional images of the retina (B-scans) which can be used to measure the thickness of the retina and to resolve its major layers, allowing the observation of swelling.
The eye care professional will look at the retina for early signs of the disease, such as:
- leaking blood vessels,
- retinal swelling, such as macular edema,
- pale, fatty deposits on the retina (exudates) – signs of leaking blood vessels,
- damaged nerve tissue (neuropathy), and
- any changes in the blood vessels.
If macular edema is suspected, OCT and sometimes retinal angiography (FFA) may be performed.
Diabetic retinopathy also affects microcirculation thorough the body. A recent study[27] showed assessment of conjunctival microvascular hemodynamics such as vessel diameter, red blood cell velocity and wall shear stress can be useful for diagnosis and screening of diabetic retinopathy. Furthermore, the pattern of conjunctival microvessels was shown to be useful for rapid monitoring and diagnosis of different stages of diabetic retinopathy.[28]
Google is testing a cloud algorithm that scans photos of the eye for signs of retinopathy. The algorithm still requires FDA approval.[29]
According to a DRSS user manual, poor quality retina images used for screening (which may apply to other methods) may be caused by cataract, poor dilation, ptosis, external ocular condition, or learning difficulties. There may be artefacts caused by dust, dirt, condensation, or smudge.[30]
Screening
In the UK, screening for diabetic retinopathy is part of the standard of care for people with diabetes.[31] After one normal screening in people with diabetes, further screening is recommended every two years.[32] In the UK, this is recommended every year.[33] Teleophthalmology has been employed in these programs.[34] In The U.S, a current guideline for diabetic retinopathy is recommendation of annual dilated exams for all patients with diabetes. There are barriers to recommended screening that is contributing to the disparity. Such as the patient factor which includes education about diabetic retinopathy and the availability of the treatment. The health care system also contributes to the disparities in diabetic screening, which includes insurance coverage, long waiting time for the appointment and difficulty scheduling appointments which makes the person less likely to screen. Provider factors also influence the barrier to screening which is a lack of awareness of the screening guidelines, skills or having the right tools to perform eye exams which can affect the diagnosis and treatment. A cross-sectional study showed that when physicians treating black patients had more difficulty providing proper subspecialty care and diagnostic imaging for the patients.[35]
There is evidence to support interventions to improve attendance for diabetic retinopathy screening.[36] These might be specifically targeted at diabetic retinopathy screening, or could be general strategies to improve diabetes care.
In addition, significant differences in genetic risk for diabetic retinopathy[19] raises the possibility of risk stratification and screening targeted to individuals with high genetic risk for diabetic retinopathy in the population.
Management
There are three major treatments for diabetic retinopathy, which are very effective in reducing vision loss from this disease.[37] In fact, even people with advanced retinopathy have a 95 percent chance of keeping their vision when they get treatment before the retina is severely damaged.[38] These three treatments are laser surgery, injection of corticosteroids or anti-VEGF agents into the eye, and vitrectomy.
Although these treatments are very successful (in slowing or stopping further vision loss), they do not cure diabetic retinopathy. Caution should be exercised in treatment with laser surgery since it causes a loss of retinal tissue. It is often more prudent to inject triamcinolone or anti-VEGF drugs. In some patients it results in a marked increase of vision, especially if there is an edema of the macula.[37]
Although commonly used in some parts of the world, it is unclear whether herbal medicine (for example, Ruscus extract and Radix Notoginseng extract) are of benefit to people with diabetic retinopathy.[39]
Avoiding tobacco use and correction of associated hypertension are important therapeutic measures in the management of diabetic retinopathy.[40]
Obstructive sleep apnea (OSA) has been associated with a higher incidence of diabetic eye disease due to blood desaturation caused by intermittent upper airway obstructions. Treatment for OSA can help reduce the risk of diabetic complications.[41]
The best way of preventing the onset and delaying the progression of diabetic retinopathy is to monitor it vigilantly and achieve optimal glycemic control.[42]
Since 2008 there have been other therapies (e.g. kinase inhibitors and anti-VEGF) drugs available.[43]
Laser photocoagulation
Laser photocoagulation can be used in two scenarios for the treatment of diabetic retinopathy. Firstly, It can be used to treat macular edema which was common before eye injections were introduced.[44] and secondly, it can be used for treating whole retina (panretinal photocoagulation) for controlling neovascularization. It is widely used for early stages of proliferative retinopathy. There are different types of lasers and there is evidence available on their benefits to treat proliferative diabetic retinopathy.[45]
Modified grid laser
A 'C' shaped area around the macula is treated with low intensity small burns. This helps in clearing the macular edema.
Panretinal
Panretinal photocoagulation, or PRP (also called scatter laser treatment), is used to treat proliferative diabetic retinopathy (PDR). The goal is to create 1,600 – 2,000 burns in the retina with the hope of reducing the retina's oxygen demand, and hence the possibility of ischemia. It is done in multiple sittings.
In treating advanced diabetic retinopathy, the burns are used to destroy the abnormal new blood vessels that form in the retina. This has been shown to reduce the risk of severe vision loss for eyes at risk by 50%.[7]
Before using the laser, the ophthalmologist dilates the pupil and applies anaesthetic drops to numb the eye. In some cases, the doctor also may numb the area behind the eye to reduce discomfort. The patient sits facing the laser machine while the doctor holds a special lens on the eye. The physician can use a single spot laser, a pattern scan laser for two dimensional patterns such as squares, rings and arcs, or a navigated laser which works by tracking retinal eye movements in real time.[46][47] During the procedure, the patient will see flashes of light. These flashes often create an uncomfortable stinging sensation for the patient. After the laser treatment, patients should be advised not to drive for a few hours while the pupils are still dilated. Vision will most likely remain blurry for the rest of the day. Though there should not be much pain in the eye itself, an ice-cream headache like pain may last for hours afterwards.
Patients will lose some of their peripheral vision after this surgery although it may be barely noticeable by the patient. The procedure does however save the center of the patient's sight. Laser surgery may also slightly reduce colour and night vision.
A person with proliferative retinopathy will always be at risk for new bleeding, as well as glaucoma, a complication from the new blood vessels. This means that multiple treatments may be required to protect vision.
Medications
Intravitreal triamcinolone acetonide
Triamcinolone is a long acting steroid preparation. Treating people with DME with intravitreal injections of triamcinolone may lead to a some degree of improvement in visual acuity when compared to eyes treated with placebo injections.[48] When injected in the vitreous cavity, the steroid decreases the macular edema (thickening of the retina at the macula) caused due to diabetic maculopathy, and that may result in an increase in visual acuity. The effect of triamcinolone is not permnanent and may last up to three months, which necessitates repeated injections for maintaining the beneficial effect. Best results of intravitreal Triamcinolone have been found in eyes that have already undergone cataract surgery. Complications of intravitreal injection of triamcinolone may include cataract, steroid-induced glaucoma, and endophthalmitis.[48]
Intravitreal anti-VEGF
There are good results from multiple doses of intravitreal injections of anti-VEGF drugs such as bevacizumab.[49] A 2017 systematic review update found moderate evidence that aflibercept may have advantages in improving visual outcomes over bevacizumab and ranibizumab, after one year.[50] In cases with vitreous hemorrhage, however, anti-VEGF injections proved to be less effective in restoring visual acuity than vitrectomy combined with panretinal laser-photocoagulation.[51] Present recommended treatment for diabetic macular edema is multiple injections of anti-VEGF drugs sometimes combined with Modified Grid laser photocoagulation. Sustained delivery systems for anti-VEGF medications can reduce the chances of endophthalmitis development by reducing the number of intravitreal injections necessary for treatment. Hydrogels have shown great promise for this platform.[52]
Topical medications
There is little evidence for the role of topical medications in the treatment of macular edema, for example, topical non‐steroidal anti‐inflammatory agents.[53]
Surgery
Instead of laser surgery, some people require a vitrectomy to restore vision. A vitrectomy is performed when there is a lot of blood in the vitreous. It involves removing the cloudy vitreous and replacing it with a saline solution.
Studies show that people who have a vitrectomy soon after a large hemorrhage are more likely to protect their vision than someone who waits to have the operation. Early vitrectomy is especially effective in people with insulin-dependent diabetes, who may be at greater risk of blindness from a hemorrhage into the eye.
Vitrectomy may be done under general or local anesthesia. The doctor makes a tiny incision in the sclera, or white of the eye. Next, a small instrument is placed into the eye to remove the vitreous and insert the saline solution into the eye.
Patients may be able to return home soon after the vitrectomy, or may be asked to stay in the hospital overnight. After the operation, the eye will be red and sensitive, and patients usually need to wear an eyepatch for a few days or weeks to protect the eye. Medicated eye drops are also prescribed to protect against infection. There is evidence which suggests anti-VEGF drugs given either prior to or during vitrectomy may reduce the risk of posterior vitreous cavity haemorrhage.[54] Vitrectomy is frequently combined with other modalities of treatment.
Research
Light treatment
A medical device comprising a mask that delivers green light through the eyelids while a person sleeps was under development in 2016.[55][56] The light from the mask stops rod cells in the retina from dark adapting, which is thought to reduce their oxygen requirement, which in turn diminishes new blood vessel formation and thus prevents diabetic retinopathy.[55] As of 2016 a large clinical trial was underway.[55] As of 2018, the results from the clinical trial showed no long-term therapeutic benefit from using the mask in diabetic retinopathy patients.[57]
C-peptide
C-peptide had shown promising results in treatment of diabetic complications incidental to vascular degeneration.[58] Creative Peptides,[59] Eli Lilly,[60] and Cebix[61] all had drug development programs for a C-peptide product. Cebix had the only ongoing program until it completed a Phase IIb trial in December 2014 that showed no difference between C-peptide and placebo, and it terminated its program and went out of business.[62][63]
Stem cell therapy
Clinical trials are under way or are being populated in preparation for study at medical centers in Brazil, Iran and the United States. Current trials involve using the patients' own stem cells derived from bone marrow and injected into the degenerated areas in an effort to regenerate the vascular system.[64]
Blood pressure control
A Cochrane review examined 15 randomized controlled trials to determine whether interventions that sought to control or reduce blood pressure in diabetics had any effects of diabetic retinopathy.[65] While the results showed that interventions to control or reduce blood pressure prevented diabetic retinopathy for up to 4–5 years in diabetics, there was no evidence of any effect of these interventions on progression of diabetic retinopathy, preservation of visual acuity, adverse events, quality of life, and costs.[65]
Fundoscopic image analyses
Diabetic retinopathy is diagnosed entirely by recognizing abnormalities on retinal images taken by fundoscopy. Color fundus photography is mainly used for staging the disease. Fluorescein angiography is used to assess the extent of retinopathy that aids in treatment plan development. Optical coherence tomography (OCT) is used to determine the severity of edema and treatment response.[67]
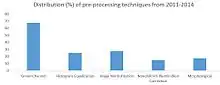
Because fundoscopic images are the main sources for diagnosis of diabetic retinopathy, manually analyzing those images can be time-consuming and unreliable, as the ability of detecting abnormalities varies by years of experience.[68] Therefore, scientists have explored developing computer-aided diagnosis approaches to automate the process, which involves extracting information about the blood vessels and any abnormal patterns from the rest of the fundoscopic image and analyzing them.[66]
See also
- Diabetic diet
- Diabetic papillopathy
- Purtscher's retinopathy, a disease with similar abnormalities in the eye, usually caused by trauma.
- Retinal regeneration[69]
References
- ↑ "Retinopathy | Definition of Retinopathy by Oxford Dictionary". lexico.com. Archived from the original on 2022-08-08. Retrieved 2022-06-29.
- ↑ "Diabetic retinopathy - Symptoms and causes". mayoclinic.org. Mayo Clinic. Archived from the original on 2022-06-28.
- 1 2 3 "Diabetic retinopathy - Diagnosis and treatment". mayoclinic.org. Mayo Clinic. Archived from the original on 2022-05-28.
- ↑ Fong, D. S.; Aiello, L.; Gardner, T. W.; et al. (2004). "Retinopathy in Diabetes". Diabetes Care. American Diabetes Association. 27: S84–S87. doi:10.2337/diacare.27.2007.S84. PMID 14693935. Archived from the original on 2021-10-06. Retrieved 2022-06-29.
- ↑ Li, Jeany Q.; Welchowski, Thomas; Schmid, Matthias; et al. (January 12, 2020). "Prevalence, incidence and future projection of diabetic eye disease in Europe: a systematic review and meta-analysis". European Journal of Epidemiology. 35 (1): 11–23. doi:10.1007/s10654-019-00560-z. PMID 31515657. S2CID 202557582. Archived from the original on June 15, 2022. Retrieved June 29, 2022 – via PubMed.
- ↑ "Diabetic retinopathy". Diabetes.co.uk. Archived from the original on 27 December 2018. Retrieved 25 November 2012.
- 1 2 Kertes PJ, Johnson TM, eds. (2007). Evidence Based Eye Care. Philadelphia, PA: Lippincott Williams & Wilkins. ISBN 978-0-7817-6964-8.
- ↑ Tapp RJ, Shaw JE, Harper CA, de Courten MP, Balkau B, McCarty DJ, Taylor HR, Welborn TA, Zimmet PZ (June 2003). "The prevalence of and factors associated with diabetic retinopathy in the Australian population". Diabetes Care. 26 (6): 1731–7. doi:10.2337/diacare.26.6.1731. PMID 12766102.
- ↑ MacEwen C. "diabetic retinopathy". Archived from the original on September 10, 2015. Retrieved August 2, 2011.
- ↑ Engelgau MM, Geiss LS, Saaddine JB, Boyle JP, Benjamin SM, Gregg EW, Tierney EF, Rios-Burrows N, Mokdad AH, Ford ES, Imperatore G, Narayan KM (June 2004). "The evolving diabetes burden in the United States". Annals of Internal Medicine. 140 (11): 945–50. doi:10.7326/0003-4819-140-11-200406010-00035. PMID 15172919.
- ↑ "Nonproliferative Diabetic Retinopathy (Includes Macular Edema)". Archived from the original on February 13, 2013. Retrieved August 17, 2013.
- ↑ "Diabetic Retinopathy: What You Should Know" (PDF). nei.nih.gov. National Eye Institute, National Institutes of Health. June 2019. p. 3. Archived (PDF) from the original on 7 July 2022. Retrieved 19 November 2021.
- ↑ Expert Committee on the Diagnosis Classification of Diabetes Mellitus (January 2003). "Report of the expert committee on the diagnosis and classification of diabetes mellitus". Diabetes Care. 26 (Suppl 1): S5–20. doi:10.2337/diacare.26.2007.S5. PMID 12502614.
- ↑ Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (July 1997). "Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus". Diabetes Care. 20 (7): 1183–97. doi:10.2337/diacare.20.7.1183. PMID 9203460. S2CID 219226914. Archived from the original on 2016-03-04. Retrieved 2022-06-29.
- ↑ Williams R, Airey M, Baxter H, Forrester J, Kennedy-Martin T, Girach A (October 2004). "Epidemiology of diabetic retinopathy and macular oedema: a systematic review". Eye. 18 (10): 963–83. doi:10.1038/sj.eye.6701476. PMID 15232600.
- ↑ "Facts About Diabetic Eye Disease". nei.nih.gov. National Eye Institute, National Institutes of Health. Archived from the original on 2018-12-28. Retrieved 2017-09-26.
- ↑ Ryeom S, Folkman J (March 2009). "Role of endogenous angiogenesis inhibitors in Down syndrome". The Journal of Craniofacial Surgery. 20 Suppl 1 (Suppl 1): 595–6. doi:10.1097/SCS.0b013e3181927f47. PMID 19795527. S2CID 21576950.
- ↑ Gooyer, Tanyth E. de; Stevenson, Kathryn A.; Humphries, Pete; Simpson, David A. C.; Gardiner, Tom A.; Stitt, Alan W. (2006-12-01). "Retinopathy Is Reduced during Experimental Diabetes in a Mouse Model of Outer Retinal Degeneration". Investigative Ophthalmology & Visual Science. 47 (12): 5561–5568. doi:10.1167/iovs.06-0647. ISSN 1552-5783. Archived from the original on 2018-07-23. Retrieved 2022-06-29.
- 1 2 3 Forrest, Iain S; Chaudhary, Kumardeep; Paranjpe, Ishan; et al. (2021-03-10). "Genome-wide polygenic risk score for retinopathy of type 2 diabetes". Human Molecular Genetics. 30 (10): 952–960. doi:10.1093/hmg/ddab067. ISSN 0964-6906. PMC 8165647. PMID 33704450. Archived from the original on 2022-08-20. Retrieved 2022-06-29.
- 1 2 Xu H, Curtis T, Stitt A (13 August 2013). "Pathophysiology and Pathogenesis of Diabetic Retinopathy [internet]". Diapedia. 7104343513 (14). doi:10.14496/dia.7104343513.14. Archived from the original on 27 August 2016. Retrieved 26 August 2016.
- ↑ Pardianto G (2005). "Understanding diabetic retinopathy". Mimbar Ilmiah Oftalmologi Indonesia. 2: 65–6.
- ↑ Geraldes P, Hiraoka-Yamamoto J, Matsumoto M, Clermont A, Leitges M, Marette A, Aiello LP, Kern TS, King GL (November 2009). "Activation of PKC-delta and SHP-1 by hyperglycemia causes vascular cell apoptosis and diabetic retinopathy". Nature Medicine. 15 (11): 1298–306. doi:10.1038/nm.2052. PMC 3290906. PMID 19881493.
- ↑ Tarr JM, Kaul K, Chopra M, Kohner EM, Chibber R (2013). "Pathophysiology of diabetic retinopathy". ISRN Ophthalmology. 2013: 343560. doi:10.1155/2013/343560. PMC 3914226. PMID 24563789.
- ↑ Bek T (2010). "Experimental Approaches to Diabetic Retinopathy – Front Diabetes" (PDF). In Hammes HP, Porta M (eds.). Clinical Presentations and Pathological Correlates of Retinopathy. Karger.com. Vol. 20. Basel. pp. 1–19. Archived (PDF) from the original on 2016-03-05. Retrieved 2022-06-29.
- ↑ Mandecka A et al.:Abnormal retinal autoregulation is detected by provoked stimulation with flicker light in well-controlled patients with type 1 diabetes without retinopathy. Diabetes Res Clin Pract. 2009 Oct;86(1):51-5.
- ↑ Bettermann K, Slocomb J,Quillen D et al.: Impaired Retinal Vasoreactivity: An Early Marker of Stroke Risk in Diabetes. J Neuroimaging 2017;27:78-84.
- ↑ Khansari MM, Wanek J, Tan M, Joslin CE, Kresovich JK, Camardo N, Blair NP, Shahidi M (April 2017). "Assessment of Conjunctival Microvascular Hemodynamics in Stages of Diabetic Microvasculopathy". Scientific Reports. 7: 45916. Bibcode:2017NatSR...745916K. doi:10.1038/srep45916. PMC 5384077. PMID 28387229.
- ↑ Khansari MM, O'Neill W, Penn R, Chau F, Blair NP, Shahidi M (July 2016). "Automated fine structure image analysis method for discrimination of diabetic retinopathy stage using conjunctival microvasculature images". Biomedical Optics Express. 7 (7): 2597–606. doi:10.1364/BOE.7.002597. PMC 4948616. PMID 27446692.
- ↑ Catherine H, Wendy L (May 8, 2018). "Preventing blindness in sight". San Francisco Chronicle. p. D1.
- ↑ "Central Mersey Diabetic Retinopathy Screening Programme (NHS England), DRSS User Manual, 2009" (PDF). Archived from the original (PDF) on 2014-07-27. Retrieved 2014-07-25.
- ↑ "Diabetic eye screening – NHS Choices". NHS Choices. 12 July 2016. Archived from the original on 24 September 2017. Retrieved 29 June 2022.
- ↑ Solomon SD, Chew E, Duh EJ, Sobrin L, Sun JK, VanderBeek BL, Wykoff CC, Gardner TW (March 2017). "Diabetic Retinopathy: A Position Statement by the American Diabetes Association". Diabetes Care. 40 (3): 412–418. doi:10.2337/dc16-2641. PMC 5402875. PMID 28223445.
- ↑ "Diabetic eye screening". 2017-10-18. Archived from the original on 2018-11-02. Retrieved 2022-06-29.
- ↑ Gupta A, Cavallerano J, Sun JK, Silva PS (17 October 2016). "Evidence for Telemedicine for Diabetic Retinal Disease". Seminars in Ophthalmology. 32 (1): 22–28. doi:10.1080/08820538.2016.1228403. PMID 27748634. S2CID 1335693.
- ↑ 1. Nsiah-Kumi, P., Ortmeier, S. R., & Brown, A. E. (2009). Disparities in Diabetic Retinopathy Screening and Disease for Racial and Ethnic Minority Populations—A Literature Review. Journal of the National Medical Association, 101(5), 430–438. doi: 10.1016/s0027-9684(15)30929-9
- ↑ Lawrenson JG, Graham-Rowe E, Lorencatto F, Burr J, Bunce C, Francis JJ, et al. (Cochrane Eyes and Vision Group) (January 2018). "Interventions to increase attendance for diabetic retinopathy screening". The Cochrane Database of Systematic Reviews. 1: CD012054. doi:10.1002/14651858.CD012054.pub2. PMC 6491139. PMID 29333660.
- 1 2 Mitchell P, Wong TY (March 2014). "Management paradigms for diabetic macular edema". American Journal of Ophthalmology. 157 (3): 505–13.e1–8. doi:10.1016/j.ajo.2013.11.012. PMID 24269850.
- ↑ "Facts About Diabetic Eye Disease | National Eye Institute". nei.nih.gov. Archived from the original on 2018-12-28. Retrieved 2016-07-18.
- ↑ Zhang HW, Zhang H, Grant SJ, Wan X, Li G, et al. (Cochrane Eyes and Vision Group) (December 2018). "Single herbal medicine for diabetic retinopathy". The Cochrane Database of Systematic Reviews. 2018 (12): CD007939. doi:10.1002/14651858.CD007939.pub2. PMC 6517038. PMID 30566763.
- ↑ Masharani U (2006). "Diabetes Ocular complications". Chronic Complications of Diabetes. Armenian Medical Network. Archived from the original on 2018-12-28. Retrieved 2022-06-29.
- ↑ "Diabetes and Vision". News-Medical.net. 2018-04-04. Archived from the original on 2018-04-10. Retrieved 2018-04-10.
- ↑ Hooper P, Boucher MC, Cruess A, Dawson KG, Delpero W, Greve M, Kozousek V, Lam WC, Maberley DA (April 2012). "Canadian Ophthalmological Society evidence-based clinical practice guidelines for the management of diabetic retinopathy". Canadian Journal of Ophthalmology. 47 (2 Suppl): S1–30, S31–54. doi:10.1016/j.jcjo.2011.12.025. PMID 22632804.
- ↑ Fraser-Bell S, Kaines A, Hykin PG (May 2008). "Update on treatments for diabetic macular edema". Current Opinion in Ophthalmology. 19 (3): 185–9. doi:10.1097/ICU.0b013e3282fb7c45. PMID 18408491. S2CID 37511491.
- ↑ Jorge EC, Jorge EN, Botelho M, Farat JG, Virgili G, El Dib R, et al. (Cochrane Eyes and Vision Group) (October 2018). "Monotherapy laser photocoagulation for diabetic macular oedema". The Cochrane Database of Systematic Reviews. 2018 (10): CD010859. doi:10.1002/14651858.CD010859.pub2. PMC 6516994. PMID 30320466.
- ↑ Moutray T, Evans JR, Lois N, Armstrong DJ, Peto T, Azuara-Blanco A (March 2018). "Different lasers and techniques for proliferative diabetic retinopathy". The Cochrane Database of Systematic Reviews. 2018 (3): CD012314. doi:10.1002/14651858.cd012314.pub2. PMC 6494342. PMID 29543992.
- ↑ Amoroso F, Pedinielli A, Astroz P, Semoun O, Capuano V, Miere A, Souied EH (November 2019). "Comparison of pain experience and time required for pre-planned navigated peripheral laser versus conventional multispot laser in the treatment of diabetic retinopathy". Acta Diabetologica. 57 (5): 535–541. doi:10.1007/s00592-019-01455-x. PMID 31749047. S2CID 208172191.
- ↑ Chhablani J, Mathai A, Rani P, Gupta V, Arevalo JF, Kozak I (May 2014). "Comparison of conventional pattern and novel navigated panretinal photocoagulation in proliferative diabetic retinopathy". Investigative Ophthalmology & Visual Science. 55 (6): 3432–8. doi:10.1167/iovs.14-13936. PMID 24787564.
- 1 2 Rittiphairoj, Thanitsara; Mir, Tahreem A.; Li, Tianjing; Virgili, Gianni (November 17, 2020). "Intravitreal steroids for macular edema in diabetes". The Cochrane Database of Systematic Reviews. 2020 (11): CD005656. doi:10.1002/14651858.CD005656.pub3. ISSN 1469-493X. PMC 8095060. PMID 33206392.
- ↑ O'Malley PG (July 2012). "Comparative effectiveness of anti-growth factor therapies for diabetic macular edema: summary of primary findings and conclusions". Archives of Internal Medicine. 172 (13): 1014–5. doi:10.1001/archinternmed.2012.2335. PMID 22688778.
- ↑ Virgili, Gianni; Parravano, Mariacristina; Evans, Jennifer R.; Gordon, Iris; Lucenteforte, Ersilia (16 October 2018). "Anti-vascular endothelial growth factor for diabetic macular oedema: a network meta-analysis". The Cochrane Database of Systematic Reviews. 10: CD007419. doi:10.1002/14651858.CD007419.pub6. ISSN 1469-493X. PMC 6517135. PMID 30325017.
- ↑ Antoszyk AN, et al. (December 2020). "Effect of intravitreous aflibercept vs vitrectomy with panretinal photocoagulation on visual acuity in patients with vitreous hemorrhage from proliferative diabetic retinopathy". Journal of the American Medical Association. 324 (23): 2383–95. doi:10.1001/jama.2020.23027. PMC 7739132. PMID 33320223.
- ↑ Seah, Ivan (January 30, 2020). "Use of biomaterials for sustained delivery of anti-VEGF to treat retinal diseases". Eye. 34 (8): 1341–1356. doi:10.1038/s41433-020-0770-y. PMC 7376230. PMID 32001821.
- ↑ Sahoo S, Barua A, Myint KT, Haq A, Abas AB, Nair NS, et al. (Cochrane Eyes and Vision Group) (February 2015). "Topical non-steroidal anti-inflammatory agents for diabetic cystoid macular oedema". The Cochrane Database of Systematic Reviews (2): CD010009. doi:10.1002/14651858.CD010009.pub2. PMID 25686158.
- ↑ Smith JM, Steel DH (August 2015). "Anti-vascular endothelial growth factor for prevention of postoperative vitreous cavity haemorrhage after vitrectomy for proliferative diabetic retinopathy". The Cochrane Database of Systematic Reviews (8): CD008214. doi:10.1002/14651858.cd008214.pub3. PMC 6599827. PMID 26250103.
- 1 2 3 Sivaprasad S, Arden G (February 2016). "Spare the rods and spoil the retina: revisited". Eye. 30 (2): 189–92. doi:10.1038/eye.2015.254. PMC 4763134. PMID 26656085.
- ↑ "Noctura 400 Sleep Mask for diabetic retinopathy". NIHR Innovation Observatory. Archived from the original on 2022-02-15. Retrieved 2022-02-15.
- ↑ Powell, Selina. "No "long-term therapeutic benefit" from £250 mask". www.aop.org.uk. Archived from the original on 2021-07-25. Retrieved 2022-02-15.
- ↑ Bhatt MP, Lim YC, Ha KS (November 2014). "C-peptide replacement therapy as an emerging strategy for preventing diabetic vasculopathy". Cardiovascular Research. 104 (2): 234–44. doi:10.1093/cvr/cvu211. PMID 25239825.
- ↑ "C-peptide - Creative Peptides -". AdisInsight. Archived from the original on 13 September 2018. Retrieved 22 October 2016.
- ↑ "C-peptide – Eli Lilly". AdisInsight. Archived from the original on 12 September 2018. Retrieved 22 October 2016.
- ↑ "C-peptide long-acting – Cebix". adisinsight.springer.com. AdisInsight. Archived from the original on 16 November 2018. Retrieved 22 October 2016.
- ↑ Bigelow BV (23 February 2015). "Cebix Shuts Down Following Mid-Stage Trial of C-Peptide Drug". Xconomy. Archived from the original on 28 December 2018. Retrieved 29 June 2022.
- ↑ Garde D (February 24, 2015). "Cebix hangs it up after raising $50M for diabetes drug". FierceBiotech. Archived from the original on September 13, 2018. Retrieved June 29, 2022.
- ↑ Ljubimov A. "Stem Cell Therapy for Diabetic Retinopathy" (PDF). Cedars-Sinai Medical Center, Regenerative Medicine Institute, Los Angeles, CA, USA Medicine, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA. Archived from the original (PDF) on 2014-12-30. Retrieved 2014-12-30.
- 1 2 Do DV, Wang X, Vedula SS, Marrone M, Sleilati G, Hawkins BS, Frank RN (January 2015). "Blood pressure control for diabetic retinopathy". The Cochrane Database of Systematic Reviews. 1: CD006127. doi:10.1002/14651858.CD006127.pub2. PMC 4439213. PMID 25637717.
- 1 2 Ahmad A, Mansoor AB, Mumtaz R, Khan M, Mirza SH (2014-12-01). "Image processing and classification in diabetic retinopathy: A review". 2014 5th European Workshop on Visual Information Processing (EUVIP): 1–6. doi:10.1109/EUVIP.2014.7018362. ISBN 978-1-4799-4572-6. S2CID 16465894.
- ↑ "Diabetic Retinopathy". Merck Manuals Professional Edition. Archived from the original on 2016-11-27. Retrieved 2016-11-13.
- ↑ Kaur M, Talwar R (2014). "Review on: Blood Vessel Extraction and Eye Retinopathy Detection". International Journal of Computer Science and Information Technologies. 5 (6): 7513–7516.
- ↑ Grossman S. "A New Treatment for Diabetic Retinopathy". Diabetescare.net. Diabetescare.net. Archived from the original on 15 March 2015. Retrieved 19 March 2015.
![]() This article incorporates text from a publication in the public domain: "Facts About Diabetic Retinopathy". National Eye Institute, National Institutes of Health (NEI/NIH). June 2012. Archived from the original on 12 May 2014. Retrieved 13 June 2002.
This article incorporates text from a publication in the public domain: "Facts About Diabetic Retinopathy". National Eye Institute, National Institutes of Health (NEI/NIH). June 2012. Archived from the original on 12 May 2014. Retrieved 13 June 2002.
Further reading
- Solomon SD, Chew E, Duh EJ, Sobrin L, Sun JK, VanderBeek BL, Wykoff CC, Gardner TW (March 2017). "Diabetic Retinopathy: A Position Statement by the American Diabetes Association". Diabetes Care. 40 (3): 412–418. doi:10.2337/dc16-2641. PMC 5402875. PMID 28223445.
External links
- Diabetic retinopathy Archived 2019-09-12 at the Wayback Machine resource guide courtesy of National Eye Institute, National Institutes of Health (NEI/NIH)
- Diabetic Eye Disease Archived 2022-06-13 at the Wayback Machine National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health (NIDDK/NIH)
- NHS Diabetic Eye Screening Programme Archived 2022-08-08 at the Wayback Machine
| Classification | |
|---|---|
| External resources |