Ipilimumab
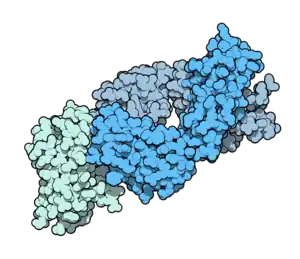 Fab fragment of ipilimumab (blue) binding CTLA-4 (green). From PDB entry 5TRU. | |
| Monoclonal antibody | |
|---|---|
| Type | Whole antibody |
| Source | Human |
| Target | CTLA-4 |
| Names | |
| Pronunciation | i pi lim′ ue mab |
| Trade names | Yervoy |
| Other names | BMS-734016,[1] MDX-010,[2] MDX-101 |
| Clinical data | |
| Main uses | Melanoma, renal cell cancer, mesothelioma, non-small cell lung cancer (NSCLC)[3][4] |
| Side effects | Rash, itchiness, tiredness, diarrhea, nausea, fever, thyroid problems, shortness of breath, liver inflammation, abdominal pain[4] |
| WHO AWaRe | UnlinkedWikibase error: ⧼unlinkedwikibase-error-statements-entity-not-set⧽ |
| Pregnancy category |
|
| Routes of use | Intravenous (IV) |
| External links | |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a611023 |
| Legal | |
| License data |
|
| Legal status | |
| Chemical and physical data | |
| Formula | C6742H9972N1732O2004S40 |
| Molar mass | 148634.46 g·mol−1 |
Ipilimumab, sold under the brand name Yervoy, is a medication used to treat melanoma, renal cell cancer, mesothelioma, and non-small cell lung cancer (NSCLC).[3][4] It is often used together with nivolumab.[4] It is given by gradual injection into a vein.[4]
Common side effects include rash, itchiness, tiredness, diarrhea, nausea, fever, thyroid problems, shortness of breath, liver inflammation, and abdominal pain.[4] Other side effects may include intestinal inflammation, toxic epidermal necrolysis, and neuropathy.[3] It is a monoclonal antibody that attaches to and blocks CTLA-4 which increases T cell activity against cancer.[4]
Ipilimumab was approved for medical use in the United States and Europe in 2011.[4][3] In the United Kingdom it costs about £15,000 for 200 mg as of 2021.[8] In the United States this amount costs about 32,300 USD.[9]
Medical uses
Ipilimumab is used to treat late-stage melanoma that has spread or cannot be removed by surgery.[10][11][12][13][14] It was later approved for stage 3 as adjuvant therapy.[15] On February 1, 2012, Health Canada approved ipilimumab for "treatment of unresectable or metastatic melanoma in patients who have failed or do not tolerate other systemic therapy for advanced disease."[16] Ipilimumab was approved in the European Union (EU), for second line treatment of metastatic melanoma in November 2012.[17][18]
Nivolumab, in combination with ipilimumab is indicated for the treatment of intermediate or poor risk, previously untreated advanced renal cell cancer.[6][19]
Ipilimumab, in combination with nivolumab, is indicated for the treatment of adults and adolescents twelve years and older with microsatellite instability-high or mismatch repair deficient metastatic colorectal cancer that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan.[6][20]
Ipilimumab, in combination with nivolumab, is indicated for the treatment of people with hepatocellular carcinoma who have been previously treated with sorafenib.[6][21]
Ipilimumab, in combination with nivolumab, is indicated for the first-line treatment of adults with metastatic non-small cell lung cancer (NSCLC) whose tumors express PD-L1 (≥1%) as determined by an FDA-approved test.[6][22][23]
In October 2020, the U.S. Food and Drug Administration (FDA) approved the combination of nivolumab with ipilimumab for the first-line treatment of adults with malignant pleural mesothelioma that cannot be removed by surgery.[24] This is the first drug regimen approved for mesothelioma in sixteen years and the second FDA-approved systemic therapy for mesothelioma.[24]
Likely to respond
During “cancer immunoediting", tumor cells can produce antigens that provoke a reduced immune response and/or establish an immunosuppressive tumor microenvironment (TME). The latter can arise as a consequence of repeated, ineffective T cell stimulation. This triggers the checkpoint that ipilumumab targets. Many patients do not benefit from treatment, which may be related to reduced mutation load and/or missense point mutation-derived neoantigens.[10] Tumor antigens can either be improperly expressed normal proteins or abnormal proteins with tumor-specific expression. Somatic cancer mutations can produce “nonself” tumor-specific mutant antigens (neoantigens).[25]
Sequencing and epitope prediction algorithms identified neoantigens in mouse tumors that functioned as tumor-specific T cell targets. Neoantigens were recognized by T cells in melanoma patients and were likely the major contributor to positive clinical effects of adoptive cell transfer. Mouse models established that neoantigens were the targets of T cells activated by checkpoint blockade therapy and that synthetic long peptides comprising these neoantigens were effective when administered as vaccines with CTLA-4 and/or PD-1 mAbs. Cancers with higher mutation burdens, and an associated likelihood of expressing neoantigens, appear most likely to respond to checkpoint therapy.[10] In melanoma and certain other cancers, the numbers of mutations and neoantigens correlate with patient response. Increased PD ligand 2 (PD-L2) transcript expression and an immune “cytolytic” gene signature also correlated with neoantigen load and tumor response. CTLA-4 expression was a response indicator, which along with PD-L2 were likely expressed in tumor-infiltrating immune cells. An inflamed TME prior to treatment is also associated with response.[25]
Nearly all neoantigens in one study were patient-specific and most likely reflected mutations that do not directly contribute to tumorigenesis. However, none revealed features or motifs exclusive to responders.[25]
Dosage
It may be used at a dose of 3 mg/kg every 21 days for four doses by itself in melanoma.[8]
Side effects
A major drawback of ipilimumab therapy is its association with severe and potentially fatal immunological adverse effects due to T cell activation and proliferation, occurring in ten to twenty percent of patients.[26] Serious adverse effects include stomach pain, bloating, constipation, diarrhea, fever, trouble breathing, and urinating problems. A "risk evaluation and mitigation strategy" informs prescribers of the potential risks.[14][27]
Between 5.7 and 9.1% of individuals treated with ipilimumab develop checkpoint inhibitor induced colitis.[28]
Individual cases of severe neurologic disorders following ipilimumab have been observed, including acute inflammatory demyelination polyneuropathy and an ascending motor paralysis, and myasthenia gravis.[29]
Interactions
The combination of ipilimumab with either leflunomide or vemurafenib may lead to increased hepatotoxicity.[30][31][32][33]
Systemic corticosteroids should be avoided before starting ipilimumab; however, systemic corticosteroids may be used to treat an immune-related adverse reaction that arises from ipilimumab treatment.[34]
Patients taking anticoagulants with ipilimumab should be monitored due to an increased risk of gastrointestinal bleeding.[34]
Mechanism of action
T lymphocytes can recognize and destroy cancer cells. However, an inhibitory mechanism interrupts this destruction. Ipilimumab turns off this inhibitory mechanism and allows the lymphocytes to continue to destroy cancer cells.[35]
Cancer cells produce antigens, which the immune system can use to identify them. These antigens are recognized by dendritic cells that present the antigens to cytotoxic T lymphocytes (CTLs) in the lymph nodes. The CTLs recognize the cancer cells by those antigens and destroy them. However, along with the antigens, the dendritic cells present an inhibitory signal. That signal binds to a receptor, cytotoxic T lymphocyte-associated antigen 4 (CTLA-4), on the CTL and turns off the cytotoxic reaction. This allows the cancer cells to survive.[35]
Ipilimumab binds to CTLA-4, blocking the inhibitory signal, which allows the CTLs to destroy the cancer cells.[35][36][37][38][39][40][41] In 2014 a study indicated that the antibody works by allowing the patients' T cells to target a greater variety of antigens rather than by increasing the number attacking a single antigen.[42]
History
The concept of using anti-CTLA4 antibodies to treat cancer was first developed by James P. Allison while he was director of the Cancer Research Laboratory at the University of California, Berkeley.[43][44] Clinical development of anti-CTLA4 was initiated by Medarex, which was later acquired by Bristol-Myers Squibb. For his work in developing ipilimumab, Allison was awarded the Lasker Award in 2015.[45] Allison later was the co-winner of the 2018 Nobel Prize in Physiology or Medicine.[46]
Following the 1987 cloning of CTLA-4 in mice,[47] its conservation in humans and similarities with CD28 were soon noticed.[48] CD28 at that time was a recently identified "T cell costimulatory" molecule important for T cell activation.[49] Anti-CTLA-4 blockade, the invention that gave rise to ipilimumab, was conceived by Allison and Krummel along with CTLA-4's inhibitory role in T cell activation.[50] They were able to demonstrate that CTLA-4 signaling in T cells inhibited T cell responses.[51] They then injected intact antibodies and demonstrated that CTLA-4 blockade enhanced T cell responses in mice responding to vaccines and to super antigens.[52] Leach, a new postdoctoral fellow, was tasked by Allison with applying these in tumor models. Antibody-treated mice showed significantly less cancer growth than the controls.[53]
Bluestone and Linsley separately studied the similarities between CD28 and CTLA-4. Bluestone's lab published studies, one together with Krummel and Allison, for in vitro studies of CTLA-4 function.[54][55] In collaboration with Mark Jenkins, they were able to see effects of anti-CTLA-4 antibodies in vivo in an immunization setting,[56] but did not effectively carry this into tumor biology. Linsley and colleagues had made antibodies against CTLA-4 three years prior to those of Krummel/Allison or Walunas/Bluestone. They concluded that the molecule functioned similarly to CD28 and was a "positive costimulator".[57] They apparently did not pursue CTLA-4 tumor targeting, although BMS licensed the Allison/Leach/Krummel patent through their acquisition of Medarex and the fully humanized antibody MDX010, which later became ipilimumab.
Research
In the 2000s, ipilimumab clinical trials were under way on patients with melanoma, renal cell carcinoma, prostate cancers, urothelial carcinoma and ovarian cancer.[58] By 2007, there were two fully human anti CTLA-4[59] monoclonal antibodies in advanced clinical trials. Ipilimumab, which is an IgG1 isotype, and tremelimumab (from Pfizer) which is an IgG2 isotype.[60][61]
Melanoma
On December 10, 2007, Bristol-Myers Squibb and Medarex released the results of three studies on ipilimumab for melanoma.[62] The three studies tested 487 patients with advanced skin cancer. One of the three studies failed to meet its primary goal of shrinking tumors in at least 10.0% of the study's 155 patients. Side effects included rashes, diarrhea, and hepatitis.
In 2010, a study was presented that showed a median survival of ten months in advanced melanoma patients treated with ipilimumab, compared with 6.4 months for those treated with gp100, an experimental vaccine (n=676), and 10.1 months for those treated with both the vaccine and ipilimumab.[63] The Phase III clinical studies on the drug were controversial for their unconventional use of a control arm (as opposed to using a placebo or standard treatment). Ipilimumab gained FDA approval in March 2011.[11][12]
To increase response rate and reduce adverse reactions, various drug combinations are being tested.
In 2013, a trial was running that compared ipilimumab alone against ipilimumab in combination with nivolumab. The response rate (tumours shrinking by at least 30%) was 58% for the combination, 44% for nivolumab alone, and 19% for ipilimumab alone.[64] This combination gained FDA approval for melanoma in Oct 2015.
In March 2014, an open-label, randomized, two agent, single center trial started combining ipilimumab with phosphatidylserine-targeting immunotherapy bavituximab for the treatment of advanced melanoma. The number of treated patients in arm A (ipilimumab plus bavituximab) was to be 16, with 8 in arm B (ipilimumab only). [65] The trial was terminated in April 2016 due to low enrollment.[66] Previous, preclinical studies showed that PS targeting antibodies (such as bavituximab) enhance the anti-tumor activity of anti-CTLA-4 and anti-PD-1 antibodies. Tumor growth inhibition correlates with infiltration of immune cells in tumors and induction of adaptive immunity. The combination of these mechanisms promotes strong, localized, anti-tumor responses without the side-effects of systemic immune activation.[67]
Prostate cancer
In 2008/09 Medarex performed a phase I/II dose escalation clinical trial of ipilimumab in metastatic hormone-refractory prostate cancer (HRPC). Some of the patients with advanced prostate cancer had their tumors drastically shrink, promoting further trials.[68]
On June 19, 2009, the Mayo Clinic reported two prostate cancer patients involved in a phase II study using MDX-010 therapy who had been told initially that their condition was inoperable but had their tumors shrunk by the drug such that operation was possible and are now cancer-free as a result.[69] This press report however was criticized as premature and somewhat inaccurate. The clinical trials were still at an early stage and were run alongside other treatments – which could have been the real explanation for the tumor shrinkage.[70] It was too early to say whether ipilimumab made any difference.[71]
In 2016, a phase II study using ipilimumab and nivolumab in AR-V7-expressing metastatic castration-resistant prostate cancer was opened.[72][73] AR-V7 is an androgen receptor splice variant that can be detected in circulating tumor cells of metastatic prostate cancer patients.[73][74]
Lung cancer
CHECKMATE-227 [75] tested the combination of nivolumab and ipilimumab in patients with stage IV or recurrent NSCLC without previous treatment.[76][75] Patients with a PD-L1 expression level of 1% or more were randomized in a 1:1:1 ratio to receive nivolumab plus ipilimumab, nivolumab alone, or chemotherapy.[76][75] The chemotherapy used was Cisplatin or Carboplatin, combined with Gemcitabine for patient with squamous cell NSCLC, or pemetrexed for patients with nonsquamous disease.[76][75] The overall survival was 17.1, 15.7 and 14.9 months, respectively.[76][75] The patients who had a PD-L1 expression level of less than 1% were randomly assigned in a 1:1:1 ratio to receive nivolumab plus ipilimumab, nivolumab plus chemotherapy, or chemotherapy.[76][75] The OS was 17.2, 15.2 and 12.2 months, respectively.[76][75]
CHECKMATE-9LA [77] randomized patients with stage IV NSCLC, to nivolumab 360 mg Q3W + ipilimumab 1 mg/kg Q6W + two cycles of chemotherapy or 4 cycles of chemotherapy alone.[76] The chemotherapy used was Cisplatin or Carboplatin combined with Pemetrexed or Paclitaxel. The data were presented in an abstract format and as a lecture during the American Society of Clinical Oncology (ASCO) 2020 annual meeting.[77] Median OS was 15.6 and 10.9 months, in the immunotherapy-chemotherapy and the chemotherapy only groups, respectively.[77][76]
Urinary tract cancer
A Phase 2 clinical trial entitled First-Line Gemcitabine, Cisplatin + Ipilimumab for Metastatic Urothelial Carcinoma Archived 2021-02-05 at the Wayback Machine was first reported in 2015 [78] Thirty-six patients were treated with chemotherapy, adding ipilimumab after the second 21-day cycle. Though the study did not meet its primary endpoint, a significant expansion of circulating CD4 cells was noted upon addition of ipilimumab, which correlated with improved survival, especially in patients with deleterious somatic DNA damage response mutations. [79]
References
- ↑ "Yervoy, ipilimumab (BMS-734016) - Product Profile - BioCentury". BioCentury Online Intelligence. BioCentury Publications. Archived from the original on 12 August 2016. Retrieved 11 August 2016.
- ↑ USAN. "STATEMENT ON A NONPROPRIETARY NAME ADOPTED BY THE USAN COUNCIL - ipilimumab" (Press release). American Medical Association (AMA). Archived from the original on 2016-02-23. Retrieved 2013-01-12.
- 1 2 3 4 "Ipilimumab Monograph for Professionals". Drugs.com. Archived from the original on 6 May 2021. Retrieved 28 November 2021.
- 1 2 3 4 5 6 7 8 "Yervoy". Archived from the original on 28 September 2020. Retrieved 28 November 2021.
- ↑ "Yervoy 5 mg/ml concentrate for solution for infusion - Summary of Product Characteristics (SmPC)". (emc). 3 August 2020. Archived from the original on 22 January 2021. Retrieved 2 October 2020.
- 1 2 3 4 5 "Yervoy- ipilimumab injection". DailyMed. 13 August 2020. Archived from the original on 4 August 2020. Retrieved 2 October 2020.
- ↑ "Yervoy EPAR". European Medicines Agency (EMA). Archived from the original on 28 September 2020. Retrieved 2 October 2020.
- 1 2 BNF 81: March-September 2021. BMJ Group and the Pharmaceutical Press. 2021. p. 918. ISBN 978-0857114105.
- ↑ "Yervoy Prices, Coupons & Patient Assistance Programs". Drugs.com. Archived from the original on 22 January 2021. Retrieved 28 November 2021.
- 1 2 3 Syn NL, Teng MW, Mok TS, Soo RA (December 2017). "De-novo and acquired resistance to immune checkpoint targeting". The Lancet Oncology. 18 (12): e731–e741. doi:10.1016/s1470-2045(17)30607-1. PMID 29208439.
- 1 2 "Drug Approval Package: Yervoy (ipilimumab) Injection NDA #125377". U.S. Food and Drug Administration (FDA). 24 December 1999. Archived from the original on 3 November 2020. Retrieved 2 October 2020.
- 1 2 "FDA approves new treatment for a type of late-stage skin cancer" (Press release). U.S. Food and Drug Administration (FDA). 2011-03-25. Archived from the original on 2011-03-27. Retrieved 2011-03-25.
- ↑ Pollack A (2011-03-25). "Approval for Drug That Treats Melanoma". The New York Times. Archived from the original on 2011-04-01. Retrieved 2011-03-27.
- 1 2 Drugs.com: Yervoy Archived 2011-08-09 at the Wayback Machine
- ↑ "FDA approves Yervoy to reduce the risk of melanoma returning after surgery" (Press release). U.S. Food and Drug Administration (FDA). 28 October 2015. Archived from the original on 2015-10-29. Retrieved 2019-04-08.
- ↑ "First an only treatment to extend survival for people with metastatic melanoma, the most deadly form of skin cancer, approved in Canada" (Press release). Bristol-Myers Squibb. 7 February 2012. Archived from the original on 2019-04-08. Retrieved 2019-04-08.
- ↑ "Bristol-Myers Squibb Receives Positive Decision from National Institute of Health and Clinical Excellence (NICE) for Yervoy (ipilimumab)" (Press release). November 1, 2012. Archived from the original on February 5, 2017. Retrieved December 17, 2012.
- ↑ Maverakis E, Cornelius LA, Bowen GM, Phan T, Patel FB, Fitzmaurice S, He Y, Burrall B, Duong C, Kloxin AM, Sultani H, Wilken R, Martinez SR, Patel F (2015). "Metastatic melanoma - a review of current and future treatment options". Acta Derm Venereol. 95 (5): 516–524. doi:10.2340/00015555-2035. PMID 25520039.
- ↑ "FDA approves nivolumab plus ipilimumab combination for intermediate or poor-risk advanced renal cell carcinoma". U.S. Food and Drug Administration (FDA). 16 April 2018. Archived from the original on 12 March 2020. Retrieved 2 October 2020.
 This article incorporates text from this source, which is in the public domain.
This article incorporates text from this source, which is in the public domain. - ↑ "FDA grants accelerated approval to ipilimumab for MSI-H or dMMR metastatic colorectal cancer". U.S. Food and Drug Administration (FDA). 10 July 2018. Archived from the original on 29 October 2020. Retrieved 2 October 2020. This article incorporates text from this source, which is in the public domain.
- ↑ "FDA grants accelerated approval to nivolumab and ipilimumab combination for hepatocellular carcinoma". U.S. Food and Drug Administration (FDA). 10 March 2020. Archived from the original on 25 September 2020. Retrieved 2 October 2020. This article incorporates text from this source, which is in the public domain.
- ↑ "FDA approves nivolumab plus ipilimumab for first-line mNSCLC (PD-L1 tumor expression ≥1%)". U.S. Food and Drug Administration (FDA). 15 May 2020. Archived from the original on 20 October 2020. Retrieved 2 October 2020. This article incorporates text from this source, which is in the public domain.
- ↑ "FDA approves nivolumab plus ipilimumab and chemotherapy for first-line treatment of metastatic NSCLC". U.S. Food and Drug Administration (FDA). 26 May 2020. Archived from the original on 24 September 2020. Retrieved 2 October 2020. This article incorporates text from this source, which is in the public domain.
- 1 2 "FDA Approves Drug Combination for Treating Mesothelioma". U.S. Food and Drug Administration (FDA) (Press release). 2 October 2020. Archived from the original on 4 October 2020. Retrieved 2 October 2020. This article incorporates text from this source, which is in the public domain.
- 1 2 3 Gubin, Matthew M.; Schreiber, Robert D. (2015-10-09). "The odds of immunotherapy success". Science. 350 (6257): 158–159. Bibcode:2015Sci...350..158G. doi:10.1126/science.aad4140. ISSN 0036-8075. PMID 26450194. S2CID 206643238.
- ↑ Johnson DB, Peng C, Sosman JA (2015). "Nivolumab in melanoma: latest evidence and clinical potential". Ther Adv Med Oncol. 7 (2): 97–106. doi:10.1177/1758834014567469. PMC 4346215. PMID 25755682.
- ↑ "FDA Rubber-Stamps Bristol-Myers Squibb's Melanoma mAb". Genetic Engineering & Biotechnology News. 2011-03-28. Archived from the original on 2011-04-01. Retrieved 2011-03-28.
- ↑ Bellaguarda, Emanuelle; Hanauer, Stephen (February 2020). "Checkpoint Inhibitor–Induced Colitis". The American Journal of Gastroenterology. 115 (2): 202–210. doi:10.14309/ajg.0000000000000497. PMID 31922959.
- ↑ "Two Cases of Myasthenia Gravis Seen With Ipilimumab". 2014-04-29. Archived from the original on 2021-10-31. Retrieved 2021-08-01.
- ↑ "Arava (leflunomide) [package insert]" (PDF). Australia: Sanofi-Aventis, July 2014. Archived from the original (PDF) on 2 November 2014. Retrieved 2 November 2014.
- ↑ Ribas, Antoni; Hodi, F. Stephen; Callahan, Margaret; Konto, Cyril; Wolchok, Jedd (April 4, 2013). "Hepatotoxicity with combination of vemurafenib and ipilimumab". N Engl J Med. 368 (14): 1365–6. doi:10.1056/NEJMc1302338. PMID 23550685.
- ↑ "Zelboraf (vemurafenib) [package insert]" (PDF). South San Francisco, CA: Genentech USA, Inc.; March 2013. Archived (PDF) from the original on 31 October 2014. Retrieved 29 October 2014.
- ↑ "Yervoy (ipilimumab) [package insert]" (PDF). Princeton, NJ: Bristol-Myers Squibb Company; Dec 2013. Archived from the original (PDF) on 6 February 2015. Retrieved 29 October 2014.
- 1 2 "Yervoy Annex I: Summary of Product Characteristics" (PDF). Archived (PDF) from the original on 20 December 2014. Retrieved 2 November 2014.
- 1 2 3 Antoni Ribas (28 June 2012). "Tumor immunotherapy directed at PD-1". New England Journal of Medicine. 366 (26): 2517–9. doi:10.1056/nejme1205943. PMID 22658126.
- ↑ Tarhini AA, Iqbal F (2010). "CTLA-4 blockade: therapeutic potential in cancer treatments". OncoTargets Ther. 3: 15–25. doi:10.2147/ott.s4833. PMC 2895779. PMID 20616954.
- ↑ Robert C, Ghiringhelli F (August 2009). "What is the role of cytotoxic T lymphocyte-associated antigen 4 blockade in patients with metastatic melanoma?". Oncologist. 14 (8): 848–61. doi:10.1634/theoncologist.2009-0028. PMID 19648604.
- ↑ Gail M. Wilkes; Margaret Barton-Burke (11 December 2009). 2010 oncology nursing drug handbook. Jones & Bartlett Learning. pp. 1–. ISBN 978-0-7637-8124-8. Archived from the original on 16 June 2013. Retrieved 30 March 2011.
- ↑ L. Harivardhan Reddy; Patrick Couvreur (1 June 2009). Macromolecular Anticancer Therapeutics. Springer. pp. 522–. ISBN 978-1-4419-0506-2. Archived from the original on 16 June 2013. Retrieved 30 March 2011.
- ↑ Zhiqiang An (8 September 2009). Therapeutic Monoclonal Antibodies: From Bench to Clinic. John Wiley and Sons. pp. 134–. ISBN 978-0-470-11791-0. Archived from the original on 12 June 2013. Retrieved 30 March 2011.
- ↑ Ralph Blum; Mark Scholz (24 August 2010). Invasion of the Prostate Snatchers: No More Unnecessary Biopsies, Radical Treatment Or Loss of Sexual Potency. Other Press, LLC. pp. 227–. ISBN 978-1-59051-342-2. Retrieved 30 March 2011.
- ↑ Colmone, A. C. (2014). "Cancer immunotherapy expands T cell attack". Science. 345 (6203): 1463. Bibcode:2014Sci...345Q1463C. doi:10.1126/science.345.6203.1463-c.
- ↑ Leach DR, Krummel MF, Allison JP (1996). "Enhancement of antitumor immunity by CTLA-4 blockade". Science. 271 (5256): 1734–6. Bibcode:1996Sci...271.1734L. doi:10.1126/science.271.5256.1734. PMID 8596936. S2CID 7215817.
- ↑ "The Story of Yervoy (Ipilimumab)". Archived from the original on 2015-09-06. Retrieved 2021-08-01.
- ↑ Lasker Foundation. "Deep brain stimulation for Parkinson's disease". The Lasker Foundation. Archived from the original on 2016-02-07. Retrieved 2021-08-01.
- ↑ "The Nobel Prize in Physiology or Medicine 2018 to James P. Allison and Tasuku Honjo". Archived from the original on 2018-12-24. Retrieved 2021-08-01.
- ↑ Brunet JF, Denizot F, Luciani MF, Roux-Dosseto M, Suzan M, Mattei MG, Golstein P (Jul 1987). "A new member of the immunoglobulin superfamily--CTLA-4". Nature. 328 (6127): 267–70. Bibcode:1987Natur.328..267B. doi:10.1038/328267a0. PMID 3496540. S2CID 4316396.
- ↑ Harper K, Balzano C, Rouvier E, Mattéi MG, Luciani MF, Golstein P (Aug 1991). "CTLA-4 and CD28 activated lymphocyte molecules are closely related in both mouse and human as to sequence, message expression, gene structure, and chromosomal location". J Immunol. 147 (3): 1037–44. PMID 1713603.
- ↑ Harding F.; McArthur J.G.; Gross J.A.; Raulet D.H.; Allison J.P. (1992). "CD28 mediated signalling costimulates murine T cells and prevents the induction of anergy in T cell clones". Nature. 356 (6370): 607–609. Bibcode:1992Natur.356..607H. doi:10.1038/356607a0. PMID 1313950. S2CID 4333730.
- ↑ Krummel, M.F. (1995). Identification and Characterization of a CTLA-4 Dependent Regulatory Mechanism for T Cell Activation (University of California, Berkeley).
- ↑ Krummel M.F.; Allison J.P. (1995). "CD28 and CTLA-4 deliver opposing signals which regulate the response of T cells to stimulation". Journal of Experimental Medicine. 182 (2): 459–465. doi:10.1084/jem.182.2.459. PMC 2192127. PMID 7543139.
- ↑ Krummel M.F.; Sullivan T.J.; Allison J.P. (1995). "Superantigen responses and costimulation: CD28 and CTLA-4 have opposing effects on T cell expansion In Vitro and In Vivo". International Immunology. 8: 101–105.
- ↑ Leach D.R.; Krummel M.F.; Allison J.P. (1996). "Enhancement of antitumor immunity by CTLA-4 blockade". Science. 271 (5256): 1734–1736. Bibcode:1996Sci...271.1734L. doi:10.1126/science.271.5256.1734. PMID 8596936. S2CID 7215817.
- ↑ Walunas T.L.; Bakker C.Y.; Bluestone J.A. (1996). "CTLA-4 ligation blocks CD28-dependent T cell activation". Journal of Experimental Medicine. 183 (6): 2541–2550. doi:10.1084/jem.183.6.2541. PMC 2192609. PMID 8676075.
- ↑ Walunas T.L.; Lenschow D.J.; Bakker C.Y.; Linsley P.S.; Freeman G.J.; Green J.M.; Thompson C.B.; Bluestone J.A. (1994). "CTLA-4 can function as a negative regulator of T cell activation". Immunity. 1 (5): 405–413. doi:10.1016/1074-7613(94)90071-x. PMID 7882171.
- ↑ Kearney E.R.; Walunas T.L.; Karr R.W.; Morton P.A.; Loh D.Y.; Bluestone J.A.; Jenkins M.K. (1995). "Antigen-dependent clonal expansion of a trace population of antigen-specific CD4+ T cells in vivo is dependent on CD28 costimulation and inhibited by CTLA-4". J Immunol. 155 (3): 1032–1036. PMID 7543510.
- ↑ Linsley P.S.; Greene J.L.; Tan P.; Bradshaw J.; Ledbetter J.A.; Anasetti C.; Damle N.K. (1992). "Coexpression and functional cooperativity of CTLA-4 and CD28 on activated T lymphocytes". Journal of Experimental Medicine. 176 (6): 1595–1604. doi:10.1084/jem.176.6.1595. PMC 2119471. PMID 1334116.
- ↑ Sharma, Pamanee; Allison, James P. (April 3, 2015). "The future of immune checkpoint therapy". Science. 348 (6230): 56–61. Bibcode:2015Sci...348...56S. doi:10.1126/science.aaa8172. PMID 25838373. S2CID 4608450.
- ↑ "CTLA-4 strategies: Abatacept / Belatacept". healthvalue.net. Archived from the original on 2008-12-05. Retrieved 2009-06-24.
- ↑ Tomillero A, Moral MA (October 2008). "Gateways to clinical trials". Methods Find Exp Clin Pharmacol. 30 (8): 643–72. doi:10.1358/mf.2008.30.5.1236622. PMID 19088949.
- ↑ Poust J (December 2008). "Targeting metastatic melanoma". Am J Health Syst Pharm. 65 (24 Suppl 9): S9–S15. doi:10.2146/ajhp080461. PMID 19052265. S2CID 207291355.
- ↑ "Top-Line Data Available from Three Ipilimumab Pivotal Trials in Patients with Advanced Metastatic Melanoma". Medarex, Inc. 2007-12-10. Archived from the original on October 20, 2008. Retrieved 2009-06-24.
- ↑ Hodi, F. S.; O'Day, S. J.; McDermott, D. F.; Weber, R. W.; Sosman, J. A.; Haanen, J. B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J. C.; Akerley, W.; Van Den Eertwegh, A. J.; Lutzky, J.; Lorigan, P.; Vaubel, J. M.; Linette, G. P.; Hogg, D.; Ottensmeier, C. H.; Lebbé, C.; Peschel, C.; Quirt, I.; Clark, J. I.; Wolchok, J. D.; Weber, J. S.; Tian, J.; Yellin, M. J.; Nichol, G. M.; Hoos, A.; Urba, W. J. (2010-08-19). "Improved Survival with Ipilimumab in Patients with Metastatic Melanoma". The New England Journal of Medicine. 363 (8): 711–723. doi:10.1056/NEJMoa1003466. PMC 3549297. PMID 20525992.
- ↑ pmhdev. "Immunotherapy drug combo could combat melanoma". PubMed Health.
- ↑ "Peregrine Pharmaceuticals Announces Initiation of an Investigator-Sponsored Trial Combining Its Immunotherapy Bavituximab and Ipilimumab (Yervoy) in Advanced Melanoma". Peregrine Pharmaceuticals, Inc. Archived from the original on 2015-10-14. Retrieved 2014-05-20.
- ↑ "A Two-arm, Single Center Phase 1b Trial of Bavituximab Plus Ipilimumab in Advanced Melanoma Patients". ClinicalTrials.gov. Archived from the original on 2016-01-19. Retrieved 2021-08-01.
- ↑ "Data Presented at AACR Support Potential of Peregrine's PS-Targeting Immunotherapy Bavituximab to Enhance Anti-Tumor and Immune-Stimulating Effects of Anti-CTLA-4 and Anti-PD-1 Treatments in Models of Melanoma and Colon Cancer". Reuters. 2014-04-09. Archived from the original on 2014-05-21. Retrieved 2014-04-09.
- ↑ "'Surprise' prostate result probed". BBC News. 2009-06-19. Archived from the original on 2009-06-24. Retrieved 2009-06-24.
- ↑ "Mayo Researchers: Dramatic Outcomes in Prostate Cancer Study". Mayo Clinic. 2009-06-01. Archived from the original on 2009-06-23. Retrieved 2009-06-24.
- ↑ Boyles S (2009-06-19). "New Therapy May Fight Prostate Cancer". WebMD. Archived from the original on 2009-06-23. Retrieved 2009-06-24.
- ↑ Lowe, Derek (2009-06-23). "Medarex, Ipilimumab, Prostate Cancer, And Reality". Science Translational Medicine. Archived from the original on 2016-08-19. Retrieved 2016-08-11.
- ↑ "Biomarker-Driven Therapy With Nivolumab and Ipilimumab in Treating Patients With Metastatic Hormone-Resistant Prostate Cancer Expressing AR-V7 - Full Text View - ClinicalTrials.gov". clinicaltrials.gov. Archived from the original on 2016-03-05. Retrieved 2016-02-27.
- 1 2 Silberstein, John L.; Taylor, Maritza N.; Antonarakis, Emmanuel S. (2016-02-23). "Novel Insights into Molecular Indicators of Response and Resistance to Modern Androgen-Axis Therapies in Prostate Cancer". Current Urology Reports. 17 (4): 29. doi:10.1007/s11934-016-0584-4. ISSN 1527-2737. PMC 4888068. PMID 26902623.
- ↑ Antonarakis, Emmanuel S.; Lu, Changxue; Wang, Hao; Luber, Brandon; Nakazawa, Mary; Roeser, Jeffrey C.; Chen, Yan; Mohammad, Tabrez A.; Chen, Yidong (2014-09-11). "AR-V7 and Resistance to Enzalutamide and Abiraterone in Prostate Cancer". New England Journal of Medicine. 371 (11): 1028–1038. doi:10.1056/NEJMoa1315815. ISSN 0028-4793. PMC 4201502. PMID 25184630.
- 1 2 3 4 5 6 7 Hellmann, Matthew D.; Paz-Ares, Luis; Caro, Reyes Bernabe; Zurawski, Bogdan; Kim, Sang-We; Costa, Enric Carcereny; Park, Keunchil; Alexandru, Aurelia; Lupinacci, Lorena; Jimenez, Emmanuel de la Mora; Sakai, Hiroshi (2019-09-28). "Nivolumab plus Ipilimumab in Advanced Non–Small-Cell Lung Cancer". New England Journal of Medicine. 381 (21): 2020–2031. doi:10.1056/NEJMoa1910231. PMID 31562796. Archived from the original on 2021-07-31. Retrieved 2021-08-01.
- 1 2 3 4 5 6 7 8 Nasser, Nicola J.; Gorenberg, Miguel; Agbarya, Abed (November 2020). "First line Immunotherapy for Non-Small Cell Lung Cancer". Pharmaceuticals. 13 (11): 373. doi:10.3390/ph13110373. PMC 7695295. PMID 33171686.
- 1 2 3 Reck, Martin; Ciuleanu, Tudor-Eliade; Dols, Manuel Cobo; Schenker, Michael; Zurawski, Bogdan; Menezes, Juliana; Richardet, Eduardo; Bennouna, Jaafar; Felip, Enriqueta; Juan-Vidal, Oscar; Alexandru, Aurella (2020-05-20). "Nivolumab (NIVO) + ipilimumab (IPI) + 2 cycles of platinum-doublet chemotherapy (chemo) vs 4 cycles chemo as first-line (1L) treatment (tx) for stage IV/recurrent non-small cell lung cancer (NSCLC): CheckMate 9LA". Journal of Clinical Oncology. 38 (15_suppl): 9501. doi:10.1200/JCO.2020.38.15_suppl.9501. ISSN 0732-183X. Archived from the original on 2021-10-31. Retrieved 2021-08-01.
- ↑ "Impact of gemcitabine + cisplatin + ipilimumab on circulating immune cells in patients (pts) with metastatic urothelial cancer (mUC). - 2015 ASCO Annual Meeting - Abstracts - Meeting Library". Archived from the original on 2016-03-08. Retrieved 2021-08-01.
- ↑ Galsky, Matthew D.; Wang, Huan; Hahn, Noah M.; Twardowski, Przemyslaw; Pal, Sumanta K.; Albany, Costatine; Fleming, Mark T.; Starodub, Alexander; Hauke, Ralph J.; Yu, Menggang; Zhao, Qianqian; Sonpavde, Guru; Donovan, Michael J; Patel, Vaibhav G.; Sfakianos, John P.; Domingo-Domenech, Josep; Oh, William K.; Akers, Nicholas; Losic, Bojan; Gnjatic, Sacha; Schadt, Eric E.; Chen, Rong; Kim-Schulze, Seunghee; Bhardwaj, Nina; Uzilov, Andrew V. (2018). "Phase 2 Trial of Gemcitabine, Cisplatin, plus Ipilimumab in Patients with Metastatic Urothelial Cancer and Impact of DNA Damage Response Gene Mutations on Outcomes". European Urology. 73 (5): 751–759. doi:10.1016/j.eururo.2017.12.001. ISSN 0302-2838. PMID 29248319. Archived from the original on 2021-10-31. Retrieved 2021-08-01.
External links
| External sites: |
|
|---|---|
| Identifiers: |
- "Ipilimumab". NCI Drug Dictionary. National Cancer Institute. Archived from the original on 2020-10-21. Retrieved 2021-08-01.
- "Ipilimumab". National Cancer Institute. Archived from the original on 2021-07-09. Retrieved 2021-08-01.