Peripheral ossifying fibroma
| Peripheral ossifying fibroma | |
|---|---|
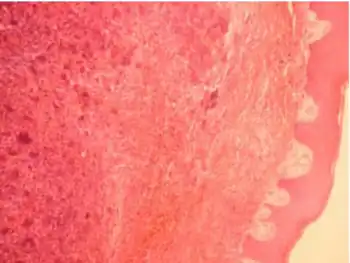 | |
| Peripheral ossifying fibroma with fibrous connective tissue | |
| Specialty | Dentistry |
Peripheral ossifying fibroma, also known as ossifying fibrous epulis, is “a gingival nodule which is composed of a cellular fibroblastic connective tissue stroma which is associated with the formation of randomly dispersed foci of mineralised products, which consists of bone, cementum-like tissue, or a dystrophic calcification. The lesion is considered part of an ossifying fibroma, but that is usually considered to be a jaw tumor. Because of its overwhelming incidence on the gingiva, the condition is associated with two other diseases, though not because they occur together. Instead, the three are associated with each other because they appear frequently on gingiva: pyogenic granuloma and peripheral giant cell granuloma. Some researchers believe peripheral ossifying fibromas to be related to pyogenic fibromas and, in some instances, are the result of a pyogenic granuloma which has undergone fibrosis and calcification.
The term peripheral ossifying fibroma has been criticized as this lesion is not related to the ossifying fibroma of bone and is not a fibroma.[1] This term is used in America, however in Britain, this lesion would be termed a fibrous epulis containing bone.[1]
Signs and symptoms
The color of peripheral ossifying fibromas ranges from red to pink, and is frequently ulcerated.[2] It can be sessile or pedunculated with the size usually being less than 2 cm. Weeks or months may pass by before it is seen and diagnosed.
There is a gender difference with 66% of the disease occurring in females. The prevalence of peripheral ossifying fibromas is highest around 10 – 19 years of age. It appears only on the gingiva, more often on the maxilla rather than the mandible, and is frequently found in the area around incisors and canines. The adjacent teeth are usually not affected.
Peripheral ossifying fibromas appear microscopically as a combination of a mineralized product and fibrous proliferation. The mineralized portion may be bone, cementum-like, or dystrophic calcifications. Additionally, highly developed bone or cementum is more likely to be present when the peripheral ossifying fibroma has existed for a longer period of time.
Diagnosis
In terms of the diagnosis for Peripheral ossifying fibroma, it is done via biopsy and pathological exam[3]
Treatment
Treatment usually involves surgical removal of the lesion down to the bone.[2] If there are any adjacent teeth, they are cleaned thoroughly to remove any possible source of irritation. Surgical methods can be traditional, Nd:YAG laser or QMR scalpel. Recurrence is around 16%,[4] with some studies reporting up to 45%.[5] It is unclear if the rate of recurrence is influenced by the surgical technique used.[5]
References
- 1 2 Cawson RA, Odell EW (2002). Cawson's essentials of oral pathology and oral medicine (7. ed.). Edinburgh: Churchill Livingstone. pp. 275–278. ISBN 0443071063.
- 1 2 Poonacha KS, Shigli AL, Shirol D (2010). "Peripheral ossifying fibroma: A clinical report". Contemp Clin Dent. 1 (1): 54–6. doi:10.4103/0976-237X.62520. PMC 3220071. PMID 22215935.
- ↑ "Peripheral ossifying fibroma | DermNet NZ". dermnetnz.org. Archived from the original on 13 August 2021. Retrieved 28 April 2022.
- ↑ Thompson LD, Wenig BM. Diagnostic Pathology: Head and Neck. Lippincott Williams & Wilkins, 2011; 4:66-67 (ISBN 1931884617)
- 1 2 Kaplan, G A; Seeman, T E; Cohen, R D; Knudsen, L P; Guralnik, J (1987). "Mortality among the elderly in the Alameda County Study: behavioral and demographic risk factors". American Journal of Public Health. 77 (3): 307–312. doi:10.2105/AJPH.77.3.307. ISSN 0090-0036. PMC 1646902. PMID 3812836.
External links
| Classification |
|---|