Potassium-sparing diuretic
Potassium-sparing diuretics refers to drugs that cause diuresis without causing potassium loss in the urine.[1] They are typically used as an adjunct in management of hypertension, cirrhosis, and congestive heart failure.[2] The steroidal aldosterone antagonists can also be used for treatment of primary hyperaldosteronism. Spironolactone, a steroidal aldosterone antagonist, is also used in management of female hirsutism and acne from PCOS or other causes.[3][4]
Types of Potassium-Sparing Diuretics
- Epithelial sodium channel blockers:[5]
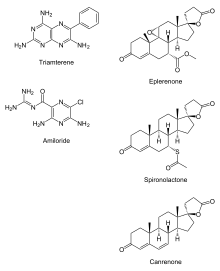
- Amiloride - better tolerated than triamterene
- Triamterene - increased renal side-effects
- Aldosterone antagonists, also known as mineralocorticoid receptor antagonists:[6]
- Spironolactone - most widespread use, inexpensive
- Eplerenone - more selective so reduced side-effects but more expensive and less potent
- Finerenone - non-steroidal, more selective and potent than spironolactone and eplerenone
- Canrenone - very limited use
Mechanism of action
Normally, sodium is reabsorbed in the collecting tubules of a renal nephron. This occurs via epithelial sodium channels or ENaCs, located on the luminal surface of principal cells that line the collecting tubules. Positively-charged Na+ entering the cells during reabsorption leads to an electronegative luminal environment causing the secretion of potassium (K+) into the lumen/ urine in exchange.[1] Sodium reabsorption also causes water retention.
When the kidneys detect low blood pressure, the renin–angiotensin–aldosterone system (RAAS) is activated and eventually, aldosterone is secreted. Aldosterone binds to aldosterone receptors (mineralocorticoid receptors) increasing sodium reabsorption in an effort to increase blood pressure and improve fluid status in the body. When excessive sodium reabsorption occurs, there is an increasing loss of K+ in the urine and can lead to clinically significant decreases, termed hypokalemia. Increased sodium reabsorption also increases water retention.
Potassium-sparing diuretics act to prevent sodium reabsorption in the collecting tubule by either binding ENaCs (amiloride, triamterene) or by inhibiting aldosterone receptors (spironolactone, eplerenone). This prevents excessive excretion of K+ in urine and decreased retention of water, preventing hypokalemia.[7]
Because these diuretics are weakly natriuretic, they do not cause clinically significant blood pressure changes and thus, are not used as primary therapy for hypertension.[8] They can be used in combination with other anti-hypertensives or drugs that cause hypokalemia to help maintain a normal range for potassium. For example, they are often used as an adjunct to loop diuretics (usually furosemide) to treat fluid retention in congestive heart failure and ascites in cirrhosis.[8]
Adverse effects
On their own this group of drugs may raise potassium levels beyond the normal range, termed hyperkalemia, which risks potentially fatal arrhythmias. Triamterene, specifically, is a potential nephrotoxin and up to half of the patients on it can have crystalluria or urinary casts.[9][10] Spironolactone can cause gynecomastia, menstrual abnormalities, impotence, and decreased libido by binding non-selective estrogen and progesterone receptors.
Other diuretics
While not classically considered potassium-sparing diuretics, ACE inhibitors (ACEis) and angiotensin receptor blockers (ARBs) are anti-hypertensive drugs with diuretic effects that decrease renal excretion of potassium. They work by inhibiting either the production (ACEis) or effects (ARBs) of angiotensin 2. This results in a decrease in aldosterone release, which causes potassium-sparing-diuretic-like effects similar to those of the aldosterone antagonists, spironolactone, and eplerenone.
See also
References
- 1 2 Rose BD (February 1991). "Diuretics". Kidney Int. 39 (2): 336–52. doi:10.1038/ki.1991.43. PMID 2002648.
- ↑ Weber KT, Villarreal D (January 1993). "Aldosterone and antialdosterone therapy in congestive heart failure". The American Journal of Cardiology. 71 (3): A3–A11. doi:10.1016/0002-9149(93)90238-8. PMID 8422002.
- ↑ Martin KA, Anderson RB, et al. (1 April 2018). "Evaluation and Treatment of Hirsutism in Premenopausal Women: An Endocrine Society* Clinical Practice Guideline". The Journal of Clinical Endocrinology & Metabolism. 103 (4): 1233–1257. doi:10.1210/jc.2018-00241. PMID 29522147.
- ↑ Grandhi R, Alikhan A (2017). "Spironolactone for the Treatment of Acne: A 4-Year Retrospective Study". Dermatology. 233 (2–3): 141–144. doi:10.1159/000471799. PMID 28472793.
- ↑ Sica DA, Gehr TW (1989). "Triamterene and the Kidney". Nephron. 51 (4): 454–461. doi:10.1159/000185375. PMID 2662034.
- ↑ Lainscak M, Pelliccia F, et al. (December 2015). "Safety profile of mineralocorticoid receptor antagonists: Spironolactone and eplerenone". International Journal of Cardiology. 200: 25–29. doi:10.1016/j.ijcard.2015.05.127. PMID 26404748.
- ↑ Horisberger J, Giebisch G (1987). "Potassium-Sparing Diuretics". Kidney and Blood Pressure Research. 10 (3–4): 198–220. doi:10.1159/000173130. PMID 2455308.
- 1 2 Hropot M, Fowler N, Karlmark B, Giebisch G (September 1985). "Tubular action of diuretics: Distal effects on electrolyte transport and acidification". Kidney International. 28 (3): 477–489. doi:10.1038/ki.1985.154. PMID 4068482.
- ↑ Modell JH, Graves SA, Ketover A (August 1976). "Clinical course of 91 consecutive near-drowning victims". Chest. 70 (2): 231–8. doi:10.1378/chest.70.2.231. PMID 780069.
- ↑ Fairley KF, Woo KT, Birch DF, Leaker BR, Ratnaike S (October 1986). "Triamterene-induced crystalluria and cylinduria: clinical and experimental studies". Clinical Nephrology. 26 (4): 169–73. PMID 3780069.
External links
- Potassium+Sparing+Diuretics at the US National Library of Medicine Medical Subject Headings (MeSH)