Chronic relapsing inflammatory optic neuropathy
| Chronic relapsing inflammatory optic neuropathy | |
|---|---|
| Other names: Chronic relapsing inflammatory optic neuritis | |
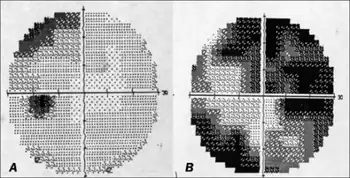 | |
| a,b)Automated perimetry at index event showing field defects in both eyes | |
| Specialty | Ophthalmology |
Chronic relapsing inflammatory optic neuropathy (CRION) is a form of recurrent optic neuritis that is steroid responsive.[1] Patients typically present with pain associated with visual loss.[1] CRION is a diagnosis of exclusion, and other demyelinating, autoimmune, and systemic causes should be ruled out.[2] Early recognition is crucial given risks for severe visual loss and because it is treatable with immunosuppressive treatment such as steroids.[2] Relapse that occurs after reducing or stopping steroids is a characteristic feature. [2]
Signs and symptoms
Pain, visual loss, relapse, and steroid response are typical of CRION.[1][2] Ocular pain is typical, although there are some cases with no reported pain.[2] Bilateral severe visual loss (simultaneous or sequential) usually occurs, but there are reports of unilateral visual loss.[2] Patients can have an associated relative afferent pupillary defect.[3] CRION is associated with at least one relapse, and up to 18 relapses have been reported in an individual.[4] Interval between episodes can range from days to over a decade.[1] Symptoms will improve with corticosteroids, and recurrence characteristically occurs after reducing or stopping steroids.[2]
Pathogenesis
As of 2013, the etiology remained unknown.[1] Given that CRION is responsive to immunosuppressive treatment, it may be immune-mediated.[2] CRION has been classified as an autoimmune process but this description is not established with certainty and there is no known associated autoimmune antibody. [2][5]
Since 2015, some research points to CRION belonging to the antiMOG associated encephalomyelitis spectrum.[6]
As of 2019, the correlation between CRION and antiMOG associated encephalomyelitis is so high that now CRION is considered the most common phenotype related to myelin oligodendrocyte glycoprotein antibodies[7]
As of 2021, some reports point out a second kind of CRION due to anti-phospholipid antibodies (anti-PL)[8]
Diagnosis
Diagnosis requires exclusion of other neurological, ophthalmological, and systemic conditions.[2] Any cause of optic neuropathy should be ruled out, including demyelinating (multiple sclerosis, and neuromyelitis optica) and systemic disease (diabetic, toxic, nutritional, and infectious causes).[2] Corticosteroid responsive optic neuritis not associated with demyelinating disease should also be ruled out, including sarcoidosis, systemic lupus erythematosus, or other systemic autoimmune disease.[9] Hereditary causes such as Leber’s hereditary optic neuropathy are also part of the differential diagnosis.[10]
There are no current diagnostic biomarkers or imaging features typical of CRION.[2] ANA, B12, folate, thyroid function tests, anti-aquaporin 4 antibodies (NMO-IgG), and GFAP can facilitate ruling out of other diseases.[2] Most patients are seronegative for NMO-IgG and GFAP, biomarkers for neuromyelitis optica.[2] ANA, indicative of autoimmune optic neuropathy, is also generally negative.[2] CSF can also be evaluated for oligoclonal bands typical of multiple sclerosis, which will not be present in CRION.[1] Chest X-ray or CT should be ordered if granulomatous optic neuropathy caused by sarcoidosis is suspected.[2]
MRI imaging can capture optic nerve inflammation, but this finding is not present in all patients,[1][2][11] Diffusion tensor imaging has been shown to detect widespread white matter abnormalities in CRION patients with normal MRI findings [12]
Five diagnostic criteria have been proposed:[2]
- History of optic neuritis with one relapse
- Objectively measured visual loss
- NMO-IgG seronegative
- Contrast enhancement on imaging of acutely inflamed optic nerves
- Response to immunosuppressive treatment and relapse on withdrawal or dose reduction
Treatment
Treatment consists of three phases:
- 1. Acute phase: IV steroids (methylprednisolone 1 mg/kg) for 3–5 days or plasmapheresis are given to restore visual function.[2]
- 2. Intermediate phase: Oral steroids (typically prednisone 1 mg/kg) with taper are given to stabilize vision.[2]
- 3. Long-term phase: To avoid adverse effects of long-term steroids and to avoid relapse of disease, physicians can transition to a steroid-sparing agent. Azathioprine, methotrexate, cyclophosphamide, mycophenolate, IVIG, plasma exchange, cyclosporine, and infliximab have been used.[2]
Visual acuity is dramatically worse with CRION than other forms of optic neuritis.[2] Treatment with corticosteroids induces prompt relief of pain and improved vision.[1] At times, patients obtain complete restoration of vision, although exact success rates are unknown.[1]
Prognosis
Recurrence is essentially inevitable in patients without treatment and patients ultimately will require lifelong immunosuppression to prevent relapse.[2][13]
Epidemiology
CRION was first described in 2003.[1] The disease is rare, with only 122 cases published from 2003 to 2013.[2] There is female predominance with 59 females (48%), 25 males (20%), and no gender designation for the rest of the 122 reported cases (32%).[2] Age ranges from 14 to 69 years of age, and the mean age is 35.6.[2] The disease is noted to occur worldwide and across many ethnicities, with reported cases in all continents except Africa and Australia.[2]
See also
References
- 1 2 3 4 5 6 7 8 9 10 Kidd D, Burton B, Plant GT, Graham EM. Chronic relapsing inflammatory optic neuropathy (CRION). Brain : A Journal of Neurology. Feb 2003;126(Pt 2):276-284
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 Petzold A, Plant GT. Chronic relapsing inflammatory optic neuropathy: a systematic review of 122 cases reported. Journal of Neurology. Jan 2014;261(1):17-26.
- ↑ Kaut O, Klockgether T. 51-year-old female with steroid-responsive optic neuropathy: a new case of chronic relapsing inflammatory optic neuropathy (CRION). Journal of Neurology. Sep 2008;255(9):1419-1420
- ↑ Saini M, Khurana D. Chronic relapsing inflammatory optic neuropathy. Annals of Indian Academy of Neurology. Jan 2010;13(1):61-63
- ↑ Petzold A, Plant GT. Diagnosis and classification of autoimmune optic neuropathy. Autoimmunity Reviews. Apr-May 2014;13(4-5):539-545
- ↑ Konstantina Chalmoukou el al. Anti-MOG antibodies are frequently associated with steroid-sensitive recurrent optic neuritis, Neurol Neuroimmunol Neuroinflamm. 2015 Aug; 2(4): e131. 2015 Jul 2. doi:10.1212/NXI.0000000000000131, PMC 4496630
- ↑ Laura Navarro Canto et al., BRAIN ATROPHY IN RELAPSING OPTIC NEURITIS IS ASSOCIATED WITH CRION PHENOTYPE, Front. Neurol., doi: 10.3389/fneur.2019.01157
- ↑ Navarro, Cristian Eduardo; Arango, Gabriel José; Cubides, María F. (20 April 2021). "Chronic relapsing inflammatory optic neuropathy in a patient with triple antiphospholipid antibody positivity". Neurological Sciences. doi:10.1007/s10072-021-05263-6.
- ↑ Myers TD, Smith JR, Wertheim MS, Egan RA, Shults WT, Rosenbaum JT. Use of corticosteroid sparing systemic immunosuppression for treatment of corticosteroid dependent optic neuritis not associated with demyelinating disease. The British Journal of Ophthalmology. May 2004;88(5):673-680
- ↑ Lee MD, Song BJ, Odel JG, Sadun AA. Bilateral vision loss responsive to corticosteroids. Survey of Ophthalmology. Nov-Dec 2013;58(6):634-639
- ↑ Sharma A, Khurana D, Kesav P. MRI findings in chronic relapsing inflammatory optic neuropathy. BMJ Case Reports. 2013;2013
- ↑ Colpak AI, Kurne AT, Oguz KK, Has AC, Dolgun A, Kansu T. White matter involvement beyond the optic nerves in CRION as assessed by diffusion tensor imaging. The International journal of neuroscience. Jan 2015;125(1):10-17
- ↑ Malik A, Ahmed M, Golnik K. Treatment options for atypical optic neuritis. Indian Journal of Ophthalmology. Oct 2014;62(10):982-984