Retinal detachment
| Retinal detachment | |
|---|---|
| Other names: Detached retina | |
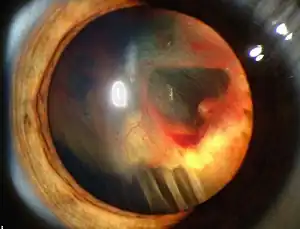 | |
| Slit lamp photograph showing retinal detachment. | |
| Specialty | Ophthalmology |
| Symptoms | Increased number of floaters, flashes of light, worsening of the outer part of the visual field[1][2] |
| Complications | Permanent loss of vision[3] |
| Usual onset | 60s and 70s[1] |
| Causes | Retina separates from the layer underneath[1] |
| Risk factors | Posterior vitreous detachment, injury to the eye, inflammation of the eye, short sighted, previous cataract surgery[1] |
| Diagnostic method | Eye exam, ultrasound[1][3] |
| Treatment | Scleral buckling, pneumatic retinopexy, vitrectomy[1] |
| Prognosis | Generally good if treated early[3][4] |
| Frequency | ~1 per 10,000 per year[5] |
Retinal detachment is a disorder of the eye in which the retina separates from the layer underneath.[1] Symptoms include an increase in the number of floaters, flashes of light, and worsening of the outer part of the visual field.[1][2] This may be described as a curtain over part of the field of vision.[2] In about 7% of cases both eyes are affected.[5] Without treatment permanent loss of vision may occur.[3]
The mechanism most commonly involves a break in the retina that then allows the fluid in the eye to get behind the retina.[1] A break in the retina can occur from a posterior vitreous detachment, injury to the eye, or inflammation of the eye.[1] Other risk factors include being short sighted and previous cataract surgery.[1] Retinal detachments also rarely occur due to a choroidal tumor.[1] Diagnosis is by either looking at the back of the eye with an ophthalmoscope or by ultrasound.[1][3]
In those with a retinal tear, efforts to prevent it becoming a detachment include cryotherapy using a cold probe or photocoagulation using a laser.[1] Treatment of retinal detachment should be carried out in a timely manner.[1] This may include scleral buckling where silicone is sutured to the outside of the eye, pneumatic retinopexy where gas is injected into the eye, or vitrectomy where the vitreous is partly removed and replaced with either gas or oil.[1]
Retinal detachments affect between 0.6 and 1.8 people per 10,000 per year.[5] About 0.3% of people are affected at some point in their life.[4] It is most common in people who are in their 60s or 70s.[1] Males are more often affected than females.[1] The long term outcomes depend on the duration of the detachment and whether the macula was detached.[1] If treated before the macula detaches outcomes are generally good.[3][4]
Signs and symptoms
A rhegmatogenous retinal detachment is commonly preceded by a posterior vitreous detachment which gives rise to these symptoms:
- very brief flashes of light (photopsia) in the extreme peripheral (outside of center) part of vision
- a sudden dramatic increase in the number of floaters
- a ring of floaters or hairs just to the temporal (skull) side of the central vision
Although most posterior vitreous detachments do not progress to retinal detachments, those that do produce the following symptoms:
- a dense shadow that starts in the peripheral vision and slowly progresses towards the central vision
- the impression that a veil or curtain was drawn over the field of vision
- straight lines (scale, edge of the wall, road, etc.) that suddenly appear curved (positive Amsler grid test)
- central visual loss
In the event of an appearance of sudden flashes of light or floaters, an eye doctor needs to be consulted immediately.[6] Any loss of vision is also a medical emergency.
Risk factors
Risk factors for retinal detachment include severe myopia, retinal tears, trauma, family history, as well as complications from cataract surgery.[4][7]
Retinal detachment can be mitigated in some cases when the warning signs [8] are caught early. The most effective means of prevention and risk reduction is through education of the initial signs, and encouragement for people to seek ophthalmic medical attention if they have symptoms suggestive of a posterior vitreous detachment.[9] Early examination allows detection of retinal tears which can be treated with laser or cryotherapy. This reduces the risk of retinal detachment in those who have tears from around 1:3 to 1:20. For this reason, the governing bodies in some sports require regular eye examination.
Trauma-related cases of retinal detachment can occur in high-impact sports or in high speed sports. Although some recommend avoiding activities that increase pressure in the eye, including diving and skydiving, there is little evidence to support this recommendation, especially in the general population. Nevertheless, ophthalmologists generally advise people with high degrees of myopia to try to avoid exposure to activities that have the potential for trauma, increase pressure on or within the eye itself, or include rapid acceleration and deceleration, such as bungee jumping or roller coaster rides.
Intraocular pressure spikes occur during any activity accompanied by the Valsalva maneuver, including weightlifting.[10] An epidemiological study suggests that heavy manual lifting at work may be associated with increased risk of rhegmatogenous retinal detachment, but this relationship is not strong.[11][12] In this study, obesity also appeared to increase the risk of retinal detachment. A high Body Mass Index (BMI) and elevated blood pressure have been identified as a risk factor in non-myopic individuals.[13]
Genetic factors promoting local inflammation and photoreceptor degeneration may also be involved in the development of the disease.[14]
Other risk factors include the following:
- Glaucoma
- AIDS[15]
- Cataract surgery[16]
- Diabetic retinopathy[15][17]
- Eclampsia[18]
- Family history of retinal detachment[19]
- Homocysteinuria[20]
- Malignant hypertension[15][18]
- Metastatic cancer, which spreads to the eye (eye cancer)[21]
- Retinoblastoma[22]
- Severe myopia[7]
- Smoking and passive smoking[23][24]
- Stickler syndrome[15]
- Von Hippel-Lindau disease[25]
Diagnosis
Retinal detachment can be examined by fundus photography or ophthalmoscopy. Fundus photography generally needs a considerably larger instrument than the ophthalmoscope, but has the advantage of availing the image to be examined by a specialist at another location and/or time, as well as providing photo documentation for future reference. Modern fundus photographs generally recreate considerably larger areas of the fundus than what can be seen at any one time with handheld ophthalmoscopes.
Ultrasound has diagnostic accuracy similar to that of examination by an ophthalmologist.[27] The recent meta-analysis shows the diagnostic accuracy of emergency department (ED) ocular ultrasonography is high. The sensitivity and specificity ranged from 97% to 100% and 83% to 100%.[27] The typical feature of retinal detachment when viewed on ultrasound is "flying angel sign". It shows the detached retina moving with a fixed point under the B mode, linear probe 10 MHz.[27]
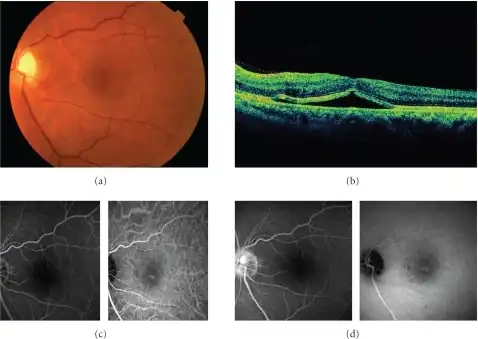 a) Image shows serous retinal detachment b) OCT shows retinal detachment involving the fovea c) early phase images of FA and IA d) Late phase images of FA and IA
a) Image shows serous retinal detachment b) OCT shows retinal detachment involving the fovea c) early phase images of FA and IA d) Late phase images of FA and IA A physician using a "three-mirror glass" to diagnose retinal detachment
A physician using a "three-mirror glass" to diagnose retinal detachment
Types
- Rhegmatogenous retinal detachment – A rhegmatogenous retinal detachment occurs due to a break in the retina (called a retinal tear) that allows fluid to pass from the vitreous space into the subretinal space between the sensory retina and the retinal pigment epithelium. Retinal breaks are divided into three types – holes, tears and dialyses. Holes form due to retinal atrophy especially within an area of lattice degeneration. Tears are due to vitreoretinal traction. Dialyses are very peripheral and circumferential, and may be either tractional or atrophic. The atrophic form most often occurs as idiopathic dialysis of the young.
- Exudative, serous, or secondary retinal detachment – An exudative retinal detachment occurs due to inflammation, injury or vascular abnormalities that results in fluid accumulating underneath the retina without the presence of a hole, tear, or break. In evaluation of retinal detachment it is critical to exclude exudative detachment as surgery will make the situation worse, not better. Although rare, exudative detachment can be caused by the growth of a tumor on the layers of tissue beneath the retina, namely the choroid. This cancer is called a choroidal melanoma.
- Tractional retinal detachment – A tractional retinal detachment occurs when fibrous or fibrovascular tissue, caused by an injury, inflammation or neovascularization, pulls the sensory retina from the retinal pigment epithelium.
A minority of retinal detachments result from trauma, including blunt blows to the orbit, penetrating trauma, and concussions to the head. A retrospective Indian study of more than 500 cases of rhegmatogenous detachments found that 11% were due to trauma, and that gradual onset was the norm, with over 50% presenting more than one month after the inciting injury.[28]
Treatment
There are several methods of treating a detached retina, each of which depends on finding and closing the breaks that have formed in the retina. All three of the procedures follow the same three general principles:
- Find all retinal breaks
- Seal all retinal breaks
- Relieve present (and future) vitreoretinal traction
Cryopexy and laser photocoagulation
Cryotherapy (freezing) or laser photocoagulation are occasionally used alone to wall off a small area of retinal detachment so that the detachment does not spread.
Scleral buckle surgery
Scleral buckle surgery is an established treatment in which the eye surgeon sews one or more silicone bands (or tyres) to the sclera (the white outer coat of the eyeball). The bands push the wall of the eye inward against the retinal hole, closing the break or reducing fluid flow through it and reducing the effect of vitreous traction thereby allowing the retina to re-attach. Cryotherapy (freezing) is applied around retinal breaks prior to placing the buckle. Often subretinal fluid is drained as part of the buckling procedure. The buckle remains in situ. The most common side effect of a scleral operation is myopic shift. That is, the operated eye will be more short sighted after the operation. Radial scleral buckle is indicated for U-shaped tears or Fishmouth tears, and posterior breaks. Circumferential scleral buckle is indicated for multiple breaks, anterior breaks and wide breaks. Encircling buckles are indicated for breaks covering more than 2 quadrants of retinal area, lattice degeneration located on more than 2 quadrant of retinal area, undetectable breaks, and proliferative vitreous retinopathy.
Pneumatic retinopexy
This operation is generally performed in the doctor's office under local anesthesia. It is another method of repairing a retinal detachment in which a gas bubble (SF6 or C3F8 gas) is injected into the eye after which laser or freezing treatment is applied to the retinal hole. The patient's head is then positioned so that the bubble rests against the retinal hole. Patients may have to keep their heads tilted for several days to keep the gas bubble in contact with the retinal hole. The surface tension of the gas/water interface seals the hole in the retina, and allows the retinal pigment epithelium to pump the subretinal space dry and "suck the retina back into place". This strict positioning requirement makes the treatment of the retinal holes and detachments that occurs in the lower part of the eyeball impractical. This procedure is usually combined with cryopexy or laser photocoagulation. Pneumatic retinopexy has significantly lower success rates compared to scleral buckle surgery and vitrectomy. Some initially successful cases will fail during the weeks and months after surgery. In some of the failed cases, an area of the retina which was healthy and attached prior to the initial pneumatic retinopexy repair procedure develops new tears and/or becomes detached. A recent Cochrane Review compared outcomes from patients receiving retinal reattachment from pneumatic retinopexy versus scleral buckle.[29] Though the quality of evidence from two randomized controlled trials was low, eyes having received the pneumatic retinopexy procedure were more likely to have a recurrence of retinal detachment by follow-up, and were 11% less likely to achieve retinal reattachment, compared to scleral buckle.[29]
Vitrectomy
Vitrectomy is an increasingly used treatment for retinal detachment. It involves the removal of the vitreous gel and is usually combined with filling the eye with either a gas bubble (SF6 or C3F8 gas) or silicone oil (PDMS). An advantage of using gas in this operation is that there is no myopic shift after the operation and gas is absorbed within a few weeks. PDMS, if used, needs to be removed after a period of 2–8 months depending on surgeon's preference. Silicone oil is more commonly used in cases associated with proliferative vitreo-retinopathy (PVR). A disadvantage is that a vitrectomy always leads to more rapid progression of a cataract in the operated eye. In many places vitrectomy is the most commonly performed operation for the treatment of retinal detachment. A recent Cochrane Review assessing various tamponade agents for patients with retinal detachment associated with PVR found that patients treated with C3F8 gas and standard silicone oil had visual and anatomic advantages over patients using SF6.[30] Heavy silicone oil did not show any advantages over regular silicone oil.[30] When a Cochrane review compared pars plana vitrectomy (PPV) with scleral buckle surgery, it was found that although there may be less recurrence of detachment, PPV may have little or no difference of success of operation and vision achieved.[31] Both PPV and scleral buckle were associated with adverse events though frequency of each type of event differed with each procedure.
Prognosis
85 percent of cases will be successfully treated with one operation with the remaining 15 percent requiring 2 or more operations. After treatment patients gradually regain their vision over a period of a few weeks, although the visual acuity may not be as good as it was prior to the detachment, particularly if the macula was involved in the area of the detachment.
Until the early 20th century, the prognosis for rhegmatogenous retinal detachment was very poor, and no effective treatments were available. Currently, about 95 percent of cases of retinal detachment can be repaired successfully.[32] Treatment failures usually involve either the failure to recognize all sites of detachment, the formation of new retinal breaks, or proliferative vitreoretinopathy.[32]
Involvement of the macula portends a worse prognosis. In cases where the macula is not involved (detached), 90 percent of patients have 20/40 vision or better after reattachment surgery.[32] Some damage to vision may occur during reattachment surgery, and 10 percent of patients with normal vision experience some vision loss after a successful reattachment surgery.
It is not clear if surgery is beneficial for asymptomatic retinal breaks or lattice degeneration.[33]
Epidemiology
The incidence of retinal detachment in otherwise normal eyes is around 5 new cases in 100,000 persons per year.[34] Detachment is more frequent in middle-aged or elderly populations, with rates of around 20 in 100,000 per year.[35] The lifetime risk in normal individuals is about 1 in 300.[4] Asymptomatic retinal breaks are present in about 6% of eyes in both clinical and autopsy studies.[33]
- Retinal detachment is more common in people with severe myopia (above 5–6 diopters), in whom the retina is more thinly stretched. In such patients, lifetime risk rises to 1 in 20.[36] About two-thirds of cases of retinal detachment occur in myopics. Myopic retinal detachment patients tend to be younger than non-myopic ones.
- Retinal detachment is more frequent after surgery for cataracts. The estimated long-term prevalence of retinal detachment after cataract surgery is in the range of 5 to 16 per 1000 cataract operations,[37] but is much higher in patients who are highly myopic, with a prevalence of up to 7% being reported in one study.[38] One study found that the probability of experiencing retinal detachment within 10 years of cataract surgery may be about 5 times higher than in the absence of treatment.[39]
- Tractional retinal detachments can also occur in patients with proliferative diabetic retinopathy[40] or those with proliferative sickle cell retinopathy disease.[41] In proliferative retinopathy, abnormal blood vessels (neovascularization) grow within the retina and extend into the vitreous. In advanced disease, the vessels can pull the retina away from the back wall of the eye, leading to tractional retinal detachment.
Although retinal detachment usually occurs in just one eye, there is a 15% chance of it developing in the other eye, and this risk increases to 25–30% in patients who have had a retinal detachment and cataracts extracted from both eyes.[36]
See also
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 Fraser, S; Steel, D (24 November 2010). "Retinal detachment". BMJ Clinical Evidence. 2010. PMC 3275330. PMID 21406128.
- 1 2 3 "Facts About Retinal Detachment". National Eye Institute. October 2009. Archived from the original on 28 July 2016. Retrieved 26 July 2016.
- 1 2 3 4 5 6 Gelston, CD (15 October 2013). "Common eye emergencies". American Family Physician. 88 (8): 515–19. PMID 24364572.
- 1 2 3 4 5 Gariano RF, Kim CH (2004). "Evaluation and management of suspected retinal detachment". American Family Physician. 69 (7): 1691–98. PMID 15086041.
- 1 2 3 Mitry, D; Charteris, DG; Fleck, BW; Campbell, H; Singh, J (June 2010). "The epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations". The British Journal of Ophthalmology. 94 (6): 678–84. doi:10.1136/bjo.2009.157727. PMID 19515646.
- ↑ "Retinal Detachment". Archived from the original on June 5, 2013. Retrieved July 26, 2013.
- 1 2 Haug SJ, Bhisitkul RB (2012). "Risk factors for retinal detachment following cataract surgery". Current Opinion in Ophthalmology. 23 (1): 7–11. doi:10.1097/ICU.0b013e32834cd653. PMID 22081033.
- ↑ "Detached retina (retinal detachment)". NHS UK. GOV.uk. 2018-01-11. Archived from the original on 2018-10-21. Retrieved October 21, 2018.
- ↑ Byer NE (1994). "Natural history of posterior vitreous detachment with early management as the premier line of defense against retinal detachment". Ophthalmology. 101 (9): 1503–13, discussion 1513–14. doi:10.1016/S0161-6420(94)31141-9. PMID 8090453.
- ↑ Dickerman RD, Smith GH, Langham-Roof L, McConathy WJ, East JW, Smith AB (1999). "Intra-ocular pressure changes during maximal isometric contraction: does this reflect intra-cranial pressure or retinal venous pressure?". Neurol. Res. 21 (3): 243–46. doi:10.1080/01616412.1999.11740925. PMID 10319330.
- ↑ Mattioli S, De Fazio R, Buiatti E, Truffelli D, Zanardi F, Curti S, Cooke RM, Baldasseroni A, Miglietta B, Bonfiglioli R, Tassinari G, Violante FS (2008). "Physical exertion (lifting) and retinal detachment among people with myopia". Epidemiology. 19 (6): 868–71. doi:10.1097/EDE.0b013e318187a7da. PMID 18854710.
- ↑ Mattioli S, Curti S, De Fazio R, Farioli A, Cooke RM, Zanardi F, Violante FS (2009). "Risk Factors for Retinal Detachment". Epidemiology. 20 (3): 465–66. doi:10.1097/EDE.0b013e31819f1b17. PMID 19363359.
- ↑ Farioli A, Hemmingsson T, Kriebel D (July 2016). "Vascular risk factors and rhegmatogenous retinal detachment: a follow-up of a national cohort of Swedish men". Br J Ophthalmol. 100 (7): 907–913. doi:10.1136/bjophthalmol-2015-307560. PMID 26472402.
- ↑ Delyfer MN, Raffelsberger W, Mercier D, Korobelnik JF, Gaudric A, Charteris DG, Tadayoni R, Metge F, Caputo G, Barale PO, Ripp R, Muller JD, Poch O, Sahel JA, Léveillard T (2011). Barnes S (ed.). "Transcriptomic Analysis of Human Retinal Detachment Reveals Both Inflammatory Response and Photoreceptor Death". PLoS ONE. 6 (12): e28791. Bibcode:2011PLoSO...628791D. doi:10.1371/journal.pone.0028791. PMC 3235162. PMID 22174898.
- 1 2 3 4 Yanoff & Duker 2008, p. 724
- ↑ Yanoff & Duker 2008, p. 492
- ↑ Goldman 2011, p. e236-13
- 1 2 Goldman 2011, p. 2467
- ↑ "Retinal detachment". MedlinePlus Medical Encyclopedia. National Institutes of Health. 2005. Archived from the original on 2006-06-24. Retrieved 2006-07-18.
- ↑ Goldman 2011, p. 1362
- ↑ Goldman 2011, p. 2442
- ↑ Goldman 2011, p. 2441
- ↑ Sema DÜNDAR; Fatih ÖZCURA; İbrahim METEOĞLU; Mehmet Erkut KARA (2012). "Effects of long-term passive smoking on the vascular endothelial growth factor and apoptosis marker expression in the retina and choroid" (PDF). Turk J Med Sci. 42 (3): 377–83. Archived (PDF) from the original on 2013-11-03.
- ↑ AJ Franklin; M Yu; RK Maturi (2002). "Tobacco Smoking Negatively Affects the Outcome of Retinal Detachment Repair". Invest Ophthalmol Vis Sci. 43. Archived from the original on 2013-04-30.
- ↑ Goldman 2011, pp. 2390–91
- ↑ "UOTW #12 - Ultrasound of the Week". Ultrasound of the Week. 5 August 2014. Archived from the original on 9 May 2017. Retrieved 27 May 2017.
- 1 2 3 Vrablik ME, Snead GR, Minnigan HJ, Kirschner JM, Emmett TW, Seupaul RA (February 2015). "The diagnostic accuracy of bedside ocular ultrasonography for the diagnosis of retinal detachment: a systematic review and meta-analysis". Ann Emerg Med. 65 (2): 199–203.e1. doi:10.1016/j.annemergmed.2014.02.020. PMID 24680547.
- ↑ Shukla Manoj; Ahuja OP; Jamal Nasir (1986). "Traumatic retinal detachment". Indian J Ophthalmol. 34 (1): 29–32. PMID 3443496.
- 1 2 Hatef E, Sena DF, Fallano KA, Crews J, Do DV (2015). "Pneumatic retinopexy versus scleral buckle for repairing simple rhegmatogenous retinal detachments". Cochrane Database Syst Rev. 5 (5): CD008350. doi:10.1002/14651858.CD008350.pub2. PMC 4451439. PMID 25950286.
- 1 2 Schwartz, Stephen G.; Flynn, Harry W.; Wang, Xue; Kuriyan, Ajay E.; Abariga, Samuel A.; Lee, Wen-Hsiang (15 May 2020). "Tamponade in surgery for retinal detachment associated with proliferative vitreoretinopathy". The Cochrane Database of Systematic Reviews. 5: CD006126. doi:10.1002/14651858.CD006126.pub4. ISSN 1469-493X. PMID 32408387. Archived from the original on 29 August 2021. Retrieved 8 July 2020.
- ↑ Znaor, Ljubo; Medic, Aleksej; Binder, Susanne; Vucinovic, Ana; Marin Lovric, Josipa; Puljak, Livia (2019-03-08). "Pars plana vitrectomy versus scleral buckling for repairing simple rhegmatogenous retinal detachments". Cochrane Database of Systematic Reviews. doi:10.1002/14651858.cd009562.pub2. ISSN 1465-1858. PMC 6407688. PMID 30848830. Archived from the original on 2021-08-29. Retrieved 2020-03-16.
- 1 2 3 Yanoff & Duker 2008, p. 725
- 1 2 Wilkinson, Charles P. (2014-09-05). "Interventions for asymptomatic retinal breaks and lattice degeneration for preventing retinal detachment". The Cochrane Database of Systematic Reviews (9): CD003170. doi:10.1002/14651858.CD003170.pub4. ISSN 1469-493X. PMC 4423540. PMID 25191970.
- ↑ Ivanisević M, Bojić L, Eterović D (2000). "Epidemiological study of nontraumatic phakic rhegmatogenous retinal detachment". Ophthalmic Res. 32 (5): 237–39. doi:10.1159/000055619. PMID 10971186.
- ↑ Li X (2003). "Incidence and epidemiological characteristics of rhegmatogenous retinal detachment in Beijing, China". Ophthalmology. 110 (12): 2413–17. doi:10.1016/S0161-6420(03)00867-4. PMID 14644727.
- 1 2 "eMedicine –Retinal Detachment : Article by Gregory Luke Larkin, MD, MSPH, MSEng, FACEP". Archived from the original on 2007-05-09. Retrieved 2007-06-04.
- ↑ Ramos M, Kruger EF, Lashkari K (2002). "Biostatistical analysis of pseudophakic and aphakic retinal detachments". Seminars in Ophthalmology. 17 (3–4): 206–13. doi:10.1076/soph.17.3.206.14784. PMID 12759852.
- ↑ Hyams SW, Bialik M, Neumann E (1975). "Myopia-aphakia. I. Prevalence of retinal detachment". The British Journal of Ophthalmology. 59 (9): 480–82. doi:10.1136/bjo.59.9.480. PMC 1042658. PMID 1203233.
- ↑ Rowe JA, Erie JC, Baratz KH, Hodge DO, Gray DT, Butterfield L, Robertson DM (1999). "Retinal detachment in Olmsted County, Minnesota, 1976 through 1995". Ophthalmology. 106 (1): 154–59. doi:10.1016/S0161-6420(99)90018-0. PMID 9917797.
- ↑ "Diabetic Retinopathy: Retinal Disorders: Merck Manual Home Health Handbook". Archived from the original on 2011-11-01. Retrieved 2007-06-04.
- ↑ "IU Opt Online CE: Retinal Vascular Disease: Sickle Cell Retinopathy". Archived from the original on 2003-01-11. Retrieved 2007-06-04.
- Works
- Goldman, Lee (2011). Goldman's Cecil Medicine (24th ed.). Philadelphia: Elsevier Saunders. ISBN 978-1437727883.
- Yanoff, Myron; Duker, Jay S. (2008). Ophthalmology (3rd ed.). Edinburgh: Mosby. ISBN 978-0323057516.
External links
| Classification | |
|---|---|
| External resources |
- Retinal Detachment Archived 2016-07-28 at the Wayback Machine Resource Guide from the National Eye Institute (NEI).
- Overview of retinal detachment from eMedicine Archived 2007-05-09 at the Wayback Machine
- Guidelines from the American Academy of Family Physicians Archived 2008-07-24 at the Wayback Machine
- Retinal detachment information from WebMD Archived 2008-07-24 at the Wayback Machine
- Retinal detachment information from the Merck Manual Archived 2011-11-02 at the Wayback Machine