Susac's syndrome
| Susac's syndrome | |
|---|---|
| Other names: Retinopathy-encephalopathy-deafness associated with microangiopathy | |
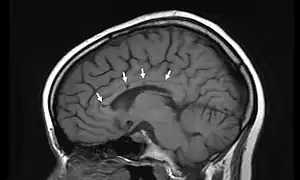 | |
| Sagittal T1 image in a 19-year-old woman with Susac's syndrome showing the pathognomonic central callosal "holes" (microinfarcts) of SS. These residual "holes" (and sometimes, "spokes") develop as the acute callosal changes resolve. | |
Susac's syndrome (retinocochleocerebral vasculopathy) is a very rare form of microangiopathy characterized by encephalopathy, branch retinal artery occlusions and hearing loss.[1] The cause is unknown but the current thinking is that antibodies are produced against endothelial cells in tiny arteries which leads to damage and the symptoms related to the illness. Despite this being an extremely rare disease, there are 4 registries collecting data on the illness; two are the United States, one in Germany, and one in Portugal.[2][3][4]
Signs and symptoms
Susac's syndrome is a very rare disease, of unknown cause, and many persons who experience it do not display the bizarre symptoms named here. Their speech can be affected, such as the case of a female of late teens who suffered speech issues and hearing problems, and many experience unrelenting and intense headaches and migraines, some form of hearing loss, and impaired vision. The problem usually corrects itself, but this can take up to five years. In some cases, subjects can become confused. The syndrome usually affects women around the age of 18 years, with female to male ratio of cases of 2:1.
Pathogenesis
In the March 1979 report in Neurology, Drs. Susac, Hardman and Selhorst reported two patients with the triad of encephalopathy, hearing loss and microangiopathy of the retina. The first patient underwent brain biopsy, which revealed sclerosis of the media and adventitia of small pial and cortical vessels, suggestive of a healed angiitis. Both patients underwent fluorescein retinal angiography that demonstrated multifocal retinal artery occlusions without evidence of embolic disease. Though the exact pathogenesis of this disorder is unknown, the retinal and brain biopsy findings suggest a small vessel vasculopathy leading to arteriolar occlusion and microinfarction of cerebral, retinal and cochlear tissue. Demyelination is not a typical feature of Susac's syndrome. Muscle biopsies from such patients are usually normal, but some have also shown nonspecific signs of inflammation such as dense hyaline material surrounding endomysial capillaries. This suggests a possible systemic component of this disease, despite the predominance of central nervous system features. The latest thinking is that an antibody directed against endothelial cells is the pathogenic mechanism in this disease which causes the microscopic strokes in the brain, retina, and inner ear.
Diagnosis
Patients typically present with low frequency hearing loss detectable via an audiogram. Headaches are frequently present in addition to roaring tinnitus and often some degree of paranoia. Partial vision loss is often present and caused by branch retinal artery occlusions. The presence of refractile or non-refractile yellow Gass plaques in the retinal arterioles is near pathognomonic for the disease. Fluorescein angiography may demonstrate leakage in areas remote from the retinal infarctions.
Radiographic appearance
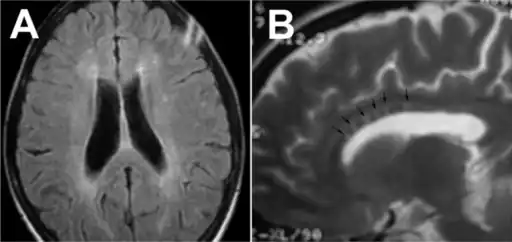
In a recent analysis (Susac et al., 2003), MRI images from 27 patients fulfilling the diagnostic criteria of Susac's syndrome were reviewed. Multifocal supratentorial lesions were present in all patients. Most lesions were small (3 to 7 mm), though some were larger than 7 mm. All 27 patients had corpus callosum lesions. These all had a punched-out appearance on follow up MRI. Though most commonly involving white matter, many patients also had lesions in deep grey matter structures, as well as leptomeningeal enhancement. Multiple sclerosis (MS) and acute disseminated encephalomyelitis (ADEM) can mimic the MRI changes seen in patients with Susac's syndrome. However, the callosal lesions in Susac's syndrome are centrally located. In comparison, patients with MS and ADEM typically have lesions involving the undersurface of the corpus callosum. Deep gray matter involvement commonly occurs in ADEM but is very rare in MS. Leptomeningeal involvement is not typical of either MS or ADEM. What this means is that if 10 lesions are found in the brain of an MS patient, a lesion may be found in the corpus callosum. If you have 10 lesions in a Susac patient, more than half will be in the corpus callosum.
A concern about this illness is that it mimics multiple sclerosis when looking at the vision loss and brain lesions. If close attention is not paid to the retina of a patient with vision loss and brain lesions, their symptoms may be mistaken for MS instead of Susac's syndrome. This may account for the low prevalence of the illness. There is also a pathological similarity between the endotheliopathy in Susac's syndrome with that seen in juvenile dermatomyositis.
Treatment
Early and aggressive treatment is important to prevent irreversible neurological damage, hearing loss, or vision loss. Medications used include immunosuppressive agents and corticosteroids such a prednisone, or intravenous immunoglobulins (IVIG). Other drugs that have been used are mycophenolate mofetil (Cellcept), azathioprine (Imuran), cyclophosphamide, rituximab, and anti-TNF therapies.[5]
Hearing aids or cochlear implants may be necessary in the event of hearing loss.[5]
History
Susac's syndrome is named for Dr. John Susac (1940–2012), of Winter Haven, Florida, who first described it in 1979.[6]William F. Hoyt was the first to call the syndrome "Susac syndrome" and later Robert Daroff asked Dr. Susac to write an editorial in Neurology about the disorder and to use the eponym of Susac syndrome in the title, forever linking this disease with him.
References
- ↑ Lian K, Siripurapu R, Yeung R, Hopyan J, Eng K, Aviv RI, Symons SP. Susac’s syndrome. Canadian Journal of Neurological Sciences. 2011 March, 38(2):335-337.
- ↑ "Susac Syndrome". Cleveland Clinic. Archived from the original on 2014-08-09. Retrieved 2016-03-01.
- ↑ "Calling All Cases of Susac Syndrome!". NOVEL: Patient Rare Disease Registry. Archived from the original on 2016-03-04. Retrieved 2016-03-01.
- ↑ "Für Ärzte und Patienten zu allen Fragen rund um das Susac-Syndrom". EUSAC, European Susac Consortium (in German). Archived from the original on 2018-03-14. Retrieved 2016-03-01.
{{cite web}}: CS1 maint: unrecognized language (link) - 1 2 "Susac's Syndrome". NORD (National Organization for Rare Disorders). Archived from the original on 2016-03-05. Retrieved 2016-03-01.
- ↑ Susac J, Hardman J, Selhorst J (1979). "Microangiopathy of the brain and retina". Neurology. 29 (3): 313–6. doi:10.1212/wnl.29.3.313. PMID 571975. S2CID 36927159.
- Egan RA, Nguyen TH, Gass JDM, Rizzo JF, Tivnan J, Susac JO. Retinal Artery Wall Plaques in Susac Syndrome. American Journal of Ophthalmology 135: 483-6; 2003
- Susac JO, Murtagh FR, Egan RA, Berger JR, Fox RJ, Galetta S, Costello F, Lee AG, Bakshi R, Lincoff N, Clark J, Daroff R. MRI Findings in Susac Syndrome. Neurology 61: 1783-1787; 2003
- Egan RA, Hills WL, Susac JO. Gass Plaques and Fluorescein Leakage in Susac Syndrome. Journal of Neurological Sciences 299(1-2): 97-100; 2010
- Susac JO, Rennebohm RM, Egan RA, Daroff RB. Susac’s Syndrome – Update. Journal of Neurological Sciences 299(1-2): 86-91; 2010
- Susac JO. Susac Syndrome: the triad of microangiopathy of the brain and retina with hearing loss in young women. Neurology 44(4): 591-3; 1994
- Dörr J, Krautwald S, Wildemann B, Jarius S, Ringelstein M, Duning T, Aktas O, Ringelstein EB, Paul F, Kleffner I. Characteristics of Susac Syndrome: a review of all reported cases. Nat Rev Neurol 9(6): 307-16; 2013
- Groh S, One of three hundred - My Life with Susac Syndrome. ISBN 9783752679120
External links
| Classification |
|
|---|---|
| External resources |
|