Gastrointestinal perforation
| Gastrointestinal perforation | |
|---|---|
| Other names: Ruptured bowel,[1] gastrointestinal rupture | |
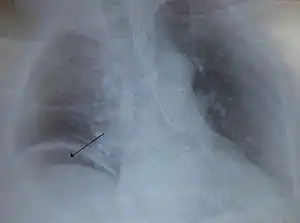 | |
| Free air under the right diaphragm from a perforated bowel. | |
| Specialty | Gastroenterology, emergency medicine |
| Symptoms | Abdominal pain, tenderness[2] |
| Complications | Sepsis, abscess[2] |
| Usual onset | Sudden or more gradual[2] |
| Causes | Trauma, following colonoscopy, bowel obstruction, colon cancer, diverticulitis, stomach ulcers, ischemic bowel, C. difficile infection[2] |
| Diagnostic method | CT scan, plain X-ray[2] |
| Treatment | Emergency surgery in the form of an exploratory laparotomy[2] |
| Medication | Intravenous fluids, antibiotics[2] |
| Prognosis | Risk of death up to 50%[2] |
Gastrointestinal perforation, also known as ruptured bowel,[1] is a hole in the wall of part of the gastrointestinal tract.[2] The gastrointestinal tract includes the esophagus, stomach, small intestine, and large intestine.[2][1] Symptoms include severe abdominal pain and tenderness.[2] When the hole is in the stomach or early part of the small intestine the onset of pain is typically sudden while with a hole in the large intestine onset may be more gradual.[2] The pain is usually constant in nature.[2] Sepsis, with an increased heart rate, increased breathing rate, fever, and confusion may occur.[2]
The cause can include trauma such as from a knife wound, eating a sharp object, or a medical procedure such as colonoscopy, bowel obstruction such as from a volvulus, colon cancer, or diverticulitis, stomach ulcers, ischemic bowel, and a number of infections including C. difficile.[2] A hole allows intestinal contents to enter the abdominal cavity.[2] The entry of bacteria results in a condition known as peritonitis or in the formation of an abscess.[2] A hole in the stomach can also lead to a chemical peritonitis due to gastric acid.[2] A CT scan is typically the preferred method of diagnosis; however, free air from a perforation can often be seen on plain X-ray.[2]
Perforation anywhere along the gastrointestinal tract typically requires emergency surgery in the form of an exploratory laparotomy.[2] This is usually carried out along with intravenous fluids and antibiotics.[2] A number of different antibiotics may be used such as piperacillin/tazobactam or the combination of ciprofloxacin and metronidazole.[3][4] Occasionally the hole can be sewn closed while other times a bowel resection is required.[2] Even with maximum treatment the risk of death can be as high as 50%.[2] A hole from a stomach ulcer occurs in about 1 per 10,000 people per year, while one from diverticulitis occurs in about 0.4 per 10,000 people per year.[1][5]
Signs and symptoms
Signs and symptoms may include a sudden pain in the epigastrium to the right of the midline indicating the perforation of a duodenal ulcer, while a gastric ulcer perforation reveals itself by burning pain in epigastrium, with flatulence and dyspepsia.
In intestinal perforation, pain starts from the site of perforation and spreads across the abdomen.
Gastrointestinal perforation results in severe abdominal pain intensified by movement, nausea, vomiting and hematemesis. Later symptoms include fever and or chills.[6] In any case, the abdomen becomes rigid with tenderness and rebound tenderness. After some time the abdomen becomes silent and heart sounds can be heard all over. Patient stops passing flatus and motion, abdomen is distended.
The symptoms of esophageal rupture may include sudden onset of chest pain.
Causes
Underlying causes include gastric ulcers, duodenal ulcers, appendicitis, gastrointestinal cancer, diverticulitis, inflammatory bowel disease, superior mesenteric artery syndrome, trauma, vascular Ehlers–Danlos syndrome,[7] and ascariasis. Typhoid fever,[8] non-steroidal anti-inflammatory drugs,[9][10] ingestion of corrosives may also be responsible.[11]
Eating multiple magnets can also lead to perforation if the magnets attract and stick to one another through different loops of the intestine.[12]
Diagnosis
On x-rays, gas may be visible in the abdominal cavity. Gas is easily visualized on x-ray while the patient is in an upright position. The perforation can often be visualised using computed tomography. White blood cells are often elevated.
Treatment
Surgical intervention is nearly always required in form of exploratory laparotomy and closure of perforation with peritoneal wash. Occasionally they may be managed laparoscopically.[13] A Graham patch may be used for duodenal perforations.
Conservative treatment including intravenous fluids, antibiotics, nasogastric aspiration and bowel rest is indicated only if the person is nontoxic and clinically stable.
References
- 1 2 3 4 Domino, Frank J.; Baldor, Robert A. (2013). The 5-Minute Clinical Consult 2014. Lippincott Williams & Wilkins. p. 1086. ISBN 9781451188509. Archived from the original on 17 August 2016. Retrieved 4 August 2016.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 Langell, JT; Mulvihill, SJ (May 2008). "Gastrointestinal perforation and the acute abdomen". The Medical Clinics of North America. 92 (3): 599–625, viii–ix. doi:10.1016/j.mcna.2007.12.004. PMID 18387378.
- ↑ Wong, PF; Gilliam, AD; Kumar, S; Shenfine, J; O'Dair, GN; Leaper, DJ (18 April 2005). "Antibiotic regimens for secondary peritonitis of gastrointestinal origin in adults". The Cochrane Database of Systematic Reviews (2): CD004539. doi:10.1002/14651858.CD004539.pub2. PMID 15846719.
- ↑ Wilson, William C.; Grande, Christopher M.; Hoyt, David B. (2007). Trauma: Resuscitation, Perioperative Management, and Critical Care. CRC Press. p. 882. ISBN 9781420015263. Archived from the original on 2016-08-17.
- ↑ Yeo, Charles J.; McFadden, David W.; Pemberton, John H.; Peters, Jeffrey H.; Matthews, Jeffrey B. (2012). Shackelford's Surgery of the Alimentary Tract (7 ed.). Elsevier Health Sciences. p. 701. ISBN 978-1455738076. Archived from the original on 2016-08-17.
- ↑ Ansari, Parswa. "Acute Perforation". Merck Manuals. Archived from the original on July 10, 2016. Retrieved June 30, 2016.
- ↑ Byers, Peter H. (21 February 2019). "Vascular Ehlers-Danlos Syndrome". University of Washington, Seattle. Archived from the original on 8 March 2021. Retrieved 8 January 2020.
- ↑ Sharma AK, Sharma RK, Sharma SK, Sharma A, Soni D (2013). "Typhoid Intestinal Perforation: 24 Perforations in One Patient". Annals of Medical and Health Sciences Research. 3 (Suppl1): S41–S43. doi:10.4103/2141-9248.121220. PMC 3853607. PMID 24349848.
- ↑ R I Russell (2001). "Non-steroidal anti-inflammatory drugs and gastrointestinal damage—problems and solutions". Postgrad Med J. 77 (904): 82–88. doi:10.1136/pmj.77.904.82. PMC 1741894. PMID 11161072. Archived from the original on 2016-07-01.
- ↑ Carlos Sostres; Carla J Gargallo; Angel Lanas (2013). "Nonsteroidal anti-inflammatory drugs and upper and lower gastrointestinal mucosal damage". Arthritis Res. Ther. 15 (Suppl 3): S3. doi:10.1186/ar4175. PMC 3890944. PMID 24267289.
- ↑ Ramasamy, Kovil; Gumaste, Vivek V. (2003). "Corrosive Ingestion in Adults". Journal of Clinical Gastroenterology. 37 (2): 119–124. doi:10.1097/00004836-200308000-00005. PMID 12869880.
- ↑ Lima, Mario (2016). Pediatric Digestive Surgery. Springer. p. 239. ISBN 9783319405254. Archived from the original on 2018-09-09. Retrieved 2018-09-09.
- ↑ Rustagi, T; McCarty, TR; Aslanian, HR (2015). "Endoscopic Treatment of Gastrointestinal Perforations, Leaks, and Fistulae". Journal of Clinical Gastroenterology. 49 (10): 804–9. doi:10.1097/mcg.0000000000000409. PMID 26325190.
External links
| Classification | |
|---|---|
| External resources |
- Gastrointestinal perforation Archived 2016-07-05 at the Wayback Machine—MedlinePlus