Lown–Ganong–Levine syndrome
Lown–Ganong–Levine syndrome (LGL) is a pre-excitation syndrome of the heart. Those with LGL syndrome have episodes of abnormal heart racing with a short PR interval and normal QRS complexes seen on their electrocardiogram when in a normal sinus rhythm. LGL syndrome was originally thought to be due to an abnormal electrical connection between the atria and the ventricles, but is now thought to be due to accelerated conduction through the atrioventricular node in the majority of cases.[1] The syndrome is named after Bernard Lown, William Francis Ganong, Jr., and Samuel A. Levine.[2][3]
Pathophysiology
LGL syndrome was originally thought to involve a rapidly conducting accessory pathway (bundle of James) that connects the atria directly to the bundle of His, bypassing the slowly conducting atrioventricular node.[1] However, the majority of those with LGL in whom electrophysiological studies have been performed do not have any evidence of an accessory pathway or structural abnormality. Whilst in a minority of cases some form of intranodal or paranodal fibers that bypass all or part of the atrioventricular node can be found with subsequent conduction down the normal His-Purkinje system, in most cases the short PR interval is caused by accelerated conduction through the atrioventricular node.[1] LGL syndrome is therefore felt to represent a clinical syndrome with multiple different underlying causes.
Diagnosis
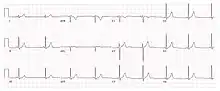
LGL syndrome is diagnosed in a person who has experienced episodes of abnormal heart racing (arrhythmias) who has a PR interval less than or equal to 0.12 second (120 ms) with normal QRS complex configuration and duration on their resting ECG.[1] A short PR interval found incidentally on an ECG without episodes of tachycardia is simply a benign ECG variant.
LGL can be distinguished from WPW syndrome because the delta waves seen in WPW syndrome are not seen in LGL syndrome. The QRS complex will also be narrow in LGL syndrome, as opposed to WPW, because ventricular conduction is via the His-Purkinje system. Lown–Ganong–Levine syndrome is a clinical diagnosis that came about before the advent of electrophysiology studies. It is important to be aware that not all WPW ECGs have a delta wave; the absence of a delta wave does not conclusively rule out WPW.
Prognosis
Individuals with LGL syndrome do not carry an increased risk of sudden death. The only morbidity associated with the syndrome is the occurrence of paroxysmal episodes of tachycardia which may be of several types, including sinus tachycardia, atrioventricular nodal re-entrant tachycardia, atrial fibrillation, or atrial flutter.[4]
See also
References
- 1 2 3 4 Josephson, Mark E. (2015-08-10). "Chapter 10 - Preexcitation syndromes". Josephson's clinical cardiac electrophysiology : techniques and interpretations. Preceded by: Josephson, Mark E. (Fifth ed.). Baltimore, MD. ISBN 9781496326614. OCLC 938434294.
- ↑ Rull G (2009). "Lown–Ganong–Levine Syndrome". Patient UK. EMIS. Retrieved 2011-05-29.
- ↑ Lown B, Ganong WF, Levine SA (May 1952). "The syndrome of short P-R interval, normal QRS complex and paroxysmal rapid heart action". Circulation. 5 (5): 693–706. doi:10.1161/01.cir.5.5.693. PMID 14926053.
- ↑ Wiener, Isaac (Sep 1, 1983). "Syndromes of Lown-Ganong-Levine and enhanced atrioventricular nodal conduction". Am J Cardiol. 52 (5): 637–639. doi:10.1016/0002-9149(83)90042-5. PMID 6613890.