Pseudoxanthoma elasticum
| Pseudoxanthoma elasticum | |
|---|---|
| Other names: Grönblad–Strandberg syndrome;[1] Groenblad-Strandberg syndrome | |
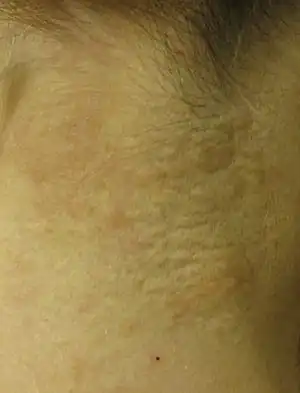 | |
| Pseudoxanthoma elasticum of the posterior lateral neck. Note the yellowish slightly raised bumps characteristic of this condition. | |
Pseudoxanthoma elasticum (PXE) is a genetic disease that causes mineralization of elastic fibers in some tissues. The most common problems arise in the skin and eyes, and later in blood vessels in the form of premature atherosclerosis.[2][3][4]
PXE is caused by autosomal recessive mutations in the ABCC6 gene on the short arm of chromosome 16 (16p13.1).[3][5][6]
Signs and symptoms
Usually, pseudoxanthoma elasticum affects the skin first, often in childhood or early adolescence.[7] Small, yellowish papular lesions form and cutaneous laxity mainly affect the neck, axillae (armpits), groin, and flexural creases (the inside parts of the elbows and knees).[3][8] Skin may become lax and redundant. Many individuals have "oblique mental creases" (horizontal grooves of the chin)[9]
PXE first affects the retina through a dimpling of the Bruch membrane (a thin membrane separating the blood vessel-rich layer from the pigmented layer of the retina), that is only visible during ophthalmologic examinations.[10] This is called peau d'orange (a French term meaning "skin of the orange"). Eventually the mineralization of the elastic fibers in the Bruch membrane create cracks called angioid streaks that radiate out from the optic nerve. Angioid streaks themselves do not cause distortion of vision, even if they cross into the foveal area. This symptom is present in almost all PXE patients and is usually noticed a few years after the onset of cutaneous lesions. These cracks may allow small blood vessels that were originally held back by Bruch's membrane to penetrate the retina. These blood vessels sometimes leak, and these retinal hemorrhages may lead to the loss of central vision. Vision loss is a major issue in many PXE patients.[11][3][4]
PXE may affect the gastrointestinal and cardiovascular systems. Gastrointestinal bleeding is a rare symptom and usually involved bleeding from the stomach. In the circulatory system, intermittent claudication, a condition in which cramping pain in the leg is induced by exercise, is a prominent feature.[12] At later stages, coronary artery disease may develop, leading to angina and myocardial infarction (heart attack).[13] Cerebral ischemia in PXE is caused by small vessel occlusive disease.
Other rare neurological complications may include intracranial aneurysms, subarachnoid and intracerebral hemorrhages.[14]
.jpg.webp) Pseudoxanthoma elasticum
Pseudoxanthoma elasticum.jpg.webp) Pseudoxanthoma elasticum
Pseudoxanthoma elasticum.jpg.webp) Pseudoxanthoma elasticum
Pseudoxanthoma elasticum Pseudoxanthoma elasticum of the posterior lateral neck.
Pseudoxanthoma elasticum of the posterior lateral neck. Pseudoxanthoma elasticum of the left axillary fold.
Pseudoxanthoma elasticum of the left axillary fold.
Genetics
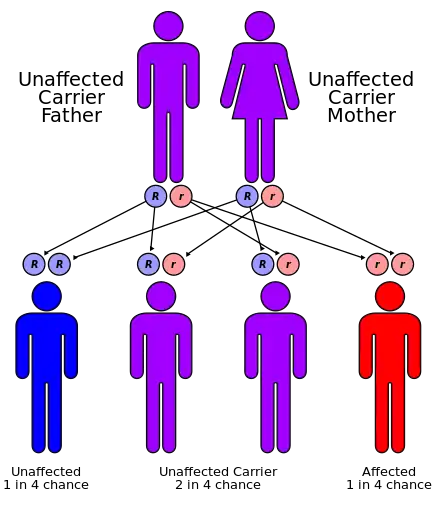
80% of clinical cases of pseudoxanthoma elasticum have detectable mutations in the ABCC6 gene.[15][16][17][18] Mutations in almost all parts of the gene have been described, of all types (missense, nonsense, splice alteration, insertion, small deletion or large deletion). Although there have been reports of autosomal dominant inheritance, the inheritance is typically autosomal recessive (both parents need to be carriers, and there is a 25% chance that a child will inherit both abnormal copies of the gene and therefore develop the condition).[3]
Strong genetic linkage was found with mutations in the ABCC6 gene, which codes for the ABCC6 protein, which is a membrane transporter from the large ATP-binding cassette transporter family. The protein is expressed in most organs, but mainly in the liver and kidney. ABCC6 mediates ATP release in the liver. This is the main source of circulating pyrophosphate (PPi), and individuals affected by PXE have strongly reduced plasma PPi levels, explaining their mineralization disorder.[19] One study suggested that mutations causing total absence of an ABCC6 protein caused a more severe disease,[20] but this could not be confirmed in a subsequent case series.[21] Given the variations in age of onset and severity it is likely that other unknown risk factors (genetic, environmental, and lifestyle) may be involved.[3]
Premature atherosclerosis is also associated with mutations in the ABCC6 gene, even in those without PXE.[22] A syndrome almost indistinguishable from hereditary PXE has been described in patients with hemoglobinopathies (sickle-cell disease and thalassemia) through a poorly understood mechanism.[3] In addition, there appears to be another PXE-like syndrome with a similar phenotype but as a result of problems with another gene, gamma-glutamyl carboxylase.[23] Mutations in ABCC6 can also cause generalized arterial calcification of infancy.[24] In some cases of PXE, mutations in ABCC6 cannot be found, and other genes such as ENPP1 may be implicated[25]
Pathophysiology
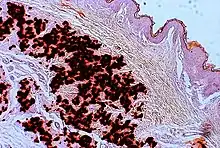
In PXE, there is mineralization (accumulation of calcium and other minerals) and fragmentation of the elastin-containing fibers in connective tissue, but primarily in the midlaminar layer of the dermis, Bruch's membrane and the midsized arteries.[26] Recent studies have confirmed that PXE is a metabolic disease, and that its features arise because metabolites of vitamin K cannot reach peripheral tissues.[27] Low levels of PPi cause mineralization in peripheral tissues.[19]
Diagnosis
The diagnostic criteria for PXE are the typical skin biopsy appearance and the presence of angioid streaks in the retina. Criteria were established by consensus of clinicians and researchers at the 2010 biennial research meeting of the PXE Research Consortium.[29] and confirmed at the 2014 meeting[30] These consensus criteria state that definitive PXE is characterized by two pathogenic mutations in the ABCC6 or ocular findings – angioid streaks > 1 DD or peau d’orange in an individual <20 years of age together with skin findings:
- Characteristic pseudoxanthomatous papules and plaques on the neck or flexural creases.
- Diagnostic histopathological changes in lesional skin: Calcified elastic fibers in the mid and lower dermis, confirmed by positive calcium stain
Differential diagnosis


| Pseudoxanthoma elasticum | LM: Mid-dermal calcification and fragmentation of elastic fibers EM: Mineralization in elastic fiber core |
| PXE-like disease with coagulation deficiency | LM: Middermal calcification and fragmentation of elastic fibers EM: Mineralization in elastic fiber periphery |
| Hemoglobinopathies | LM: Middermal calcification and fragmentation of elastic fibers EM: Mineralization in elastic fiber core |
| PXE-like papillary dermal elastolysis | LM: Selective elastic tissue elimination in the papillary dermis and presence of melanophages |
| White fibrous papulosis of the neck | LM: Dermal fibrosis in papillary and mid-reticular dermis |
| Late-onset focal dermal elastosis | EM: Decrease of elastic fibers; fragmentation of remaining fibers LM: Accumulation of elastic fibers in mid- and reticular dermis without fragmentation or calcification |
| Perforating calcific elastosis | LM: Middermal calcification and degeneration of elastic fibers with transepidermal elimination |
| Buschke-Ollendorff syndrome | LM: Increased amount of hypertrophic elastic fibers in dermis EM: Altered translucent elastic fibers |
| Elastosis perforans serpiginosa | LM: Transepidermal or perifollicular perforating canals |
| Papular elastorrhexis | LM: Thickening of collagen bundles next to loss and fragmentation of elastic fibers |
| Upper dermal elastolysis | LM: Complete loss of elastic fibers in the upper dermis |
| Middermal elastolysis | LM: Complete absence of elastic fibers in the middermis |
| Linear focal elastosis | LM: Massive basophilic fibers; clumping of elastic fibers in papillary dermis |
| Elastoderma | LM: Increased, intertwining thin elastic fibers in papillary and upper reticular dermis |
| Calcinosis cutis | LM: Deposits of calcium in the dermis |
Treatment
There is no confirmed treatment that directly interferes with the disease process.[5][6]
Cosmetic surgery to remove excessive skin has been used to improve aesthetic appearance in PXE patients[5] but because of the non-life-threatening nature of these symptoms, should be used with caution.[6]
One of the most critical symptom of PXE is choroidal neovascularization which can lead to deterioration of central vision. Photodynamic therapy has been used as a treatment, but this has been replaced with endothelial growth factor (VEGF) inhibitors (such as bevacizumab, ranibizumab, and aflibercept)[6] with efficacy similar to their use in treatment of age-related macular degeneration.[4]
To limit cardiovascular symptoms, reduction of cardiovascular risk factors through lifestyle changes is recommended.[6] Generally clinicians recommend avoidance of non-steroidal anti-inflammatory drugs (NSAIDS) that increase bleeding risk, such as aspirin, and ibuprofen to prevent eye and gastrointestinal bleeding.[6]
Formerly, dietary restriction of calcium was tried with no benefit, and in fact accelerated mineralization in mice.[31] There are a number of potential treatments that are currently being tested or have just undergone testing including magnesium,[32] etidronate,[33] PPi,[34] and tissue-nonspecific alkaline phosphatase inhibitors.[35]
Given that ABCC6 heterozygous mutations result in few symptoms of PXE, this disease is a candidate for gene therapy. Some initial proof-of-principle experiments have been done in mice that have relieved some of symptoms of PXE, but as with all gene therapy treatments, there are many hurdles that must be over come including insuring that the treatment will be long-lasting and reducing the risk of insertional mutagenesis and severe immune reactions.[6]
Epidemiology
The reported prevalence of pseudoxanthoma elasticum is about 1:25,000. Females are twice as likely to be affected as males. The disease occurs in all ethnicities, but Afrikaners are more likely to have PXE as a result of a founder effect (i.e., higher prevalence in the small group of people from whom Afrikaners descend).[36]
History
The first description of PXE that distinguished it from other xanthoma conditions was by Dr Ferdinand-Jean Darrier in 1896.[37] The eponym "Grönblad-Strandberg syndrome" is used in older literature, after two physicians who made further discoveries in the disease manifestations.[38]
PXE has the distinction of being the only disease for which a layperson is the discover of the mutated gene. The ABCC6 gene mutation was discovered simultaneously by four research teams, all of which published at the same time. The principal investigators were (in order of the date of publication): Jouni Uitto,[15] Arthur Bergen,[16] Charles Boyd,[17] and Klaus Lindpainter.[18] The gene was patented by Charles D. Boyd, Katalin Csiszar, Olivier LeSaux, Zsolt Urban, Sharon Terry, and assigned to PXE International by these co-inventors. Between the filing and 2013, when the Supreme Court of the United States declared that genes may not be patented.[39] PXE International freely licensed the gene to any lab for clinical testing and research. PXE International continues to hold and maintain other patents (diagnosis and treatment patents).[40][41]
PXE International, a support organization, was founded in 1995, by Patrick and Sharon Terry,[42][43][44][45] following the diagnosis of their two children. It has a registry of 4,600 affected individuals.
See also
References
- ↑ Rapini RP, Bolognia JL, Jorizzo JL (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 978-1-4160-2999-1.
- ↑ Li Q, van de Wetering K, Uitto J (February 2019). "Pseudoxanthoma Elasticum as a Paradigm of Heritable Ectopic Mineralization Disorders: Pathomechanisms and Treatment Development". review. The American Journal of Pathology. 189 (2): 216–225. doi:10.1016/j.ajpath.2018.09.014. PMC 6412714. PMID 30414410.
- 1 2 3 4 5 6 7 Chassaing N, Martin L, Calvas P, Le Bert M, Hovnanian A (December 2005). "Pseudoxanthoma elasticum: a clinical, pathophysiological and genetic update including 11 novel ABCC6 mutations". review. Journal of Medical Genetics. 42 (12): 881–92. doi:10.1136/jmg.2004.030171. PMC 1735972. PMID 15894595.
- 1 2 3 Finger RP, Charbel Issa P, Ladewig MS, Götting C, Szliska C, Scholl HP, Holz FG (2009). "Pseudoxanthoma elasticum: genetics, clinical manifestations and therapeutic approaches". review. Survey of Ophthalmology. 54 (2): 272–85. doi:10.1016/j.survophthal.2008.12.006. PMID 19298904.
- 1 2 3 Marconi B, Bobyr I, Campanati A, Molinelli E, Consales V, Brisigotti V, et al. (August 2015). "Pseudoxanthoma elasticum and skin: Clinical manifestations, histopathology, pathomechanism, perspectives of treatment". review. Intractable & Rare Diseases Research. 4 (3): 113–22. doi:10.5582/irdr.2015.01014. PMC 4561240. PMID 26361562.
- 1 2 3 4 5 6 7 Germain DP (May 2017). "Pseudoxanthoma elasticum". review. Orphanet Journal of Rare Diseases. 12 (1): 85. doi:10.1186/s13023-017-0639-8. PMC 5424392. PMID 28486967.
- ↑ Naouri M, Boisseau C, Bonicel P, Daudon P, Bonneau D, Chassaing N, Martin L (September 2009). "Manifestations of pseudoxanthoma elasticum in childhood". The British Journal of Dermatology. 161 (3): 635–9. doi:10.1111/j.1365-2133.2009.09298.x. PMID 19519828.
- ↑ Neldner KH, Struk B (2003). Pseudoxanthoma Elasticum. Connective Tissue and Its Heritable Disorders. John Wiley & Sons, Ltd. pp. 561–583. doi:10.1002/0471221929.ch11. ISBN 9780471221920.
- ↑ Lebwohl M, Lebwohl E, Bercovitch L (April 2003). "Prominent mental (chin) crease: a new sign of pseudoxanthoma elasticum". primary. Journal of the American Academy of Dermatology. 48 (4): 620–2. doi:10.1067/mjd.2003.195. PMID 12664032. Archived from the original on 2021-08-29. Retrieved 2021-07-06.
- ↑ Gliem M, Müller PL, Birtel J, Hendig D, Holz FG, Charbel Issa P (June 2016). "Frequency, Phenotypic Characteristics and Progression of Atrophy Associated With a Diseased Bruch's Membrane in Pseudoxanthoma Elasticum". primary. Investigative Ophthalmology & Visual Science. 57 (7): 3323–30. doi:10.1167/iovs.16-19388. PMID 27367499.
- ↑ Risseeuw S, Ossewaarde-van Norel J, Klaver CC, Colijn JM, Imhof SM, van Leeuwen R (August 2019). "Visual Acuity in Pseudoxanthoma Elasticum". primary. Retina. 39 (8): 1580–1587. doi:10.1097/IAE.0000000000002173. PMID 29652691.
- ↑ Lefthériotis G, Abraham P, Le Corre Y, Le Saux O, Henrion D, Ducluzeau PH, et al. (November 2011). "Relationship between ankle brachial index and arterial remodeling in pseudoxanthoma elasticum". primary. Journal of Vascular Surgery. 54 (5): 1390–4. doi:10.1016/j.jvs.2011.04.041. PMC 5529101. PMID 21723076.
- ↑ Kranenburg G, de Jong PA, Mali WP, Attrach M, Visseren FL, Spiering W (January 2017). "Prevalence and severity of arterial calcifications in pseudoxanthoma elasticum (PXE) compared to hospital controls. Novel insights into the vascular phenotype of PXE". primary. Atherosclerosis. 256: 7–14. doi:10.1016/j.atherosclerosis.2016.11.012. PMID 27940376.
- ↑ Kauw F, Kranenburg G, Kappelle LJ, Hendrikse J, Koek HL, Visseren FL, et al. (February 2017). "Cerebral disease in a nationwide Dutch pseudoxanthoma elasticum cohort with a systematic review of the literature". review. Journal of the Neurological Sciences. 373: 167–172. doi:10.1016/j.jns.2016.12.053. PMID 28131180.
- 1 2 Ringpfeil F, Lebwohl MG, Christiano AM, Uitto J (May 2000). "Pseudoxanthoma elasticum: mutations in the MRP6 gene encoding a transmembrane ATP-binding cassette (ABC) transporter". primary. Proceedings of the National Academy of Sciences of the United States of America. 97 (11): 6001–6. Bibcode:2000PNAS...97.6001R. doi:10.1073/pnas.100041297. PMC 18548. PMID 10811882.
- 1 2 Bergen AA, Plomp AS, Schuurman EJ, Terry S, Breuning M, Dauwerse H, et al. (June 2000). "Mutations in ABCC6 cause pseudoxanthoma elasticum". primary. Nature Genetics. 25 (2): 228–31. doi:10.1038/76109. PMID 10835643.
- 1 2 Le Saux O, Urban Z, Tschuch C, Csiszar K, Bacchelli B, Quaglino D, et al. (June 2000). "Mutations in a gene encoding an ABC transporter cause pseudoxanthoma elasticum". primary. Nature Genetics. 25 (2): 223–7. doi:10.1038/76102. PMID 10835642.
- 1 2 Struk B, Cai L, Zäch S, Ji W, Chung J, Lumsden A, et al. (2000). "Mutations of the gene encoding the transmembrane transporter protein ABC-C6 cause pseudoxanthoma elasticum". primary. Journal of Molecular Medicine. 78 (5): 282–6. doi:10.1007/s001090000114. PMID 10954200.
- 1 2 Jansen RS, Duijst S, Mahakena S, Sommer D, Szeri F, Váradi A, et al. (September 2014). "ABCC6-mediated ATP secretion by the liver is the main source of the mineralization inhibitor inorganic pyrophosphate in the systemic circulation-brief report". primary. Arteriosclerosis, Thrombosis, and Vascular Biology. 34 (9): 1985–9. doi:10.1161/ATVBAHA.114.304017. PMC 6743317. PMID 24969777.
- ↑ Schulz V, Hendig D, Szliska C, Götting C, Kleesiek K (June 2005). "Novel mutations in the ABCC6 gene of German patients with pseudoxanthoma elasticum". primary. Human Biology. 77 (3): 367–84. doi:10.1353/hub.2005.0054. PMID 16392638.
- ↑ Pfendner EG, Vanakker OM, Terry SF, Vourthis S, McAndrew PE, McClain MR, et al. (October 2007). "Mutation detection in the ABCC6 gene and genotype-phenotype analysis in a large international case series affected by pseudoxanthoma elasticum". primary. Journal of Medical Genetics. 44 (10): 621–8. doi:10.1136/jmg.2007.051094. PMC 2597973. PMID 17617515.
- ↑ Trip MD, Smulders YM, Wegman JJ, Hu X, Boer JM, ten Brink JB, et al. (August 2002). "Frequent mutation in the ABCC6 gene (R1141X) is associated with a strong increase in the prevalence of coronary artery disease". primary. Circulation. 106 (7): 773–5. doi:10.1161/01.CIR.0000028420.27813.C0. PMID 12176944.
- ↑ Vanakker OM, Martin L, Gheduzzi D, Leroy BP, Loeys BL, Guerci VI, et al. (March 2007). "Pseudoxanthoma elasticum-like phenotype with cutis laxa and multiple coagulation factor deficiency represents a separate genetic entity". primary. The Journal of Investigative Dermatology. 127 (3): 581–7. doi:10.1038/sj.jid.5700610. PMID 17110937.
- ↑ Li Q, Brodsky JL, Conlin LK, Pawel B, Glatz AC, Gafni RI, et al. (March 2014). "Mutations in the ABCC6 gene as a cause of generalized arterial calcification of infancy: genotypic overlap with pseudoxanthoma elasticum". primary. The Journal of Investigative Dermatology. 134 (3): 658–665. doi:10.1038/jid.2013.370. PMC 3945730. PMID 24008425.
- ↑ Jin L, Jiang Q, Wu Z, Shao C, Zhou Y, Yang L, et al. (May 2015). "Genetic heterogeneity of pseudoxanthoma elasticum: the Chinese signature profile of ABCC6 and ENPP1 mutations". primary. The Journal of Investigative Dermatology. 135 (5): 1294–1302. doi:10.1038/jid.2015.10. PMC 4402129. PMID 25615550.
- ↑ Gheduzzi D, Sammarco R, Quaglino D, Bercovitch L, Terry S, Taylor W, Ronchetti IP (2003). "Extracutaneous ultrastructural alterations in pseudoxanthoma elasticum". primary. Ultrastructural Pathology. 27 (6): 375–84. doi:10.1080/716100800. PMID 14660276.
- ↑ Li Q, Jiang Q, Pfendner E, Váradi A, Uitto J (January 2009). "Pseudoxanthoma elasticum: clinical phenotypes, molecular genetics and putative pathomechanisms". review. Experimental Dermatology. 18 (1): 1–11. doi:10.1111/j.1600-0625.2008.00795.x. PMC 3349969. PMID 19054062.
- 1 2 3 4 Hosen, Mohammad J.; Lamoen, Anouck; De Paepe, Anne; Vanakker, Olivier M. (2012). "Histopathology of Pseudoxanthoma Elasticum and Related Disorders: Histological Hallmarks and Diagnostic Clues". Scientifica. 2012: 1–15. doi:10.6064/2012/598262. ISSN 2090-908X. PMC 3820553. PMID 24278718.
-Creative Commons Attribution 3.0 Unported Archived 2011-02-23 at the Wayback Machine license - ↑ Uitto J, Bercovitch L, Terry SF, Terry PF (July 2011). "Pseudoxanthoma elasticum: progress in diagnostics and research towards treatment : Summary of the 2010 PXE International Research Meeting". review. American Journal of Medical Genetics. Part A. 155A (7): 1517–26. doi:10.1002/ajmg.a.34067. PMC 3121926. PMID 21671388.
- ↑ Uitto J, Jiang Q, Váradi A, Bercovitch LG, Terry SF (June 2014). "Visual Acuity in Pseudoxanthoma Elasticum". review. Expert Opinion on Orphan Drugs. 2 (6): 567–577. doi:10.1517/21678707.2014.908702. PMC 4219573. PMID 25383264.
- ↑ Jiang Q, Uitto J (September 2012). "Restricting dietary magnesium accelerates ectopic connective tissue mineralization in a mouse model of pseudoxanthoma elasticum (Abcc6(-/-) )". primary. Experimental Dermatology. 21 (9): 694–9. doi:10.1111/j.1600-0625.2012.01553.x. PMC 3422765. PMID 22897576.
- ↑ Rose S, On SJ, Fuchs W, Chen C, Phelps R, Kornreich D, et al. (July 2019). "Magnesium supplementation in the treatment of pseudoxanthoma elasticum: A randomized trial". primary. Journal of the American Academy of Dermatology. 81 (1): 263–265. doi:10.1016/j.jaad.2019.02.055. PMID 30826287.
- ↑ Kranenburg G, de Jong PA, Bartstra JW, Lagerweij SJ, Lam MG, Ossewaarde-van Norel J, et al. (March 2018). "Etidronate for Prevention of Ectopic Mineralization in Patients With Pseudoxanthoma Elasticum". primary. Journal of the American College of Cardiology. 71 (10): 1117–1126. doi:10.1016/j.jacc.2017.12.062. PMID 29519353.
- ↑ Dedinszki D, Szeri F, Kozák E, Pomozi V, Tőkési N, Mezei TR, et al. (November 2017). "Oral administration of pyrophosphate inhibits connective tissue calcification". primary. EMBO Molecular Medicine. 9 (11): 1463–1470. doi:10.15252/emmm.201707532. PMC 5666306. PMID 28701330.
- ↑ Li Q, Huang J, Pinkerton AB, Millan JL, van Zelst BD, Levine MA, et al. (February 2019). "-/- Mouse Model of PXE but Not in the Enpp1 Mutant Mouse Models of GACI". primary. The Journal of Investigative Dermatology. 139 (2): 360–368. doi:10.1016/j.jid.2018.07.030. PMC 6342656. PMID 30130617.
- ↑ Le Saux O, Beck K, Sachsinger C, Treiber C, Göring HH, Curry K, et al. (October 2002). "Evidence for a founder effect for pseudoxanthoma elasticum in the Afrikaner population of South Africa". primary. Human Genetics. 111 (4–5): 331–8. doi:10.1007/s00439-002-0808-1. PMID 12384774.
- ↑ Darrier FJ (1896). "Pseudoxanthoma elasticum". Monatschr Prakt Dermatol (in German). 23: 609–17.
{{cite journal}}: CS1 maint: unrecognized language (link) - ↑ synd/1059 at Who Named It?
- ↑ Liptak A (2013-06-13). "Justices, 9-0, Bar Patenting Human Genes". The New York Times. ISSN 0362-4331. Archived from the original on 2015-02-26. Retrieved 2019-08-24.
- ↑ Katalin Csiszar, Olivier LeSaux, Zsolt Urban, Sharon Terry, Charles D. Boyd. United States Patent and Trademark Office. "Methods and Composition for Diagnosing and Treating Pseudoxanthoma Elasticum and Related Conditions". assignment.uspto.gov. Archived from the original on 2020-04-20. Retrieved 2019-08-24.
{{cite web}}: CS1 maint: uses authors parameter (link) - ↑ Charles D. Boyd, Katalin Csiszar, Olivier LeSaux, Zsolt Urban, Sharon Terry. United States Patent and Trademark Office =. "Methods for Diagnosing Pseudoxanthoma Elasticum". assignment.uspto.gov. Archived from the original on 2020-04-20. Retrieved 2019-08-24.
{{cite web}}: CS1 maint: uses authors parameter (link) - ↑ Terry SF (2003). "Learning genetics". Health Affairs. 22 (5): 166–71. doi:10.1377/hlthaff.22.5.166. PMID 14515892.
- ↑ Terry SF (March 2016). "Life as a numerator: Putting the person in personal genomics". Applied & Translational Genomics. 8: 40–1. doi:10.1016/j.atg.2016.01.007. PMC 4796705. PMID 27047760.
- ↑ Terry S, Science didn't understand my kids' rare disease until I decided to study it, archived from the original on 2019-08-16, retrieved 2019-08-24
- ↑ "Sharon Terry: When Siblings Get A Rare Diagnosis, Can Their Parents Find the Cure? TED Radio Hour". NPR.org. Archived from the original on 2019-12-23. Retrieved 2019-08-24.
External links
- PXE international Archived 2021-07-13 at the Wayback Machine
| Classification | |
|---|---|
| External resources |
- pxe at NIH/UW GeneTests
- Pseudoxanthoma elasticum at NLM Genetics Home Reference