Transient ischemic attack
| Transient ischemic attack | |
|---|---|
| Other names: Mini-strokes | |
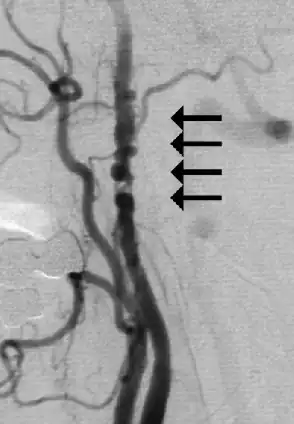 | |
| Angiogram showing narrowing of the arteries in the neck in a women with a TIA[1] | |
| Specialty | Neurology, vascular surgery |
| Symptoms | Weakness or numbness on one side, sudden loss of vision, difficulty talking or understanding, poor coordination, confusion[2] |
| Complications | Stroke[3] |
| Usual onset | Sudden[2] |
| Duration | < 1 hr[2] |
| Risk factors | Diabetes, high blood pressure, smoking, alcoholism, psychological stress, lack of exercise[3] |
| Diagnostic method | Based on symptoms and medical imaging[4] |
| Differential diagnosis | Bells palsy, migraine, carotid artery dissection, multiple sclerosis, syncope, stroke, meningitis[3] |
| Treatment | Lifestyle changes, medications, surgery[3] |
| Prognosis | Survival ~ 91% (hospital discharge) 67% (five yr)[5] |
| Frequency | 1 per 1,000 per yr[3] |
Transient ischemic attack (TIA), also known as a mini-stroke, is a brief episode of neurological dysfunction caused by lack of blood flow (ischemia) to an area of the brain or retina, without tissue death.[4] It results in the same symptoms as a stroke, such as weakness or numbness on one side of the body, sudden loss of vision, difficulty talking or understanding speech, poor coordination, or confusion.[2] Symptoms generally start suddenly and last less than an hour.[2]
Risk factors include diabetes, high blood pressure, smoking, alcoholism, psychological stress, and lack of exercise.[3] TIAs have a similar underlying mechanism as ischemic strokes.[3] The definition was previously based a duration of symptoms of less than 24 hours; with newer definitions also include no evidence of infarction on medical imaging.[4]
It is a medical emergency.[3] Treatment may include lifestyle changes such as stopping smoking and limiting alcohol, as well as medications such as aspirin, clopidogrel, or anticoagulants (blood thinners).[2][6] Other measures include blood pressure management, statins, and blood sugar control.[3] In people with narrowing of the arteries in their neck, a carotid endarterectomy may be indicated.[3] About a third of people who have a TIA have a stroke in the future.[2]
About 2% of people have previously had a TIA and 1 per 1,000 people are newly affected per year.[3] Older people (> 60 years) are more commonly affected.[3][7] Males are more commonly affected than females.[7] TIAs were first described around 400 BC by Hippocrates and noted to be a risk factor for later stroke.[8]
Signs and symptoms
Signs and symptoms of TIA are widely variable and can mimic other neurologic conditions, making the clinical context and physical exam crucial in ruling in or out the diagnosis. The most common presenting symptoms of TIA are focal neurologic deficits, which can include, but are not limited to:[9]
- Amaurosis fugax (painless, temporary loss of vision)
- One-sided facial droop
- One-sided motor weakness
- Diplopia (double vision)
- Problems with balance and spatial orientation or dizziness
- Visual field deficits, such as homonymous hemianopsia or monocular blindness[10]
- Sensory deficits in one or more limbs and of the face[10]
- Loss of ability to understand or express speech (aphasia)[10]
- Difficulty with articulation of speech (dysarthria)[10]
- Unsteady gait[10]
- Difficulties with swallowing (dysphagia)[10]
A detailed neurologic exam, including a thorough cranial nerve exam, is important to identify these findings and to differentiate them from mimickers of TIA. Symptoms such as unilateral weakness, amaurosis fugax, and double vision have higher odds of representing TIA compared to memory loss, headache, and blurred vision.[11] Below is a table of symptoms at presentation, and what percentage of the time they are seen in TIAs versus conditions that mimic TIA. In general, focal deficits make TIA more likely, but the absence of focal findings do not exclude the diagnosis and further evaluation may be warranted if clinical suspicion for TIA is high (see "Diagnosis" section below).[12]
Cause
The most common underlying pathology leading to TIA and stroke is a cardiac condition called atrial fibrillation, where poor coordination of contraction leads to a formation of a clot in the atrial chamber that can become dislodged and travel to a cerebral artery.[13][14] Unlike in stroke, the blood flow can become restored prior to infarction which leads to the resolution of neurologic symptoms.[9][13] Another common culprit of TIA is an atherosclerotic plaque located in the common carotid artery, typically by the bifurcation between the internal and external carotids, that becomes an embolism to the brain vasculature similar to the clot in the prior example.[13][14] A portion of the plaque can become dislodged and lead to embolic pathology in the cerebral vessels.[13]
In-situ thrombosis, an obstruction that forms directly in the cerebral vasculature unlike the remote embolism previously mentioned, is another vascular occurrence with possible presentation as TIA.[13] Also, carotid stenosis secondary to atherosclerosis narrowing the diameter of the lumen and thus limiting blood flow is another common cause of TIA.[13] Individuals with carotid stenosis may present with TIA symptoms, thus labeled symptomatic, while others may not experience symptoms and be asymptomatic.[9][13][14]
Risk factors
Risk factors associated with TIA are categorized as modifiable or non-modifiable. Non-modifiable risk factors include age greater than 55, sex, family history, genetics, and race/ethnicity.[13][15] Modifiable risk factors include cigarette smoking, hypertension (elevated blood pressure), diabetes, hyperlipidemia, level of carotid artery stenosis (asymptomatic or symptomatic) and activity level.[13][14][15] The modifiable risk factors are commonly targeted in treatment options to attempt to minimize risk of TIA and stroke.[4][13][14]
Pathogenesis
There are three major mechanisms of ischemia in the brain: embolism traveling to the brain, in situ thrombotic occlusion in the intracranial vessels supplying the parenchyma of the brain, and stenosis of vessels leading to poor perfusion secondary to flow-limiting diameter.[13][14] Globally, the vessel most commonly affected is the middle cerebral artery.[13] Embolisms can originate from multiple parts of the body.
Common mechanisms of stroke and TIA:[13]
| Stroke mechanism | Frequency | Pattern of infarcts | Number of infarct |
|---|---|---|---|
| In situ thrombotic occlusion | Uncommon | Large subcortical; Sometimes with borderzone; Rarely, whole territory | Sometimes enlarging;
Single |
| Artery to artery embolism | Common | Small cortical and subcortical | Multiple |
| Impaired clearance of emboli | Common | Small, scattered, alongside the borderzone region | Multiple |
| Branch occlusive disease | Common | Small subcortical, lacune-like | Single |
| Hemodynamic | Uncommon | Borderzone;
May be without lesion |
Multiple; None |
Diagnosis
.png.webp)
The initial clinical evaluation of a suspected TIA involves obtaining a history and physical exam (including a neurological exam).[10] History taking includes defining the symptoms and looking for mimicking symptoms as described above. Bystanders can be very helpful in describing the symptoms and giving details about when they started and how long they lasted. The time course (onset, duration, and resolution), precipitating events, and risk factors are particularly important.
Lab test
Laboratory tests should focus on ruling out metabolic conditions that may mimic TIA (e.g. hypoglycemia causing altered mental status), in addition to further evaluating a patient's risk factors for ischemic events. All patients should receive a complete blood count with platelet count, blood glucose, basic metabolic panel, prothrombin time/international normalized ratio, and activated partial thromboplastin time as part of their initial workup.[16] These tests help with screening for bleeding or hypercoagulable conditions. Other lab tests, such as a full hypercoagulable state workup or serum drug screening, should be considered based on the clinical situation and factors, such as age of the patient and family history.[12] A fasting lipid panel is also appropriate to thoroughly evaluate the patient's risk for atherosclerotic disease and ischemic events in the future.[12] Other lab tests may be indicated based on the history and presentation; such as obtaining inflammatory markers (erythrocyte sedimentation rate and C-reactive protein) to evaluate for giant cell arteritis (which can mimic a TIA) in those presenting with headaches and monocular blindness.[10]
Heart rhythm
An electrocardiogram is necessary to rule out abnormal heart rhythms, such as atrial fibrillation, that can predispose patients to clot formation and embolic events.[16] Hospitalized patients should be placed on heart rhythm telemetry, which is a continuous form of monitoring that can detect abnormal heart rhythms.[10] Prolonged heart rhythm monitoring (such as with a Holter monitor or implantable heart monitoring) can be considered to rule out arrhythmias like paroxysmal atrial fibrillation that may lead to clot formation and TIAs, however this should be considered if other causes of TIA have not been found.[12][4]
Imaging
According to guidelines from the American Heart Association and American Stroke Association Stroke Council, patients with TIA should have head imaging "within 24 hours of symptom onset, preferably with magnetic resonance imaging, including diffusion sequences".[4] MRI is a better imaging modality for TIA than computed tomography (CT), as it is better able to pick up both new and old ischemic lesions than CT. CT, however, is more widely available and can be used particularly to rule out intracranial hemorrhage.[12] Diffusion sequences can help further localize the area of ischemia and can serve as prognostic indicators.[16] Presence of ischemic lesions on diffusion weighted imaging has been correlated with a higher risk of stroke after a TIA.[17]
Vessels in the head and neck may also be evaluated to look for atherosclerotic lesions that may benefit from interventions, such as carotid endarterectomy. The vasculature can be evaluated through the following imaging modalities: magnetic resonance angiography (MRA), CT angiography (CTA), and carotid ultrasonography/transcranial doppler ultrasonography.[4] Carotid ultrasonography is often used to screen for carotid artery stenosis, as it is more readily available, is noninvasive, and does not expose the person being evaluated to radiation. However, all of the above imaging methods have variable sensitivities and specificities, making it important to supplement one of the imaging methods with another to help confirm the diagnosis (for example: screen for the disease with ultrasonography, and confirm with CTA).[18] Confirming a diagnosis of carotid artery stenosis is important because the treatment for this condition, carotid endarterectomy, can pose significant risk to the patient, including heart attacks and strokes after the procedure.[18] For this reason, the U.S. Preventive Services Task Force (USPSTF) "recommends against screening for asymptomatic carotid artery stenosis in the general adult population".[18] This recommendation is for asymptomatic patients, so it does not necessarily apply to patients with TIAs as these may in fact be a symptom of underlying carotid artery disease (see "Causes and Pathogenesis" above). Therefore, patients who have had a TIA may opt to have a discussion with their clinician about the risks and benefits of screening for carotid artery stenosis, including the risks of surgical treatment of this condition.
Cardiac imaging can be performed if head and neck imaging do not reveal a vascular cause for the patient's TIA (such as atherosclerosis of the carotid artery or other major vessels of the head and neck). Echocardiography can be performed to identify patent foramen ovale (PFO), valvular stenosis, and atherosclerosis of the aortic arch that could be sources of clots causing TIAs, with transesophageal echocardiography being more sensitive than transthoracic echocardiography in identifying these lesions.[4]
Differential diagnosis
| Symptoms[12] | % mimics[12] | % TIAs[12] |
|---|---|---|
| Unilateral paresis | 29 | 58 |
| Memory loss/cognitive impairment | 18 to 26 | 2 to 12 |
| Headache | 15 to 23 | 2 to 36 |
| Blurred vision | 22 | 5 |
| Dysarthria | 13 | 21 |
| Hemianopia | 4 | 4 |
| Transient monocular blindness | 0 | 6 |
| Diplopia | 0 | 5 |
Non-focal symptoms such as amnesia, confusion, incoordination of limbs, unusual cortical visual symptoms (such as isolated bilateral blindness or bilateral positive visual phenomena), headaches and transient loss of consciousness are usually not associated with TIA,[10] however assessment is still needed. Public awareness on the need to seek a medical assessment for these non-focal symptoms is also low, and can result in a delay by people to seek treatment [19]
Symptoms of TIAs can last on the order of minutes to one–two hours, but occasionally may last for a longer period of time.[20][4] TIAs used to be defined as ischemic events in the brain that last less than 24 hours, but given the variation in duration of symptoms, this definition holds less significance.[4] A pooled study of 808 people with TIAs from 10 hospitals showed that 60% lasted less than one hour, 71% lasted less than two hours, and 14% lasted greater than six hours.[21] People with symptoms that last more than one hour are more likely to have permanent neurologic damage, making prompt diagnosis and treatment important to maximize recovery.[4]
| Diagnosis[12] | Findings[12] |
| Brain tumor | Severe unilateral headache with nausea and vomiting |
| Central nervous system infection (e.g., meningitis, encephalitis) | Fever, headache, confusion, neck stiffness, nausea, vomiting, photophobia, change in mental status |
| Falls/trauma | Headache, confusion, bruising |
| Hypoglycemia | Confusion, weakness, diaphoresis |
| Migraines | Severe headaches with or without photophobia, younger age |
| Multiple sclerosis | Diplopia, limb weakness, paresthesia, urinary retention, optic neuritis |
| Seizure disorder | Confusion with or without loss of consciousness, urinary incontinence, tongue biting, tonic-clonic movements |
| Subarachnoid hemorrhage | Severe headache with sudden onset and photophobia |
| Vertigo (central or peripheral) | Generalized dizziness and diaphoresis with or without hearing loss |
Prevention
Although there is a lack of robust studies demonstrating the efficacy of lifestyle changes in preventing TIA, many medical professionals recommend them.[22] These include:
- Avoiding smoking
- Cutting down on fats to help reduce the amount of plaque buildup
- Eating a healthy diet including plenty of fruits and vegetables
- Limiting sodium in the diet, thereby reducing blood pressure
- Exercising regularly
- Moderating intake of alcohol, stimulants, sympathomimetics, etc.
- Maintaining a healthy weight
In addition, it is important to control any underlying medical conditions that may increase the risk of stroke or TIA, including:[22]
- Hypertension
- High cholesterol
- Diabetes mellitus
- Atrial fibrillation
Treatment
By definition, TIAs are transient, self-resolving, and do not cause permanent impairment. However, they are associated with an increased risk of subsequent ischemic strokes, which can be permanently disabling.[23] Therefore, management centers on the prevention of future ischemic strokes and addressing any modifiable risk factors. The optimal regimen depends on the underlying cause of the TIA.
Lifestyle
Lifestyle changes have not been shown to reduce the risk of stroke after TIA.[24] While no studies have looked at the optimal diet for secondary prevention of stroke, some observational studies have shown that a Mediterranean diet can reduce stroke risk in patients without cerebrovascular disease.[25] A Mediterranean diet is rich in fruits, vegetables and whole grains, and limited in red meats and sweets. Vitamin supplementation has not been found to be useful in secondary stroke prevention.[25]
Antiplatelets
The antiplatelet medications, aspirin and clopidogrel, are recommended together for secondary prevention of stroke after high-risk TIAs.[25][26] The clopidogrel can generally be stopped after 10 to 21 days.[26][6] An exception is TIAs due to blood clots originating from the heart, in which case anticoagulants are generally recommended.[25] After TIA or minor stroke, aspirin therapy has been shown to reduce the short-term risk of recurrent stroke by 60–70%, and the long-term risk of stroke by 13%.[27]
Anticoagulants
Anticoagulants may be started if the TIA is thought to be attributable to atrial fibrillation. Atrial fibrillation is an abnormal heart rhythm that may cause the formation of blood clots that can travel to the brain, resulting in TIAs or ischemic strokes. Atrial fibrillation increases stroke risk by five times, and is thought to cause 10-12% of all ischemic strokes in the US.[25][28] Anticoagulant therapy can decrease the relative risk of ischemic stroke in those with atrial fibrillation by 67%[29] Warfarin is a common anticoagulant used, but direct acting oral anticoagulants (DOACs), such as apixaban, have been shown to be equally effective while also conferring a lower risk of bleeding.[28][30] Generally, anticoagulants and antiplatelets are not used in combination, as they result in increased bleeding risk without a decrease in stroke risk.[25] However, combined antiplatelet and anticoagulant therapy may be warranted if the patient has symptomatic coronary artery disease in addition to atrial fibrillation.
Sometimes, myocardial infarction ("heart attack") may lead to the formation of a blood clot in one of the chambers of the heart. If this is thought to be the cause of the TIA, people may be temporarily treated with warfarin or other anticoagulant to decrease the risk of future stroke.[25]
Blood pressure control
Blood pressure control may be indicated after TIA to reduce the risk of ischemic stroke. About 70% of patients with recent ischemic stroke are found to have hypertension, defined as systolic blood pressure (SBP) > 140 mmHg, or diastolic blood pressure (DBP) > 90 mmHg.[25] Until the first half of the 2010s, blood pressure goals have generally been SBP < 140 mmHg and DBP < 90 mmHg.[25] However, newer studies suggest that a goal of SBP <130 mmHg may confer even greater benefit.[31][32] Blood pressure control is often achieved using diuretics or a combination of diuretics and angiotensin converter enzyme inhibitors, although the optimal treatment regimen depends on the individual.[25]
Cholesterol control
There is inconsistent evidence regarding the effect of LDL-cholesterol levels on stroke risk after TIA. Elevated cholesterol may increase ischemic stroke risk while decreasing the risk of hemorrhagic stroke.[33][34][35] While its role in stroke prevention is currently unclear, statin therapy has been shown to reduce all-cause mortality and may be recommended after TIA.[25]
Diabetes control
Diabetes mellitus increases the risk of ischemic stroke by 1.5-3.7 times, and may account for at least 8% of first ischemic strokes.[25] While intensive glucose control can prevent certain complications of diabetes such as kidney damage and retinal damage, there has previously been little evidence that it decreases the risk of stroke or death.[36] However, data from 2017 suggests that metformin, pioglitazone and semaglutide may reduce stroke risk.[36]
Surgery
If the TIA affects an area that is supplied by the carotid arteries, a carotid ultrasound scan may demonstrate stenosis, or narrowing, of the carotid artery. For people with extra-cranial carotid stenosis, if 70-99% of the carotid artery is clogged, carotid endarterectomy can decrease the five-year risk of ischemic stroke by approximately half.[37] For those with extra-cranial stenosis between 50-69%, carotid endarterectomy decreases the 5-year risk of ischemic stroke by about 16%.[37] For those with extra-cranial stenosis less than 50%, carotid endarterectomy does not reduce stroke risk and may, in some cases, increase it.[37] The efficacy of carotid endarterectomy or carotid artery stenting in reducing stroke risk in patients with intra-cranial carotid artery stenosis is currently unknown.[25]
In carotid endarterectomy, a surgeon makes an incision in the neck, opens up the carotid artery, and removes the plaque occluding the blood vessel. The artery may then be repaired by adding a graft from another vessel in the body, or a woven patch. In patients who undergo carotid endarterectomy after a TIA or minor stroke, the 30-day risk of death or stroke is 7%.[37]
Carotid artery stenting is a less invasive alternative to carotid endarterectomy for patients with extra-cranial carotid artery stenosis. In this procedure, the surgeon makes a small cut in the groin and threads a small flexible tube, called a catheter, into the patient's carotid artery. A balloon is inflated at the site of stenosis, opening up the clogged artery to allow for increased blood flow to the brain. To keep the vessel open, a small wire mesh coil, called a stent, may be inflated along with the balloon. The stent remains in place, and the balloon is removed.
In patients over the age of 70, carotid endarterectomy is associated with fewer postoperative deaths or strokes than carotid artery stenting.[38] In younger patients, there is no significant difference in outcomes between carotid endarterectomy and carotid artery stenting.[38] People who undergo carotid endarterectomy or carotid artery stenting for stroke prevention are medically managed with antiplatelets, statins, and other interventions as well.[25]
Prognosis
Without treatment, the risk of an ischemic stroke in the three months after a TIA is about 20% with the greatest risk occurring within two days of the TIA.[10] Other sources cite that 10% of TIAs will develop into a stroke within 90 days, half of which will occur in the first two days following the TIA.[39] Treatment and preventative measures after a TIA (for example treating elevated blood pressure) can reduce the subsequent risk of an ischemic stroke by about 80%.[10] The risk of a stroke occurring after a TIA can be predicted using the ABCD² score. One limitation of the ABCD² score is that it does not reliably predict the level of carotid artery stenosis, which is a major cause of stroke in TIA patients. The patient's age is the most reliable risk factor in predicting any level of carotid stenosis in transient ischemic attack.[40] The ABCD2 score is no longer recommended for triage (to decide between outpatient management versus hospital admission) of those with a suspected TIA due to these limitations.[10]
Epidemiology
With the difficulty in diagnosing a TIA due to its nonspecific symptoms of neurologic dysfunction at presentation and a differential including many mimics, the exact incidence of the disease is unclear. It is currently estimated to have an incidence of approximately 200,000 to 500,000 cases per year in the US according to the American Heart Association.[4] TIA incidence trends similarly to stroke, such that incidence varies with age, gender, and different race/ethnicity populations.[4][41][9] Associated risk factors include age greater than or equal to 60, blood pressure greater than or equal to 140 systolic or 90 diastolic, and comorbid diseases, such as diabetes, hypertension, atherosclerosis, and atrial fibrillation. It is thought that approximately 15 to 30 percent of strokes have a preceding TIA episode associated.[9][12][42]
References
- ↑ Arning, C; Grzyska, U (2004-07-20). "Color Doppler imaging of cervicocephalic fibromuscular dysplasia". Cardiovascular ultrasound. 2: 7. doi:10.1186/1476-7120-2-7. PMID 15265239.
- 1 2 3 4 5 6 7 "Transient Ischemic Attack Information Page | National Institute of Neurological Disorders and Stroke". www.ninds.nih.gov. Archived from the original on 9 April 2021. Retrieved 25 May 2021.
- 1 2 3 4 5 6 7 8 9 10 11 12 Panuganti, KK; Tadi, P; Lui, F (January 2021). "Transient Ischemic Attack". PMID 29083778.
{{cite journal}}: Cite journal requires|journal=(help) - 1 2 3 4 5 6 7 8 9 10 11 12 13 Easton, J. Donald; Saver, Jeffrey L.; Albers, Gregory W.; Alberts, Mark J.; Chaturvedi, Seemant; Feldmann, Edward; Hatsukami, Thomas S.; Higashida, Randall T.; Johnston, S. Claiborne; Kidwell, Chelsea S.; Lutsep, Helmi L.; Miller, Elaine; Sacco, Ralph L.; American Heart Association; American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; Interdisciplinary Council on Peripheral Vascular Disease (June 2009). "Definition and Evaluation of Transient Ischemic Attack: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease: The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists". Stroke. 40 (6): 2276–2293. doi:10.1161/STROKEAHA.108.192218. PMID 19423857.
- ↑ Gattellari, Melina; Goumas, Chris; Biost, Frances Garden M.; Worthington, John M. (January 2012). "Relative Survival After Transient Ischaemic Attack: Results From the Program of Research Informing Stroke Management (PRISM) Study". Stroke. 43 (1): 79–85. doi:10.1161/STROKEAHA.111.636233. PMID 22076008. S2CID 16722015. Lay summary.
{{cite journal}}: Cite uses deprecated parameter|lay-url=(help) - 1 2 Ton, Joey (31 May 2021). "#291 Early dual antiplatelet therapy after minor stroke: Does it take two to tango?". CFPCLearn. Archived from the original on 25 March 2023. Retrieved 15 June 2023.
- 1 2 Ferri, Fred F. (2019-06-01). Ferri's Clinical Advisor 2020 E-Book: 5 Books in 1. Elsevier Health Sciences. p. 1394. ISBN 978-0-323-67977-0. Archived from the original on 2021-08-29. Retrieved 2021-05-25.
- ↑ Rolak, Loren A. (1993). Neurology Secrets. Hanley & Belfus. p. 398. ISBN 978-1-56053-056-5. Archived from the original on 2021-08-29. Retrieved 2021-05-25.
- 1 2 3 4 5 Panuganti, Kiran K.; Tadi, Prasanna; Lui, Forshing (2020). "Transient Ischemic Attack". StatPearls. Archived from the original on 2021-01-19. Retrieved 2021-04-25.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 Solomon, Caren G.; Amarenco, Pierre (14 May 2020). "Transient Ischemic Attack". New England Journal of Medicine. 382 (20): 1933–1941. doi:10.1056/NEJMcp1908837. PMID 32402163.
- ↑ Amort, Margareth; Fluri, Felix; Schäfer, Juliane; Weisskopf, Florian; Katan, Mira; Burow, Annika; Bucher, Heiner C.; Bonati, Leo H.; Lyrer, Philippe A.; Engelter, Stefan T. (2011). "Transient Ischemic Attack versus Transient Ischemic Attack Mimics: Frequency, Clinical Characteristics and Outcome" (PDF). Cerebrovascular Diseases. 32 (1): 57–64. doi:10.1159/000327034. PMID 21613786. S2CID 43769238. Archived (PDF) from the original on 2020-09-23. Retrieved 2021-04-25.
- 1 2 3 4 5 6 7 8 9 10 11 Simmons BB, Cirignano B, Gadegbeku AB (Sep 2012). "Transient ischemic attack: Part I. Diagnosis and evaluation". Am Fam Physician. 86 (6): 521–6. PMID 23062043. Archived from the original on 2021-08-29. Retrieved 2021-04-25.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - 1 2 3 4 5 6 7 8 9 10 11 12 13 Smith, Wade S.; Johnston, S. Claiborne; Hemphill, III, J. Claude (2019). "Cerebrovascular Diseases". In Jameson, J. Larry; Fauci, Anthony S.; Kasper, Dennis L.; Hauser, Stephen L.; Longo, Dan L.; Loscalzo, Joseph (eds.). Harrison's Principles of Internal Medicine (20th ed.). Archived from the original on 2021-02-25. Retrieved 2021-04-25.
- 1 2 3 4 5 6 Wong, Ka Sing; Caplan, Louis R.; Kim, Jong S. (2017). "Stroke Mechanisms". Intracranial Atherosclerosis: Pathophysiology, Diagnosis and Treatment. Frontiers of Neurology and Neuroscience. Vol. 40. pp. 58–71. doi:10.1159/000448302. ISBN 978-3-318-02758-7. PMID 27960181.
- 1 2 Boehme, Amelia K.; Esenwa, Charles; Elkind, Mitchell S.V. (3 February 2017). "Stroke Risk Factors, Genetics, and Prevention". Circulation Research. 120 (3): 472–495. doi:10.1161/CIRCRESAHA.116.308398. PMC 5321635. PMID 28154098.
- 1 2 3 Adams, Harold P.; del Zoppo, Gregory; Alberts, Mark J.; Bhatt, Deepak L.; Brass, Lawrence; Furlan, Anthony; Grubb, Robert L.; Higashida, Randall T.; Jauch, Edward C.; Kidwell, Chelsea; Lyden, Patrick D.; Morgenstern, Lewis B.; Qureshi, Adnan I.; Rosenwasser, Robert H.; Scott, Phillip A.; Wijdicks, Eelco F.M.; American Heart Association; American Stroke Association Stroke Council; Clinical Cardiology Council; Cardiovascular Radiology and Intervention Council; Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups (May 2007). "Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/ American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists". Stroke. 38 (5): 1655–1711. doi:10.1161/STROKEAHA.107.181486. PMID 17431204.
- ↑ Redgrave JN, Coutts SB, Schulz UG, Briley D, Rothwell PM (2007). "Systematic review of associations between the presence of acute ischemic lesions on diffusion-weighted imaging and clinical predictors of early stroke risk after transient ischemic attack". Stroke. 38 (5): 1482–1488. doi:10.1161/strokeaha.106.477380. PMID 17379821.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - 1 2 3 "Final Recommendation Statement: Carotid Artery Stenosis: Screening". United States Preventive Services Taskforce. 8 July 2014. Archived from the original on 29 January 2020. Retrieved 25 April 2021.
- ↑ Butler, Sonia & Crowfoot, Gary & Quain, Debbie & Davey, Andrew & Magin, Parker & Maguire, Jane. (2017). "Opening the Door to Funny Turns: A Constructivist Thematic Analysis of Patient Narratives after TIA". Public Health Research. 7. 62–72.
- ↑ "Transient Ischemic Attack". Archived from the original on 2019-01-13. Retrieved 2021-04-25.
- ↑ Shah SH, Saver JL, Kidwell CS, Albers GW, Rothwell PM, Ay H, Koroshetz WJ, Inatomi Y, Uchino M, Demchuk AM, Coutts SB, Purroy F, Alvarez-Sabin JS, Sander D, Sander K, Restrepo L, Wityk RJ, Marx JJ, Easton JD (2007). "A multicenter pooled, patient-level data analysis of diffusion-weighted MRI in TIA patients". Stroke. 38 (2): 463. S2CID 78309677.
{{cite journal}}: CS1 maint: multiple names: authors list (link) in "Abstracts From the 2007 International Stroke Conference". Stroke. 38 (2): 453–607. February 2007. doi:10.1161/str.38.2.453. - 1 2 "Transient ischaemic attack (TIA) - Prevention - NHS Choices". Nhs.uk. 2014-10-15. Archived from the original on 2015-09-06. Retrieved 2015-08-19.
- ↑ Mohan, Keerthi M.; Wolfe, Charles D.A.; Rudd, Anthony G.; Heuschmann, Peter U.; Kolominsky-Rabas, Peter L.; Grieve, Andrew P. (May 2011). "Risk and Cumulative Risk of Stroke Recurrence: A Systematic Review and Meta-Analysis". Stroke. 42 (5): 1489–1494. doi:10.1161/STROKEAHA.110.602615. PMID 21454819. S2CID 18230964.
- ↑ Lawrence, Maggie; Pringle, Jan; Kerr, Susan; Booth, Joanne; Govan, Lindsay; Roberts, Nicola J. (20 March 2015). "Multimodal Secondary Prevention Behavioral Interventions for TIA and Stroke: A Systematic Review and Meta-Analysis". PLOS ONE. 10 (3): e0120902. Bibcode:2015PLoSO..1020902L. doi:10.1371/journal.pone.0120902. PMC 4368743. PMID 25793643.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Kernan, Walter N.; Ovbiagele, Bruce; Black, Henry R.; Bravata, Dawn M.; Chimowitz, Marc I.; Ezekowitz, Michael D.; Fang, Margaret C.; Fisher, Marc; Furie, Karen L.; Heck, Donald V.; Johnston, S. Claiborne (Clay); Kasner, Scott E.; Kittner, Steven J.; Mitchell, Pamela H.; Rich, Michael W.; Richardson, DeJuran; Schwamm, Lee H.; Wilson, John A.; American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on Peripheral Vascular Disease (July 2014). "Guidelines for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association". Stroke. 45 (7): 2160–2236. doi:10.1161/STR.0000000000000024. PMID 24788967.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - 1 2 Hao, Qiukui; Tampi, Malavika; O’Donnell, Martin; Foroutan, Farid; Siemieniuk, Reed AC; Guyatt, Gordon (18 December 2018). "Clopidogrel plus aspirin versus aspirin alone for acute minor ischaemic stroke or high risk transient ischaemic attack: systematic review and meta-analysis". BMJ. 363: k5108. doi:10.1136/bmj.k5108. PMC 6298178. PMID 30563866.
- ↑ Rothwell, Peter M; Algra, Ale; Chen, Zhengming; Diener, Hans-Christoph; Norrving, Bo; Mehta, Ziyah (2016-07-23). "Effects of aspirin on risk and severity of early recurrent stroke after transient ischaemic attack and ischaemic stroke: time-course analysis of randomised trials". The Lancet. 388 (10042): 365–375. doi:10.1016/S0140-6736(16)30468-8. PMC 5321490. PMID 27209146.
- 1 2 López-López, José A; Sterne, Jonathan A C; Thom, Howard H Z; Higgins, Julian P T; Hingorani, Aroon D; Okoli, George N; Davies, Philippa A; Bodalia, Pritesh N; Bryden, Peter A; Welton, Nicky J; Hollingworth, William; Caldwell, Deborah M; Savović, Jelena; Dias, Sofia; Salisbury, Chris; Eaton, Diane; Stephens-Boal, Annya; Sofat, Reecha (28 November 2017). "Oral anticoagulants for prevention of stroke in atrial fibrillation: systematic review, network meta-analysis, and cost effectiveness analysis". BMJ. 359: j5058. doi:10.1136/bmj.j5058. PMC 5704695. PMID 29183961.
- ↑ Shoamanesh, Ashkan; Charidimou, Andreas; Sharma, Mukul; Hart, Robert G. (December 2017). "Should Patients With Ischemic Stroke or Transient Ischemic Attack With Atrial Fibrillation and Microbleeds Be Anticoagulated?". Stroke. 48 (12): 3408–3412. doi:10.1161/STROKEAHA.117.018467. PMID 29114097. S2CID 3831870.
- ↑ Proietti, Marco; Romanazzi, Imma; Romiti, Giulio Francesco; Farcomeni, Alessio; Lip, Gregory Y.H. (January 2018). "Real-World Use of Apixaban for Stroke Prevention in Atrial Fibrillation: A Systematic Review and Meta-Analysis". Stroke. 49 (1): 98–106. doi:10.1161/STROKEAHA.117.018395. hdl:2434/748104. PMID 29167388. S2CID 204046043.
- ↑ Reboussin, David M.; Allen, Norrina B.; Griswold, Michael E.; Guallar, Eliseo; Hong, Yuling; Lackland, Daniel T.; Miller, Edgar (Pete) R.; Polonsky, Tamar; Thompson-Paul, Angela M. (2017-11-13). "Systematic Review for the 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines". Journal of the American College of Cardiology. 71 (19): 2176–2198. doi:10.1016/j.jacc.2017.11.004. PMID 29146534.
- ↑ Katsanos, Aristeidis H.; Filippatou, Angeliki; Manios, Efstathios; Deftereos, Spyridon; Parissis, John; Frogoudaki, Alexandra; Vrettou, Agathi-Rosa; Ikonomidis, Ignatios; Pikilidou, Maria; Kargiotis, Odysseas; Voumvourakis, Konstantinos; Alexandrov, Anne W.; Alexandrov, Andrei V.; Tsivgoulis, Georgios (January 2017). "Blood Pressure Reduction and Secondary Stroke Prevention: A Systematic Review and Metaregression Analysis of Randomized Clinical Trials". Hypertension. 69 (1): 171–179. doi:10.1161/HYPERTENSIONAHA.116.08485. PMID 27802419. S2CID 42869560.
- ↑ Manktelow, Bradley N; Potter, John F (8 July 2009). "Interventions in the management of serum lipids for preventing stroke recurrence". Cochrane Database of Systematic Reviews (3): CD002091. doi:10.1002/14651858.CD002091.pub2. PMC 6664829. PMID 19588332.
- ↑ Cheng, Suk F.; Brown, Martin M. (March 2017). "Contemporary medical therapies of atherosclerotic carotid artery disease". Seminars in Vascular Surgery. 30 (1): 8–16. doi:10.1053/j.semvascsurg.2017.04.005. PMID 28818261. Archived from the original on 2021-08-29. Retrieved 2021-04-25.
- ↑ O’Regan, Christopher; Wu, Ping; Arora, Paul; Perri, Dan; Mills, Edward J. (January 2008). "Statin Therapy in Stroke Prevention: A Meta-analysis Involving 121,000 Patients". The American Journal of Medicine. 121 (1): 24–33. doi:10.1016/j.amjmed.2007.06.033. PMID 18187070.
- 1 2 Castilla-Guerra, Luis; Fernandez-Moreno, María del Carmen; Leon-Jimenez, David; Carmona-Nimo, Eduardo (2017-09-20). "Antidiabetic drugs and stroke risk. Current evidence". European Journal of Internal Medicine. 48: 1–5. doi:10.1016/j.ejim.2017.09.019. PMID 28939005.
- 1 2 3 4 Rerkasem, Amaraporn; Orrapin, Saritphat; Howard, Dominic Pj; Rerkasem, Kittipan (12 September 2020). "Carotid endarterectomy for symptomatic carotid stenosis". The Cochrane Database of Systematic Reviews. 9: CD001081. doi:10.1002/14651858.CD001081.pub4. ISSN 1469-493X. PMID 32918282. Archived from the original on 16 November 2020. Retrieved 25 April 2021.
- 1 2 Bonati, Leo H; Lyrer, Philippe; Ederle, Jörg; Featherstone, Roland; Brown, Martin M (12 September 2012). "Percutaneous transluminal balloon angioplasty and stenting for carotid artery stenosis". Cochrane Database of Systematic Reviews (9): CD000515. doi:10.1002/14651858.CD000515.pub4. PMID 22972047.
- ↑ "What is TIA?". Stroke.org. Archived from the original on 2014-10-25. Retrieved 2015-08-19.
- ↑ Mannu G. S., Kyu M. M., Bettencourt-Silva J. H., Loke Y. K., Clark A. B., Metcalf A. K., Potter J. F., Myint P. K. (2015). "Age but not ABCD2 score predicts any level of carotid stenosis in either symptomatic or asymptomatic side in transient ischaemic attack". Int J Clin Pract. 69 (9): 948–956. doi:10.1111/ijcp.12637. PMID 25832133. S2CID 24197113.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Ramirez Lucas, Kim-Tenser May A., Sanossian Nerses, Cen Steven, Wen Ge, He Shuhan, Mack William J., Towfighi Amytis (2016). "Trends in Transient Ischemic Attack Hospitalizations in the United States". Journal of the American Heart Association. 5 (9): e004026. doi:10.1161/jaha.116.004026. PMC 5079046. PMID 27664805.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Wheatley Matthew A., Ross Michael A. (2017). "Care of Neurologic Conditions in an Observation Unit". Emergency Medicine Clinics of North America. 35 (3): 603–623. doi:10.1016/j.emc.2017.03.007. PMID 28711127.
External links
| Classification | |
|---|---|
| External resources |